Download presentation
Presentation is loading. Please wait.

1
Chapter 31 Antithrombotic therapy August 8, 2005

2
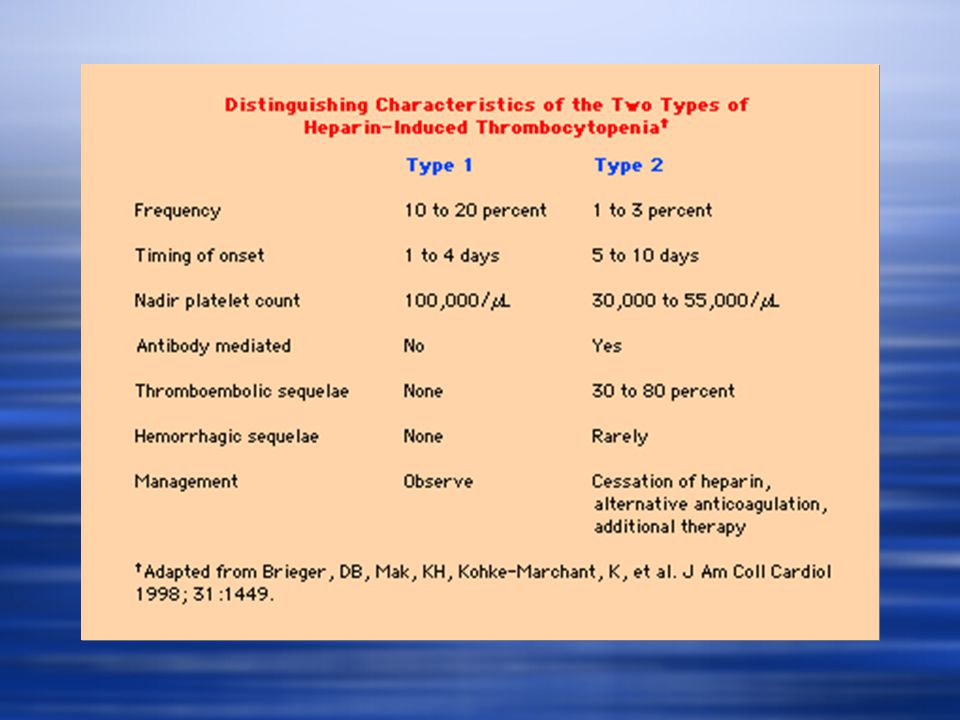
Heparin induced thrombocytopenia (HIT) Characterized by formation of antibodies against the heparin-platelet factor 4 complex, type II Type I due to direct effect of heparin on platelet activation, occurs within the first two days and often normalizes with continued heparin administration Characterized by formation of antibodies against the heparin-platelet factor 4 complex, type II Type I due to direct effect of heparin on platelet activation, occurs within the first two days and often normalizes with continued heparin administration
 Characterized by formation of antibodies against the heparin-platelet factor 4 complex, type II Type I due to direct effect of heparin on platelet activation, occurs within the first two days and often normalizes with continued heparin administration Characterized by formation of antibodies against the heparin-platelet factor 4 complex, type II Type I due to direct effect of heparin on platelet activation, occurs within the first two days and often normalizes with continued heparin administration")
4
HIT incidence Frequency of 0.3 to 3% in patients exposed to heparin for more than 4 days One randomized study of heparin vs LMWH for hip surgery prophylaxis HIT incidence was 2.7% vs 0% for those on LMWH SQ unfractionated heparin had an incidence of 0.8% for HIT with 598 consecutive medical patients Amount required can be as small as 250u from heparin flushes or heparin coated catheters Frequency of 0.3 to 3% in patients exposed to heparin for more than 4 days One randomized study of heparin vs LMWH for hip surgery prophylaxis HIT incidence was 2.7% vs 0% for those on LMWH SQ unfractionated heparin had an incidence of 0.8% for HIT with 598 consecutive medical patients Amount required can be as small as 250u from heparin flushes or heparin coated catheters

5
HIT pathophysiology IgG and IgM antibodies provoked not by heparin alone but complex of heparin and platelet factor 4 Heparin-PF4-antibody complex binds to platelet surface and leads to platelet activation that further releases PF4 causing a positive feedback loop Activated platelets aggregate and are removed prematurely from circulation leading to thrombocytopenia and frequently thrombosis IgG and IgM antibodies provoked not by heparin alone but complex of heparin and platelet factor 4 Heparin-PF4-antibody complex binds to platelet surface and leads to platelet activation that further releases PF4 causing a positive feedback loop Activated platelets aggregate and are removed prematurely from circulation leading to thrombocytopenia and frequently thrombosis

7
HIT clinical presentation Typically occurs 4 to 10 days after initiation of heparin Earlier onset seen in patients treated with heparin in preceeding 3 to 4 months Thrombocytopenia is rarely severe with platelet counts over 20k, median platelet count nadir of 60k Spontaneous bleeding is unusual Delayed onset HIT Can occur after heparin has been withdrawn, avg 9 days later, patients have high titer platelet activating antibodies in one study of 12 patients 14 patients avg time 14 days (9 to 40 days), 11 patients readmitted and treated with heparin resulting in thrombocytopenia and clinical deterioration and death in 3 patients Criteria for delayed onset HIT, 1 exposure to heparin with benign hospital course, 2 representation with venous and/or arterial thrombosis, 3 positive serological tests for heparin-induced antibodies Typically occurs 4 to 10 days after initiation of heparin Earlier onset seen in patients treated with heparin in preceeding 3 to 4 months Thrombocytopenia is rarely severe with platelet counts over 20k, median platelet count nadir of 60k Spontaneous bleeding is unusual Delayed onset HIT Can occur after heparin has been withdrawn, avg 9 days later, patients have high titer platelet activating antibodies in one study of 12 patients 14 patients avg time 14 days (9 to 40 days), 11 patients readmitted and treated with heparin resulting in thrombocytopenia and clinical deterioration and death in 3 patients Criteria for delayed onset HIT, 1 exposure to heparin with benign hospital course, 2 representation with venous and/or arterial thrombosis, 3 positive serological tests for heparin-induced antibodies
, 11 patients readmitted and treated with heparin resulting in thrombocytopenia and clinical deterioration and death in 3 patients Criteria for delayed onset HIT, 1 exposure to heparin with benign hospital course, 2 representation with venous and/or arterial thrombosis, 3 positive serological tests for heparin-induced antibodies Typically occurs 4 to 10 days after initiation of heparin Earlier onset seen in patients treated with heparin in preceeding 3 to 4 months Thrombocytopenia is rarely severe with platelet counts over 20k, median platelet count nadir of 60k Spontaneous bleeding is unusual Delayed onset HIT Can occur after heparin has been withdrawn, avg 9 days later, patients have high titer platelet activating antibodies in one study of 12 patients 14 patients avg time 14 days (9 to 40 days), 11 patients readmitted and treated with heparin resulting in thrombocytopenia and clinical deterioration and death in 3 patients Criteria for delayed onset HIT, 1 exposure to heparin with benign hospital course, 2 representation with venous and/or arterial thrombosis, 3 positive serological tests for heparin-induced antibodies")
9
HIT thrombosis 89% of 9 patients with HIT developed thrombosis (7 venous and 1 arterial) after hip surgery Retrospective review of 127 with HIT, 78 (61%) patients venous thrombosis and 18 (14%) patients arterial thrombosis, P/E manifested occurred in 25% of these patients, patient with isolated thrombocytopenia had a 30 day risk of thrombosis of 53% 89% of 9 patients with HIT developed thrombosis (7 venous and 1 arterial) after hip surgery Retrospective review of 127 with HIT, 78 (61%) patients venous thrombosis and 18 (14%) patients arterial thrombosis, P/E manifested occurred in 25% of these patients, patient with isolated thrombocytopenia had a 30 day risk of thrombosis of 53%
 after hip surgery Retrospective review of 127 with HIT, 78 (61%) patients venous thrombosis and 18 (14%) patients arterial thrombosis, P/E manifested occurred in 25% of these patients, patient with isolated thrombocytopenia had a 30 day risk of thrombosis of 53% 89% of 9 patients with HIT developed thrombosis (7 venous and 1 arterial) after hip surgery Retrospective review of 127 with HIT, 78 (61%) patients venous thrombosis and 18 (14%) patients arterial thrombosis, P/E manifested occurred in 25% of these patients, patient with isolated thrombocytopenia had a 30 day risk of thrombosis of 53%")
10
HIT diagnostic testing Clinical diagnosis Unexplained thrombocytopenia, thrombosis associated with thrombocytopenia, or normal platelet count that has fallen more than 50% Serotonin release assay 14C-serotonin release assay is gold standard Normal donor platelets labeled with C14-serotonin, washed, then patient serum is added along with low and high concentration heparin Positive test occurs with release of C14-serotonin with therapeutic concentrations of heparin (0.1u/Ml) Very expensive Heparin induced platelet aggregation Very specific (>90%) but with low sensitivity Solid phase immunoassay Not a functional assay Sensitive >91% but not specific as many antibody positive patients do not develop clinical HIT Best used in conjunction with one of the other tests Clinical diagnosis Unexplained thrombocytopenia, thrombosis associated with thrombocytopenia, or normal platelet count that has fallen more than 50% Serotonin release assay 14C-serotonin release assay is gold standard Normal donor platelets labeled with C14-serotonin, washed, then patient serum is added along with low and high concentration heparin Positive test occurs with release of C14-serotonin with therapeutic concentrations of heparin (0.1u/Ml) Very expensive Heparin induced platelet aggregation Very specific (>90%) but with low sensitivity Solid phase immunoassay Not a functional assay Sensitive >91% but not specific as many antibody positive patients do not develop clinical HIT Best used in conjunction with one of the other tests
 Very expensive Heparin induced platelet aggregation Very specific (>90%) but with low sensitivity Solid phase immunoassay Not a functional assay Sensitive >91% but not specific as many antibody positive patients do not develop clinical HIT Best used in conjunction with one of the other tests Clinical diagnosis Unexplained thrombocytopenia, thrombosis associated with thrombocytopenia, or normal platelet count that has fallen more than 50% Serotonin release assay 14C-serotonin release assay is gold standard Normal donor platelets labeled with C14-serotonin, washed, then patient serum is added along with low and high concentration heparin Positive test occurs with release of C14-serotonin with therapeutic concentrations of heparin (0.1u/Ml) Very expensive Heparin induced platelet aggregation Very specific (>90%) but with low sensitivity Solid phase immunoassay Not a functional assay Sensitive >91% but not specific as many antibody positive patients do not develop clinical HIT Best used in conjunction with one of the other tests")
11
HIT thrombosis Other clinical manifestations Venous limb gangrene (distal ischemic necrosis followed by DVT) Cerebral sinus thrombosis Upper extremity DVT 260 cases, upper extremity DVT present in 5.4% of cases, all occurred in patients with central venous catheters and at catheter site Arterial thrombosis Stroke MI Limb ischemia from peripheral artery occlusion Organ infarction (mesentery, kidney) Skin necrosis Similar to warfarin induced skin necrosis but patients not deficient in protein C/S or antithrombin Other clinical manifestations Venous limb gangrene (distal ischemic necrosis followed by DVT) Cerebral sinus thrombosis Upper extremity DVT 260 cases, upper extremity DVT present in 5.4% of cases, all occurred in patients with central venous catheters and at catheter site Arterial thrombosis Stroke MI Limb ischemia from peripheral artery occlusion Organ infarction (mesentery, kidney) Skin necrosis Similar to warfarin induced skin necrosis but patients not deficient in protein C/S or antithrombin
 Cerebral sinus thrombosis Upper extremity DVT 260 cases, upper extremity DVT present in 5.4% of cases, all occurred in patients with central venous catheters and at catheter site Arterial thrombosis Stroke MI Limb ischemia from peripheral artery occlusion Organ infarction (mesentery, kidney) Skin necrosis Similar to warfarin induced skin necrosis but patients not deficient in protein C/S or antithrombin Other clinical manifestations Venous limb gangrene (distal ischemic necrosis followed by DVT) Cerebral sinus thrombosis Upper extremity DVT 260 cases, upper extremity DVT present in 5.4% of cases, all occurred in patients with central venous catheters and at catheter site Arterial thrombosis Stroke MI Limb ischemia from peripheral artery occlusion Organ infarction (mesentery, kidney) Skin necrosis Similar to warfarin induced skin necrosis but patients not deficient in protein C/S or antithrombin")
12
HIT prevention Low incidence of heparin dependent IgG antibodies 2.2% vs. 7.8% with use of LMWH Warfarin should not be given to HIT patients until thrombocytopenia resolves and therapy should be bridged by argatroban or hirudin, LMWH should not be substituted after HIT Low incidence of heparin dependent IgG antibodies 2.2% vs. 7.8% with use of LMWH Warfarin should not be given to HIT patients until thrombocytopenia resolves and therapy should be bridged by argatroban or hirudin, LMWH should not be substituted after HIT

13
HIT treatment Immediate cessation of all exposure to heparin Consider direct thrombin inhibitor lepirudin or argatroban to bridge anticoagulation therapy Warfarin Start when patient stably anticoagulated with a thrombin specific inhibitor and platelet count increased to 100k Warfarin therapy alone may increase risk of venous limb gangrene in patients with DVT High initial doses >= 10 mg should be avoided to minimize transient hypercoagulable state induced by decline in protein C levels Anticoagulation should be continued for 2 to 3 months Immediate cessation of all exposure to heparin Consider direct thrombin inhibitor lepirudin or argatroban to bridge anticoagulation therapy Warfarin Start when patient stably anticoagulated with a thrombin specific inhibitor and platelet count increased to 100k Warfarin therapy alone may increase risk of venous limb gangrene in patients with DVT High initial doses >= 10 mg should be avoided to minimize transient hypercoagulable state induced by decline in protein C levels Anticoagulation should be continued for 2 to 3 months

14
Direct thrombin inhibitors Hirudin derivative Lepirudin, renally excreted and monitored using aPTT, initial bolus of 0.4mg/kg followed by infusion of 0.15mg/kg/hr to keep aPTT 1.5 to 2.5 greater than baseline Lepirudin approved for treatment of HIT Lepirudin as safe and effective as heparin for unstable angina, adjunct to thrombolytic therapy, prophylaxis and treatment of VTE Hirulogs Bivalirudin (angiomax) monitored by ACT to maintain >350 secs Only direct thrombin inhibitor approved for acute coronary syndromes Decrease rate of clinically significant bleeding compared to heparin 3.5% vs. 9.3%. Hirudin derivative Lepirudin, renally excreted and monitored using aPTT, initial bolus of 0.4mg/kg followed by infusion of 0.15mg/kg/hr to keep aPTT 1.5 to 2.5 greater than baseline Lepirudin approved for treatment of HIT Lepirudin as safe and effective as heparin for unstable angina, adjunct to thrombolytic therapy, prophylaxis and treatment of VTE Hirulogs Bivalirudin (angiomax) monitored by ACT to maintain >350 secs Only direct thrombin inhibitor approved for acute coronary syndromes Decrease rate of clinically significant bleeding compared to heparin 3.5% vs. 9.3%.
 monitored by ACT to maintain >350 secs Only direct thrombin inhibitor approved for acute coronary syndromes Decrease rate of clinically significant bleeding compared to heparin 3.5% vs. 9.3%..")
15
Small molecule direct thrombin inhibitors Argatroban Only one FDA approved Borderline increased risk of MI and lower rates of major bleeding Hepatically cleared 2ug/kg/min adjusted to maintian aPTT at 1.5 to 3 times baseline, 0.5ug/kg/min for patients with hepatic dysfunction Ximelagatran Oral bioavailability of 18 to 24% Transformed to melagatran Compared to dalteparin, combination of ximelagatran and melagatran reduced frequency of VTE in ortho patients from 28.2% to 15.1% Dosing not influenced by age, gender, or weight and does not require monitoring Ximelagatran vs. warfarin reduced incidence of VTE and death 20.3% vs. 27.6% with total knee replacement patients and no increased risk of bleeding but elevated transaminases were identified 6.4% vs 1.2% (placebo) Argatroban Only one FDA approved Borderline increased risk of MI and lower rates of major bleeding Hepatically cleared 2ug/kg/min adjusted to maintian aPTT at 1.5 to 3 times baseline, 0.5ug/kg/min for patients with hepatic dysfunction Ximelagatran Oral bioavailability of 18 to 24% Transformed to melagatran Compared to dalteparin, combination of ximelagatran and melagatran reduced frequency of VTE in ortho patients from 28.2% to 15.1% Dosing not influenced by age, gender, or weight and does not require monitoring Ximelagatran vs. warfarin reduced incidence of VTE and death 20.3% vs. 27.6% with total knee replacement patients and no increased risk of bleeding but elevated transaminases were identified 6.4% vs 1.2% (placebo)
 Argatroban Only one FDA approved Borderline increased risk of MI and lower rates of major bleeding Hepatically cleared 2ug/kg/min adjusted to maintian aPTT at 1.5 to 3 times baseline, 0.5ug/kg/min for patients with hepatic dysfunction Ximelagatran Oral bioavailability of 18 to 24% Transformed to melagatran Compared to dalteparin, combination of ximelagatran and melagatran reduced frequency of VTE in ortho patients from 28.2% to 15.1% Dosing not influenced by age, gender, or weight and does not require monitoring Ximelagatran vs. warfarin reduced incidence of VTE and death 20.3% vs. 27.6% with total knee replacement patients and no increased risk of bleeding but elevated transaminases were identified 6.4% vs 1.2% (placebo).")
16
HIT use of heparin later Brief use of heparin during cardiopulmonary bypass has been successful But consider if alternative anticoagulants are available Prove that HIT antibodies are not detectable Restrict use of heparin to operative procedure itself Use alternative anticoagulant pre/post op (eg, lepirudin, warfarin) Brief use of heparin during cardiopulmonary bypass has been successful But consider if alternative anticoagulants are available Prove that HIT antibodies are not detectable Restrict use of heparin to operative procedure itself Use alternative anticoagulant pre/post op (eg, lepirudin, warfarin)
 Brief use of heparin during cardiopulmonary bypass has been successful But consider if alternative anticoagulants are available Prove that HIT antibodies are not detectable Restrict use of heparin to operative procedure itself Use alternative anticoagulant pre/post op (eg, lepirudin, warfarin)")
17
Factor Xa inhibitors Fondaparinux (arixtra) Inhibit thrombin generation Reduced odds of VTE when compared to enoxaparin in major othropedic cases (6.8% vs. 13.7%) but at the cost of increased major bleeding events (2.7% vs. 1.7%) Patients with acute symptomatic pulmonary embolism no significant difference in recurrent thromboembolism (3.8% vs. 5%) and major bleeding (1.3% and 1.1%) Fondaparinux (arixtra) Inhibit thrombin generation Reduced odds of VTE when compared to enoxaparin in major othropedic cases (6.8% vs. 13.7%) but at the cost of increased major bleeding events (2.7% vs. 1.7%) Patients with acute symptomatic pulmonary embolism no significant difference in recurrent thromboembolism (3.8% vs. 5%) and major bleeding (1.3% and 1.1%)
 but at the cost of increased major bleeding events (2.7% vs. 1.7%) Patients with acute symptomatic pulmonary embolism no significant difference in recurrent thromboembolism (3.8% vs. 5%) and major bleeding (1.3% and 1.1%) Fondaparinux (arixtra) Inhibit thrombin generation Reduced odds of VTE when compared to enoxaparin in major othropedic cases (6.8% vs. 13.7%) but at the cost of increased major bleeding events (2.7% vs. 1.7%) Patients with acute symptomatic pulmonary embolism no significant difference in recurrent thromboembolism (3.8% vs. 5%) and major bleeding (1.3% and 1.1%).")
18
Antiplatelet agents Aspirin Permanently inactivates cyclooxygenase activity of prostaglandin H synthase-1 and 2 Short half-life but able to completely inhibit platelet thromboxane A2 production Equally effective in low doses (50 to 100 mg/day) vs. high doses (900-1500 mg/day) Ticlopidine and clopidogrel Selectively inhibit ADP-induced platelet aggregation Ticlopidine effectively reduces mortality in claudicants by 29.1% Potential side effects include bone marrow suppresion, aplastic anemia, and thrombocytopenic purpura Clopidogrel six time more potent than ticlopidine and has a better safety profile, at 50 to 100 mg, requires 4 to 7 days to reach steady state, loading doses of 300 mg may result in more rapid effectiveness Bleeding risk similar to ASA and ASA is more likely to cause GI bleeding Aspirin Permanently inactivates cyclooxygenase activity of prostaglandin H synthase-1 and 2 Short half-life but able to completely inhibit platelet thromboxane A2 production Equally effective in low doses (50 to 100 mg/day) vs. high doses (900-1500 mg/day) Ticlopidine and clopidogrel Selectively inhibit ADP-induced platelet aggregation Ticlopidine effectively reduces mortality in claudicants by 29.1% Potential side effects include bone marrow suppresion, aplastic anemia, and thrombocytopenic purpura Clopidogrel six time more potent than ticlopidine and has a better safety profile, at 50 to 100 mg, requires 4 to 7 days to reach steady state, loading doses of 300 mg may result in more rapid effectiveness Bleeding risk similar to ASA and ASA is more likely to cause GI bleeding
 Ticlopidine and clopidogrel Selectively inhibit ADP-induced platelet aggregation Ticlopidine effectively reduces mortality in claudicants by 29.1% Potential side effects include bone marrow suppresion, aplastic anemia, and thrombocytopenic purpura Clopidogrel six time more potent than ticlopidine and has a better safety profile, at 50 to 100 mg, requires 4 to 7 days to reach steady state, loading doses of 300 mg may result in more rapid effectiveness Bleeding risk similar to ASA and ASA is more likely to cause GI bleeding Aspirin Permanently inactivates cyclooxygenase activity of prostaglandin H synthase-1 and 2 Short half-life but able to completely inhibit platelet thromboxane A2 production Equally effective in low doses (50 to 100 mg/day) vs. high doses ( mg/day) Ticlopidine and clopidogrel Selectively inhibit ADP-induced platelet aggregation Ticlopidine effectively reduces mortality in claudicants by 29.1% Potential side effects include bone marrow suppresion, aplastic anemia, and thrombocytopenic purpura Clopidogrel six time more potent than ticlopidine and has a better safety profile, at 50 to 100 mg, requires 4 to 7 days to reach steady state, loading doses of 300 mg may result in more rapid effectiveness Bleeding risk similar to ASA and ASA is more likely to cause GI bleeding.")
19
Antiplatelet agents Clopidogrel In patients with PVD, recent stroke, or recent MI reduced risk of stroke, MI or vascular death by 23.8% compared to ASA (3.71% compared to 4.86%) In patients with acute coronary syndromes with ST segment elevation, combination of ASA and clopidrogrel reduced incidence of CV death, non- fatal MI or stroke from 11.4% to 9.3%, this came at the cost of major bleeding from GI and puncture sites Compared to placebo combination of ASA and clopidogrel found to increase risk of bleeding (24% vs. 42%) without reduction in thrombotic events in patients with PTFE hemodialysis grafts Abciximab GP-IIb/IIIa inhibitor (inhibits fibrinogen binding) reduces rate of death, MI, or urgent revascularization in patients undergoing PCI as well as a reduction in 1 year mortality When used in conjunction with carefully managed heparin and early removal of arterial sheaths, major bleeding rates are similar to the use of heparin alone May be associated with thrombocytopenia Clopidogrel In patients with PVD, recent stroke, or recent MI reduced risk of stroke, MI or vascular death by 23.8% compared to ASA (3.71% compared to 4.86%) In patients with acute coronary syndromes with ST segment elevation, combination of ASA and clopidrogrel reduced incidence of CV death, non- fatal MI or stroke from 11.4% to 9.3%, this came at the cost of major bleeding from GI and puncture sites Compared to placebo combination of ASA and clopidogrel found to increase risk of bleeding (24% vs. 42%) without reduction in thrombotic events in patients with PTFE hemodialysis grafts Abciximab GP-IIb/IIIa inhibitor (inhibits fibrinogen binding) reduces rate of death, MI, or urgent revascularization in patients undergoing PCI as well as a reduction in 1 year mortality When used in conjunction with carefully managed heparin and early removal of arterial sheaths, major bleeding rates are similar to the use of heparin alone May be associated with thrombocytopenia
 without reduction in thrombotic events in patients with PTFE hemodialysis grafts Abciximab GP-IIb/IIIa inhibitor (inhibits fibrinogen binding) reduces rate of death, MI, or urgent revascularization in patients undergoing PCI as well as a reduction in 1 year mortality When used in conjunction with carefully managed heparin and early removal of arterial sheaths, major bleeding rates are similar to the use of heparin alone May be associated with thrombocytopenia Clopidogrel In patients with PVD, recent stroke, or recent MI reduced risk of stroke, MI or vascular death by 23.8% compared to ASA (3.71% compared to 4.86%) In patients with acute coronary syndromes with ST segment elevation, combination of ASA and clopidrogrel reduced incidence of CV death, non- fatal MI or stroke from 11.4% to 9.3%, this came at the cost of major bleeding from GI and puncture sites Compared to placebo combination of ASA and clopidogrel found to increase risk of bleeding (24% vs. 42%) without reduction in thrombotic events in patients with PTFE hemodialysis grafts Abciximab GP-IIb/IIIa inhibitor (inhibits fibrinogen binding) reduces rate of death, MI, or urgent revascularization in patients undergoing PCI as well as a reduction in 1 year mortality When used in conjunction with carefully managed heparin and early removal of arterial sheaths, major bleeding rates are similar to the use of heparin alone May be associated with thrombocytopenia.")
20
Antiplatelet agents Consensus statement that ASA 325 mg/day be started preoperatively for all prosthetic conduits; grafts to the tibial- peroneal arteries; complex reconstructions requiring composite grafts or endarterectomy; and suboptimal bypasses with limited runoff or requiring a compromised conduit Combination of warfarin and ASA to maintain an INR of 2 to 3 improved three year primary graft patency and limb salvage rate of 74% and 81% respectively compared with 51% and 31% alone Consensus statement that ASA 325 mg/day be started preoperatively for all prosthetic conduits; grafts to the tibial- peroneal arteries; complex reconstructions requiring composite grafts or endarterectomy; and suboptimal bypasses with limited runoff or requiring a compromised conduit Combination of warfarin and ASA to maintain an INR of 2 to 3 improved three year primary graft patency and limb salvage rate of 74% and 81% respectively compared with 51% and 31% alone

21
Reversal of anticoagulants Unfractionated heparin Protamine 1 mg per 100 units, risks bradycardia and hypotension Allergic reactions due to previous exposure to protamine containing insulin, vasectomy and fish allergies LMWH Protamine less effective due to shorter heparin chains Normal dosing acutely reverses 42% of factor Xa activity and 92% of anti-factor IIa actvity Warfarin Oral vitamin K reduces INR in 24 hrs Low dose IV doses effective (0.5 to 2.5mg), higher doses (>10mg) associated with temporary warfarin resistance on reintroduction Unfractionated heparin Protamine 1 mg per 100 units, risks bradycardia and hypotension Allergic reactions due to previous exposure to protamine containing insulin, vasectomy and fish allergies LMWH Protamine less effective due to shorter heparin chains Normal dosing acutely reverses 42% of factor Xa activity and 92% of anti-factor IIa actvity Warfarin Oral vitamin K reduces INR in 24 hrs Low dose IV doses effective (0.5 to 2.5mg), higher doses (>10mg) associated with temporary warfarin resistance on reintroduction
, higher doses (>10mg) associated with temporary warfarin resistance on reintroduction Unfractionated heparin Protamine 1 mg per 100 units, risks bradycardia and hypotension Allergic reactions due to previous exposure to protamine containing insulin, vasectomy and fish allergies LMWH Protamine less effective due to shorter heparin chains Normal dosing acutely reverses 42% of factor Xa activity and 92% of anti-factor IIa actvity Warfarin Oral vitamin K reduces INR in 24 hrs Low dose IV doses effective (0.5 to 2.5mg), higher doses (>10mg) associated with temporary warfarin resistance on reintroduction")
22
Reversal of anticoagulants Warfarin INR lowering or omitting a dose INR >5 and withhold 1 to 2 doses +/- 1 to 2.5mg of oral vitamin K INR >9 3 to 5mg of oral vitamin K For serious bleeding => FFP and slow IV administration of 10mg vitamin K In preparation for surgery, most patients require 4 days to reach an INR <1.5 after discontinuation of therapy Warfarin INR lowering or omitting a dose INR >5 and withhold 1 to 2 doses +/- 1 to 2.5mg of oral vitamin K INR >9 3 to 5mg of oral vitamin K For serious bleeding => FFP and slow IV administration of 10mg vitamin K In preparation for surgery, most patients require 4 days to reach an INR <1.5 after discontinuation of therapy

23
Reversal of anticoagulants For VTE, preoperative heparin for INR <2.0 in those with an event within 1 month Postoperative heparin for those with an event in preceeding 3 months For cardiogenic thromboembolism, preoperative anticoagulation for those with an event in the preceeding month For low risk patients (remote >3 month hx of DVT, or atrial fibrillation without stroke) no heparin is indicated High risk patients (recent DVT, prosthetic mitral valves, or older mechanical valves) warfarin D/C 4 days prior with full bridging heparin anticoagulation when INR <2 For VTE, preoperative heparin for INR <2.0 in those with an event within 1 month Postoperative heparin for those with an event in preceeding 3 months For cardiogenic thromboembolism, preoperative anticoagulation for those with an event in the preceeding month For low risk patients (remote >3 month hx of DVT, or atrial fibrillation without stroke) no heparin is indicated High risk patients (recent DVT, prosthetic mitral valves, or older mechanical valves) warfarin D/C 4 days prior with full bridging heparin anticoagulation when INR <2
 no heparin is indicated High risk patients (recent DVT, prosthetic mitral valves, or older mechanical valves) warfarin D/C 4 days prior with full bridging heparin anticoagulation when INR <2 For VTE, preoperative heparin for INR <2.0 in those with an event within 1 month Postoperative heparin for those with an event in preceeding 3 months For cardiogenic thromboembolism, preoperative anticoagulation for those with an event in the preceeding month For low risk patients (remote >3 month hx of DVT, or atrial fibrillation without stroke) no heparin is indicated High risk patients (recent DVT, prosthetic mitral valves, or older mechanical valves) warfarin D/C 4 days prior with full bridging heparin anticoagulation when INR <2")
24
2004;126;204-233 Chest Hylek Jack Ansell, Jack Hirsh, Leon Poller, Henry Bussey, Alan Jacobson and Elaine Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy The Pharmacology and Management of the Vitamin K Antagonists: The

25
Reversal of anticoagulants Newer anticoagulants No specific antidote for factor Xa inhibitors Protamine ineffective against direct thrombin inhibitors Lepirudin and bivalirudin can be partially cleared by hemodialysis Newer anticoagulants No specific antidote for factor Xa inhibitors Protamine ineffective against direct thrombin inhibitors Lepirudin and bivalirudin can be partially cleared by hemodialysis

Similar presentations








 of these drugs should be the one(s) I use, and for what?>")



 V, VIII, XIII, Fibrinogen Inactive Factor Xa Common Pathway Inactive.>")








