Download presentation
Presentation is loading. Please wait.

1
Parenteral Anticoagulant
BY : Maha khalid Supervisor : Pro Dr Seham Hafez

2
Parenteral Anticoagulant
UFH & LMWH all consist of high MW molecules that Are highly ionized (they don't absorbed from GIT they must given by IV infusion or deep SC injection. ( never IM ) LMWH UFH Fondaparinux
 LMWH. UFH. Fondaparinux.")
3
Objective of anticoagulation
To prevent death & recurrent event with acceptable rate of bleeding complications. Considering the high mortality rate (30 %) in untreated patient with suspected PE anticoagulant treatment should be consider while a waiting definitive diagnostic confirmation.
 in untreated patient with suspected PE anticoagulant treatment should be consider while a waiting definitive diagnostic confirmation.")
4
Goals of anticoagulation therapy
1-The efficacy of heparin therapy depends on achieving a critical therapeutic level of heparin within the first 24 hours of treatment. The critical therapeutic level of heparin is 1.5 times the baseline control value or the upper limit of normal range of the activated partial thromboplastin time (aPTT). This level of anticoagulation is expected to correspond to a heparin blood level of U/mL by the protamine sulfate titration assay and by the antifactor X assay.
. This level of anticoagulation is expected to correspond to a heparin blood level of U/mL by the protamine sulfate titration assay and by the antifactor X assay.")
5
UFH Vs LMWH 1-Standard heparin is comprised of an unfractionated heterogeneous mixture of polysaccharide chains with mean molecular weights ranging from to daltons. 2-LMWHs are formed by depolymerization of unfractionated heparin side chains, producing “smaller” heparin fragments, with mean molecular weights ranging from 1000 daltons to daltons.

7
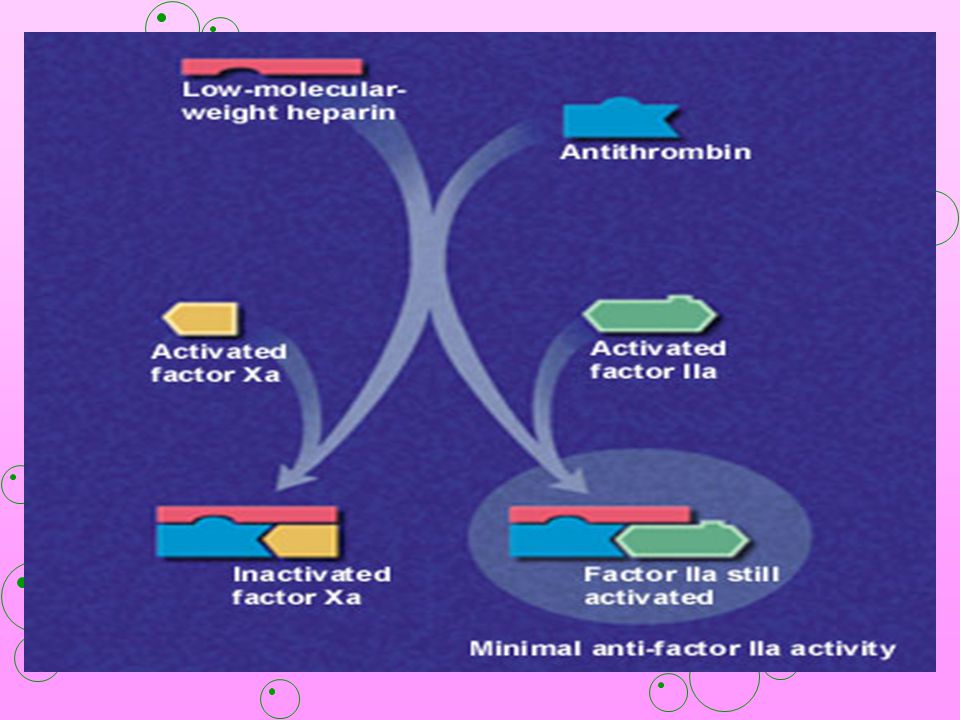
UFH Vs LMWH 1- Both types of heparin inactivate factor Xa by interacting with antithrombin (AT) 2- unfractionated heparin (UFH) is able to inactivate factor IIa through formation of a tertiary complex. 3- UFH inactivates factors IIa and Xa and affects the apTT (activated partial thromboplastin time ) 4-LMWH inhibits factor Xa and minimally affects factor IIa; thus activated partial thromboplastin time is not used to measure its anticoagulant activity
 is able to inactivate factor IIa through formation of a tertiary complex. 3- UFH inactivates factors IIa and Xa and affects the apTT (activated partial thromboplastin time ) 4-LMWH inhibits factor Xa and minimally affects factor IIa; thus activated partial thromboplastin time is not used to measure its anticoagulant activity.")
11
Anticoagulant Properties of UFH
1-Inhibits the thrombin-mediated conversion of fibrinogen to fibrin 3-Inhibits activation of fibrin stabilizing enzyme 2-Inhibits the aggregation of platelets by thrombin 4-Inhibits activated factors XII, XI, IX, X and II

12
When unfractionated heparin is used, the aPTT should not be checked until 6 h after the initial heparin bolus because an extremely high or low value during this time should not provoke any action. Does not actively lyse but is able to inhibit further thrombogenesis. Prevents reaccumulation of clot after spontaneous fibrinolysis

13
UFH weight based dose:

14
can give once or at the most
UFH Vs LMWH LMWH have potential desirable PK than heparin , they excreted renally & have longer half lives 1-Heparin half life is 1 hrs but it shorter in patient with PE It excreted by both hepatic & renal ways it would take 5 hrs ( five half lives to reach steady state , a loading dose is required to reduced the time to achieve adequate anticoagulation have more predictable dose response than UFH.,they can give once or at the most twice daily in fixed dose.

15
UFH Vs LMWH Hemorrhage Heparin LMWH risk commoner in of hemorrhage
may produce fewer hemorrhagic complication & monitoring of effect is not routinely required LMWH risk of hemorrhage is increased in those given heparin by Intermittent intravenous bolus rather than by continuous administration. Heparin commoner in patients with sever heart or liver disease ,renal disease , general debility & women aged over 60 years. The risk of hemorrhage is increased in those with prolonged clotting times Hemorrhage More less

16
LMWH Heparin HIT Thrombocytopenia
LMWH are less likely to produce thrombocytopenia this complication only in :Patient only previoulsly developed thrombocytopenia after UFH . Heparin HIT LMWH Thrombocytopenia

17
Heparin induced thrombocytopenia “ HIT “
the second type occure after 6 days of FIRSTtreatment or hours to 2-3 days with re-exposure. the first occurs after 3-5 days after initiate of treatment often result in much more reduction in plateletscount & increased risk of thromboembolism . doesnot result in complication

18
HIT ( Mechanism ) HIT is the most common drug-induced thrombocytopenia in adults, complicating 1-4% of full-dose exposures to standard heparin. Unlike other thrombocytopenias, HIT carries a high thrombotic morbidity (30-50%) and mortality (10-15%) because it is a syndrome of platelet activation. Heparin forms a complex with platelet factor 4 (PF4) which is released from platelets by platelet activation. Antibody directed against the heparin-PF4 complex binds via its Fab region. The antibody-heparin-PF4 immune complex binds to the Fc receptor on the surface of the platelet leading to activation of the platelet.
 and mortality (10-15%) because it is a syndrome of platelet activation. Heparin forms a complex with platelet factor 4 (PF4) which is released from platelets by platelet activation. Antibody directed against the heparin-PF4 complex binds via its Fab region. The antibody-heparin-PF4 immune complex binds to the Fc receptor on the surface of the platelet leading to activation of the platelet.")
20
Criteria for Diagnosing HIT

21
Complications of HIT 1-•Deep vein thrombosis• 2-Pulmonary embolism•
3-Myocardial infarction• 4-Occlusion of limb arteries (possibly resulting in amputation)• 5-Cerebrovascular accidents (stroke ) 6-Skin necrosis• 7-End-organ damage (e.g., adrenal, bowel, spleen, gallbladder or hepatic infarction; renal failure)• 8-Death
• 5-Cerebrovascular accidents (stroke ) 6-Skin necrosis• 7-End-organ damage (e.g., adrenal, bowel, spleen, gallbladder or hepatic infarction; renal failure)• 8-Death.")
22
Treatment of HIT : C/I must be stopped should be AVOIDED
1-ALL heparin (lines, flushes, heparin-coated catheters, LMWH ) should be AVOIDED Platelet transfusion (transfusion may precipitate thrombosis) warfarin in the acute phase of HIT (its use may precipitate venous gangrene and thrombosis). C/I
 should be AVOIDED. Platelet transfusion. (transfusion may precipitate thrombosis) warfarin in the acute phase of HIT. (its use may precipitate venous gangrene and thrombosis). C/I.")
23
highly specific direct in order to prevent further
[1-lepirudin (rDNA) for injection highly specific direct inhibitor of thrombin indicated as an anticoagulant for prophylaxis or treatment of thrombosis in patients with HIT and associated thromboembolic disease in order to prevent further complications. Treatment of HIT : 2-Argatroban is a synthetic direct thrombin inhibitor indicated as an anticoagulant for prophylaxis or treatment of thrombosis in patients with HIT
 for injection. highly specific direct. inhibitor of thrombin. indicated as an. anticoagulant. for prophylaxis. or treatment of. thrombosis in. patients with HIT. and associated. thromboembolic. disease. in order to prevent further. complications. Treatment of HIT : 2-Argatroban is a. synthetic direct. thrombin inhibitor. indicated as an. anticoagulant. for prophylaxis. or treatment. of thrombosis in. patients with HIT.")
24
For how long UFH &LMWH should be used ?
1-Heparin used in immediate stages of venous thrombosis & PE until the effect of warfarin become apparent . In the past it has been continued for 7-10 days but recent evidence indicate that 3-5 days of therapy maybe sufficient in many instances : this will reduce the risk of HIT which normally occurred after 6 days. 2- LMWH are used for similar length but they are give SC without loading dose & without routinely monitoring.

25
Enoxaparin Only LMWH approved by FDA for both
treatment and prophylaxis of DVT and PE. Dose Adult :DVT/PE: 1 mg/kg SC q12h or 1.5 mg/kg SC qd Prophylaxis of DVT: 30 mg SC q12h Prophylaxis in abdominal surgery: 40 mg SC qd, first dose given 2 h prior to surgery Pediatric DVT/PE: 1 mg/kg SC q 12h Interactions: Platelet inhibitors or oral anticoagulants (eg, dipyridamole , salicylates, aspirin, NSAIDs, sulfinpyrazone, ticlopidine) may increase risk of bleeding
 may increase risk of bleeding.")
26
Enoxaparin(Con”d) Pregnancy
contraindication Documented hypersensitivity; major bleeding; thrombocytopenia Pregnancy B - Usually safe but benefits must outweigh the risks Precautions If thromboembolic event occurs despite LMWH prophylaxis, discontinue drug and initiate alternate therapy; elevation of hepatic transaminases may occur but is reversible; HIT may occur; 1 mg protamine sulfate reverses effect of approximately 1 mg enoxaparin if significant bleeding complications develop

27
When LMWH will need dose adjustment :
in patient with renal failure dose adjustment according to anti-Xa level. If crcl less than 30ml/min heparin is preferred Also patient at high risk of bleeding heparin should be considering as it effect is easy to reversed. very thin or very obese patient dose adjustment According to factor Xa pregnancy.

28
FONDAPARINUX Synthetic anticoagulant that works by inhibiting factor Xa a key component involved in blood clotting. Provides highly predictable response. Bioavailability is 100%. Has a rapid onset of action and a half-life of h, allowing for sustained antithrombotic activity over 24-h period Does not affect prothrombin time or activated partial Thromboplastin time, nor does it affect platelet function Dose : 2.5 mg SC qd

29
administration of platelet inhibitors,
DRUG INTERACTIONS: None reported; increased risk of bleeding possible with concurrent administration of platelet inhibitors, oral anticoagulants, or thrombolytic agents Contraindication Documented hypersensitivity; seriously impaired kidney function or in patients who weigh <110 lb; patients given spinal anesthesia or spinal puncture Pregnancy C - Safety for use during pregnancy has not been established. Precautions When spinal anesthesia or spinal puncture used, may develop blood clot in spine , which can result in long-term or permanent paralysis

30
Finally which one is better UFH or LMWH ?

31
Several meta-analyses have indicated that:
1-LMWH is associated with less bleeding and fewer episodes of heparin- Induced thrombocytopenia Than UFH 2-patients receiving LMWH reported a higher quality of life in terms of physical and social function and sense of well-being. 3- Treatment of DVT with LMWH was more cost-effective than therapy with UFH because the length of The hospital stay was reduced by 60 to 70 percent without an increase in the cost of home health care

32
But Two recent studies of patients with DVT :
To compare the effect of LMWH given on an outpatient basis SC twice daily with that of UFH given by continuous IV infusion in the No significant different was hospital found in rates of recurrent venous thromboembolism, hemorrhagic complications, development of thrombocytopenia or mortality. LMWH were as safe and effective as UFH and most patients were managed at home immediately after diagnosis or a brief hospitalization.

33
With warfarin

34
THANK YOU

Similar presentations










 of these drugs should be the one(s) I use, and for what?>")




 V, VIII, XIII, Fibrinogen Inactive Factor Xa Common Pathway Inactive.>")







