Download presentation
1
Management of pancreatic adenocarcinoma
Moderator: Dr A. Saraya Presenter: Ujjwal

2
EPIDEMIOLOGY 13th most common cancer and 8th most common cause of cancer related deaths Pancreatic cancer is the second most common gastrointestinal malignancy in the United States For all stages combined, the one- and five-year relative survival rates are 24% and 5% American cancer society, facts and figures, 2004

3
EPIDEMIOLOGY 80% to 90% of tumors are diagnosed at an unresectable stage In India, incidence increasing over last 2 decades in both males and females Cancer mortality and morbidity in Mumbai, Indian cancer society,1997

4
India has the lowest incidence of pancreatic cancer
/100,000 males and /100,000 females Dhir V et al, Indian J gastroenterol 1999 No significant decrease in mortality over last 2 decades even in developed countries GLOBOCON 2008 Cancer Incidence and Mortality

5
RISK FACTORS ENVIRONMENTAL
Cigratte smoking (most important) (OR 1.74, 95% CI 1.61–1.87), Consumption of red processed meat (OR 1.55, 95% CI 1.16–2.07) Occupational exposure to benzidine and beta-napthylamine The risk may be particularly elevated in smokers who have homozygous deletions of the gene for glutathione S-transferase T1 (GSTT1), which is a carcinogen metabolizing enzyme.16
 (OR 1.74, 95% CI 1.61–1.87), Consumption of red processed meat (OR 1.55, 95% CI 1.16–2.07) Occupational exposure to benzidine and beta-napthylamine. The risk may be particularly elevated in smokers who have homozygous deletions of the gene for glutathione S-transferase T1 (GSTT1), which is a carcinogen metabolizing enzyme.16.")
6
BMI of more than 35 (OR 1.55, 95% CI 1.16–2.07)
consumption of more than 6 alcoholic beverages per day (OR 1.46, 95% CI 1.16– 1.83) Klein AP. Identifying people at high risk of developin pancreaticcancer. Nat Rev Cancer 2013
 Klein AP. Identifying people at high risk of developin pancreaticcancer. Nat Rev Cancer")
7
presence of non–type O blood antigens (OR 1. 42, 95% CI 1. 21–1
presence of non–type O blood antigens (OR 1.42, 95% CI 1.21–1.66), which display aberrant expression on pancreatic ductal cells, and affect signal transduction and cellular adhesion Wolpin BM. Genotype derived ABO blood groups alleles and the risk of pancreatic cancer. Cancer Res 2010
, which display aberrant expression on pancreatic ductal cells, and affect signal transduction and cellular adhesion. Wolpin BM. Genotype derived ABO blood groups alleles and the risk of pancreatic cancer. Cancer Res")
8
Chronic pancreatitis (risk: 2% per decade,independent of the type of pancreatitis)
RR: 7.2 Bracci PM et al, cancer 2009

9
family history of pancreatic cancer (OR 2.41, 95% CI 1.04– 4.74)
GENETIC FACTORS family history of pancreatic cancer (OR 2.41, 95% CI 1.04– 4.74) hereditary pancreatic cancer syndrome Hereditary pancreatitis (RR: 50-80) Peutz-jeghers syndrome (RR: 132) HNPCC (RR: unknown) FAMMM (RR: 20-30) Familial atypical mole melanoma: Two or more blood relatives with melanoma and an underlying CDKN2A/p16 mutation. Assocation with pancreatic cancer: OR 47.8, 95% CI 28.4–74.7. Prevalence: >1/1000.
 hereditary pancreatic cancer syndrome. Hereditary pancreatitis (RR: 50-80) Peutz-jeghers syndrome (RR: 132) HNPCC (RR: unknown) FAMMM (RR: 20-30) Familial atypical mole melanoma: Two or more blood relatives with melanoma and an underlying CDKN2A/p16 mutation. Assocation with pancreatic cancer: OR 47.8, 95% CI 28.4–74.7. Prevalence: >1/1000.")
10
CLINICAL PRESENTATION
The pancreas is located in the retroperitoneum, where initial growth of the cancer is silent; therefore, symptoms are usually a sign of advanced disease. Depends on the stage of disease and the location of the primary tumour

11
CLINICAL PRESENTATION
Right–upper quadrant or epigastric pain (79%) Jaundice (56%) Nausea or vomiting secondary to obstruction of the gastric outlet (51%) Diarrhea (43%) and steatorrhea due to pancreatic insufficiency (25%) New or worsening back pain (49%) could signal cancer in the pancreatic body or tail.
 Jaundice (56%) Nausea or vomiting secondary to obstruction of the gastric outlet (51%) Diarrhea (43%) and steatorrhea due to pancreatic insufficiency (25%) New or worsening back pain (49%) could signal cancer in the pancreatic body or tail.")
12
systemic manifestations may include:
New onset or worsening of previously stable diabetes, although not usually due to the cancer, should alert the physician to the possibility of pancreatic cancer systemic manifestations may include: rapid weight loss (85%) and anorexia (83%) thromboembolic disease (3%) ...Porta Mand stage. Clin Transl Oncol 2005 At diagnosis, one third of tumours of the pancreas head were in stage I and another third in stage IV. None of the tumours of the body and tail were in stage I, and over 80% were in stage IV (p < 0.001) . At presentation, the most frequent symptoms were asthenia (86%), anorexia (85%), weight-loss (85%), abdominal pain (79%), and choluria (59%). Cholestatic symptoms were more common in tumours affecting only the pancreatic head (p < 0.001) . There was a clear trend toward more localized tumours with increasing numbers of cholestatic signs (p < 0.001) . Asthenia, anorexia and weight-loss were unrelated to stage. An increased symptom-to-diagnosis interval was associated with more advanced stage (p = 0.048
 and anorexia (83%) thromboembolic disease (3%) ...Porta Mand stage. Clin Transl Oncol At diagnosis, one third of tumours of the pancreas head were in stage I and another third in stage IV. None of the tumours of the body and tail were in stage I, and over 80% were in stage IV (p < 0.001) . At presentation, the most frequent symptoms were asthenia (86%), anorexia (85%), weight-loss (85%), abdominal pain (79%), and choluria (59%). Cholestatic symptoms were more common in tumours affecting only the pancreatic head (p < 0.001) . There was a clear trend toward more localized tumours with increasing numbers of cholestatic signs (p < 0.001) . Asthenia, anorexia and weight-loss were unrelated to stage. An increased symptom-to-diagnosis interval was associated with more advanced stage (p =")
13
PANCREATIC CANCER ACCORDING TO SITE
pancreatic head, neck or uncinate process (70%) body or tail (20%) Multifocal disease (10%) Artinyan A et al. The anatomic location of pancreatic cancer is a prognostic factor for survival. HPB 2008
 body or tail (20%) Multifocal disease (10%) Artinyan A et al. The anatomic location of pancreatic cancer is a prognostic factor for survival. HPB")
14
SURGERY/EXTENT ACCORDING TO SITE
HEAD N=18666 BODY/TAIL N=5192 P-VALUE CANCER DIRECTED SURGERY 5637 29% 960 16% < 0.001 EXTENT OF DISEASE METASTATIC 6252 35% 3841 67%

15
SURVIVAL ACCORDING TO SITE

16
DIAGNOSIS AND STAGING Triphasic contrast-enhanced abdominal CT (sensitivity 89%–97%, specificity 95%) Most validated imaging study for both diagnosis and staging Useful in assessing resectibility 70-85 % of those who have resectable disease on CT undergo curative resection

17
Sensitivity poor for peritoneal metastasis and tumor < 2 cm in size
MRI is considered equivalent to CT (sensitivity 81%–99%, specificity 70%–93%), its more limited availability has restricted its use to patients with contraindications to CT (e.g., pregnancy, nephropathy) or where resectability is unclear after CT. Optimal study: NCCT plus arterial, portal venous and pancreatic protocol phase with 3 mm cuts
, its more limited availability has restricted its use to patients with contraindications to CT (e.g., pregnancy, nephropathy) or where resectability is unclear after CT. Optimal study: NCCT plus arterial, portal venous and pancreatic protocol phase with 3 mm cuts.")
18
Optimal study: Non-contrast plus arterial, portal venous and pancreatic protocol phase with 3 mm cuts

19
ROLE OF EUS Diagnosis: For tumors < 2 cm in size which are not well visualised on CT Inflammotory head mass in the setting of chronic pancreatitis To discriminate between benign and malignant strictures

20
ROLE OF EUS STAGING: Complimentary to CT and MRI
Mainly in patients whose scans show doubtful vascular or lymph node involvement

21
ROLE OF PET-CT Has a role in staging of disease
Adjunct to multiphasic CT/MRI Has increased sensitivity for detection of distant metastasis Can prevent unnecessary pancreatic resection in upto 25 % of patients by detecting unsuspected metastasis Saif MW et al, J. gastrointestin liver disease, 2008

22
ROLE OF LAPROSCOPY Role in staging:
High sensitivity for peritoneal and liver capsular metastasis Not a substitute for poor quality imaging

23
ROLE OF LAPROSCOPY Considered when high risk of metastatic disease:
Tumor size > 2cm Border line resectable disease Tumor of body/tail Markedly elevated CA 19-9

24
ROLE OF BIOPSY No role in resectable disease
Required in unresectable disease and metastatic disease to confirm diagnosis before starting chemotherapy EUS FNA is preferable to CT guided FNA Less bleeding and infection and metastatic seeding

25
BIOMARKERS Various biomarkers:
CA 19-9 (best validated and most useful) CA 125 CEA Pancreatic oncofetal antigen
 CA 125. CEA. Pancreatic oncofetal antigen.")
26
CA 19-9: Sialylated lewis A blood group antigen Good diagnostic marker (sensitvity: 80%, specificity: 82-90%) Correlates with staging and resectibility

27
Prognostic marker: Low post-operative levels and serial decrease in levels after surgery correlate with survival post curative resection Berger AC et al J. Clin oncology 2008 Pre-treatment levels are an independent prognostic factor for survival in advanced pancreatic cancers Hess V et al, lancet oncology 2008

28
Predictor of response:
Change in CA 19-9 levels after chemotherapy in patients with advanced disease predicts response to treatment

29
FALSE – ve: lewis antigen negative patients
Biliary obstruction Cholangitis Biliary malignanciaes Pre-operative levels should be measured after biliary drainage and normalisation of blirubin levels

30
SUMMARY

32
STAGING stage Tumor grade Node status Distant metastasis 5yr survival,
% Median Survival,mo Characteristics IA T1 No Mo 14 24 Tumor <2cm in pancreas only IB T2 12 21 Tumor >2cm in pancreas only IIA T3 7 15 Tumor extends beyond the pancreas, but with no involvement of the celiac or SMA IIB T1-3 N1 5 13 Regional lymph node metastasis III T4 N0-1 3 11 Tumor involves the celiac or SMA IV T1-4 M1 1

33
CLASSIFICATION PANCREATIC ADENOCARCINOMA BOREDERLINE RESECTABLE
PPANCREATIC BOREDERLINE RESECTABLE RESECTABLE ADVANCED METASTASIS ENCASEMENT OF ARTERIES EXTENSIVE INVOLVEMENT OF VEINS NO METASTASIS NO VASCULAR INVOLVEMANT PARTIAL ABUTMENT OF PORTAL OR SMV

34
Stage of disease SMA Celiac axis Common Hepatic Artery SMV-PV Resectable(all four required) No extension; normal fat plane between the tumor and the artery Patent (may include tumor abutment or encasement) Boderline resectable (one required) Abutment Abutment or short segment encasement if reconstruction possible Short segment occlusion if reconstruction possible Unresectable (one required) Encasement Extensive encasement with no technical option for reconstruction Occluded with no technical option for reconstruction
 Boderline resectable (one required) Abutment. Abutment or short segment encasement if reconstruction possible. Short segment occlusion if reconstruction possible. Unresectable (one required) Encasement. Extensive encasement with no technical option for reconstruction. Occluded with no technical option for reconstruction.")
35
RESECTABLE DISEASE Only 15% -20 % of newly diagnosed cases
SURGERY is the only curative treatment Procedure depends on the location of the tumour: Pancreaticoduodenectomy (Whipple procedure): lesions of the head, neck and uncinate process Distal pancreatectomy: lesions of the body or tail Total pancreatectomy: multifocal disease
: lesions of the head, neck and uncinate process. Distal pancreatectomy: lesions of the body or tail. Total pancreatectomy: multifocal disease.")
36
Overall 5-year survival after pancreatic resection is 14
Overall 5-year survival after pancreatic resection is 14.6%, but higher in well-differentiated disease (30%–40%) and disease that has not metastasized to the lymph nodes (25%–30%) Cleary SP, et al J Am Coll Surg 2004 Negative margin status, tumor size and lymph node status are the strongest predictors of survival
 and disease that has not metastasized to the lymph nodes (25%–30%) Cleary SP, et al J Am Coll Surg Negative margin status, tumor size and lymph node status are the strongest predictors of survival.")
37
ADJUVANT CHEMOTHERAPY
Recommended for all patients who undergo curative resection Either gemcitabine or 5 - fluorouracil (5-FU) prolongs median survival by 3 months (95% CI 0.3–5.7) Boeck S et al Oncology 2007 metaanalysis
 prolongs median survival by 3 months (95% CI 0.3–5.7) Boeck S et al Oncology 2007 metaanalysis.")
38
We performed a retrospective review 472 consecutive patients who underwent complete
resection with negative margins (R0) for invasive carcinoma (T1-3N0-1M0) of the pancreas between 1975 and 2005 at the Mayo Clinic in Rochester, MN.
 for invasive carcinoma (T1-3N0-1M0) of the pancreas. between 1975 and 2005 at the Mayo Clinic in Rochester, MN.")
39
For the 466 surviving patients, median follow-up was 32
For the 466 surviving patients, median follow-up was 32.4 months; median OS was 21.6 months. Median OS after adjuvant CT-RT was 25.2 versus 19.2 months after no adjuvant therapy (P .001). Two-year OS was 50% versus 39%, and 5-year OS was 28% versus 17%.
. Two-year OS was 50% versus 39%, and 5-year OS was 28% versus 17%.")
40
Adverse prognostic factors identified by univariate and multivariate analysis included positive lymph nodes (risk ratio [RR] 1.3; P .001), high histologic grade (RR 1.2; P .001), and no adjuvant therapy (RR 1.3; P .001).
![Adverse prognostic factors identified by univariate and multivariate analysis included positive lymph nodes (risk ratio [RR] 1.3; P .001), high histologic grade (RR 1.2; P .001), and no adjuvant therapy (RR 1.3; P .001).](http://slideplayer.com/slide/2478860/9/images/40/Adverse+prognostic+factors+identified+by+univariate+and+multivariate+analysis+included+positive+lymph+nodes+%28risk+ratio+%5BRR%5D+1.3%3B+P+.001%29%2C+high+histologic+grade+%28RR+1.2%3B+P+.001%29%2C+and+no+adjuvant+therapy+%28RR+1.3%3B+P+.001%29..jpg "Adverse prognostic factors identified by univariate and multivariate analysis included positive lymph nodes (risk ratio [RR] 1.3; P .001), high histologic grade (RR 1.2; P .001), and no adjuvant therapy (RR 1.3; P .001).")
41
Gemcitabine has been recommended as the first-line adjuvant agent owing to its lower toxicity profile

42
ROLE OF ADJUAVENT RADIATION
The benefit of adjuvant radiation therapy is unclear based on the results of the ESPAC-1 trial.28 Median survival with chemoradiation (13.9 mo, 95% CI 12.2–17.3) was similar to that seen with observation alone (16.9 mo, 95% CI 12.3–24.8), but was longer when chemoradiation was followed by chemotherapy (19.9 mo, 95% CI 14.2–22.5) and longest with adjuvant chemotherapy alone (21.6 mo, 95% CI 13.5– 27.3).
 was similar to that. seen with observation alone (16.9 mo, 95% CI. 12.3–24.8), but was longer when chemoradiation. was followed by chemotherapy (19.9 mo, 95% CI 14.2–22.5) and longest with adjuvant. chemotherapy alone (21.6 mo, 95% CI 13.5– 27.3).")
45
ROLE OF ADJUAVENT RADIATION
No clear benefit of radiation therapy in addition to adjuvant chemotherapy

46
ROLE OF NEOADJUAVENT THERAPY
Benefit of neoadjuvant therapy at the cost of delaying surgery is controversial No phase III trials comparing outcomes between neoadjuvant and adjuvant therapy most centres refrain from using neoadjuvant therapy outside of research protocols

47
A meta -analysis mainly consisting of heterogenous phase I and II studies found a median overall survival of 23.3 (range 12–54) months, with perioperative mortality of 5.3% (95% CI 4.1%– 6.8%).
 months, with perioperative mortality of 5.3% (95% CI 4.1%– 6.8%).")
48
A total of 111 studies (n = 4,394) including 56 phase I-II trials were analyzed. A median of 31 (interquartile range [IQR] 19-46) patients per study were included.
 patients per study were included..")
49
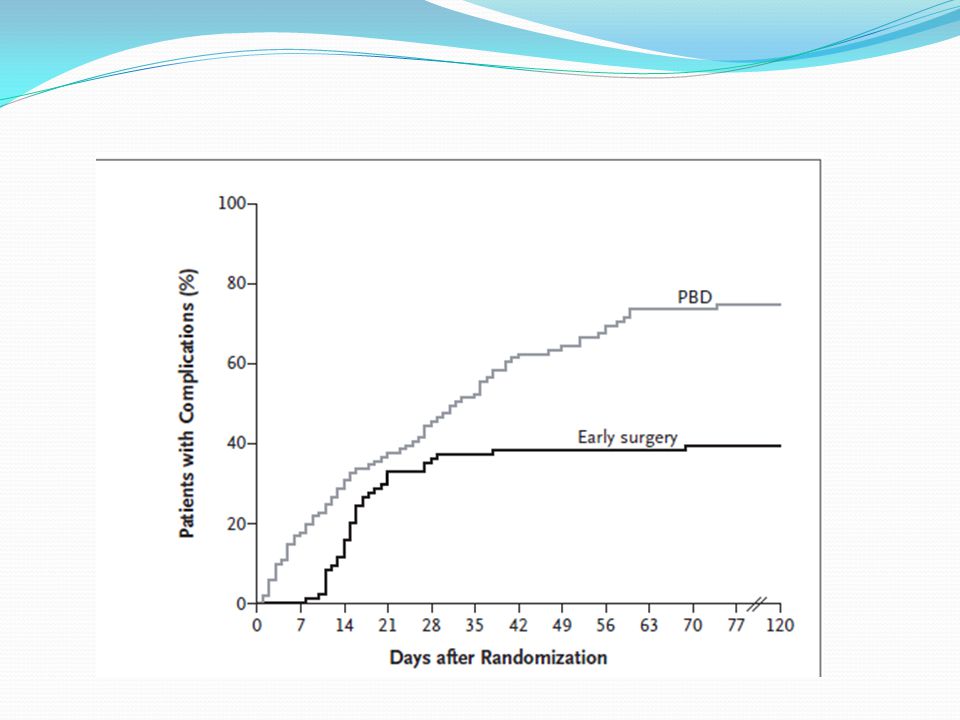
ROLE OF PRE-OPERATIVE DRAINAGE
Goal To alleviate symptoms of pruritis To provide drainage in patients with cholangitis Decrease surgical morbidity by improving liver function

50
Studies have failed to show decreased mortality in patients who underwent pre-operative drainage

51
RCT in 2010

53
Recommended: Cholangitis Significant pruritis and > 1 week delay of surgery If patient has to receive neoadjuvant therapy Plastic stents are preferred over metal stents

54
BORDERLINE RESECTABLE DISEASE
Surgery is attempted only if complete resection is possible Role of neoadjuvant therapy is debatable No phase 3 RCTs A 6-year prospective study involving 110 patients with resection of the hepatic portal vein, SMV or both for suspected tumour infiltration showed median overall survival of 14.5 (range 7.3–24) months, with perioperative mortality of 3.7%. Müller SA, Hartel M, Mehrab A, et al. Vascular resection in pancreatic cancer surgery: survival determinants. J Gastrointest Surg 2009;13: These results suggest that major venous resection and reconstruction is safe in experienced hands and results in oncologic results equivalent to those of complete resection.
 months, with perioperative mortality of 3.7%. Müller SA, Hartel M, Mehrab A, et al. Vascular resection in pancreatic cancer surgery: survival determinants. J Gastrointest Surg 2009;13: These results suggest that major venous resection and reconstruction is safe in experienced hands and results in oncologic results equivalent to those of complete resection.")
55
A role and optimal regimen for neoadjuvant therapy in borderline resectable disease is unclear, based on inconclusive findings regarding median survival in a retrospective study of neoadjuvant treatment versus immediate surgery (35 mo v. 27 mo; p = 0.7). Barugola G et al. Outcomes after resection of borderline resectable pancreatic cancer after neoadjuvant therapy. Am J Surg 2012

56
ADVANCED DISEASE Median overall survival of 2–3 months without treatment Chemotherapy is advised as it improves survival Distant organ involvement, typically that of the liver, peritoneum or lung, occurs in 50% of cases.

57
51 trials involving 9,970 patients met the inclusion criteria, and 33 of these trials involving 6,026 patients were included in the meta-analyses

58
N=432 mortality reduction = 36 %
51 trials involving 9,970 patients met the inclusion criteria, and 33 of these trials involving 6,026 patients were included in the meta-analyses. N=432 mortality reduction = 36 %

59
Journal of clinical oncology, 1997
Gemcitabine better than 5 FU Journal of clinical oncology, 1997

61
ROLE OF COMBINATION CHEMOTHERAPY
No overall improved survival as compared to monotherapy Survival benefit in a subset of patient who have good performance status Individual clinical trials of combination gemcitabine with various cytotoxic agents53–56 have failed to show a survival benefit over gem citabine alone (Appendix 1), but significantly improved overall survival was seen when these studies were pooled (HR 0.91, 95% CI 0.85–0.97).37 Furthermore, patients with a good performance status (Karnofsky performance score > 90%) survived longer with combination gem citabine (HR 0.76, 95% CI 0.67–0.87), whereas patients with a poor performance status did not (HR 1.08, 95% CI 0.90– 1.29).
, but significantly improved overall survival was seen when these studies were pooled (HR 0.91, 95% CI 0.85–0.97).37 Furthermore, patients with a good performance status (Karnofsky performance score > 90%) survived longer with combination gem citabine (HR 0.76, 95% CI 0.67–0.87), whereas patients with a poor performance status did not (HR 1.08, 95% CI 0.90– 1.29).")
63
improve Meta analysis for combination chemotherapy in advanced pancreatic cancer – overall survival with regard to combination partner (platinum analog, fluoropyrimidine or other) for gemcitabine.
 for gemcitabine.")
64
Meta-analysis for combination chemotherapy in advanced pancreatic cancer-overall survival with regard to performance status

65
Reserved for patients with good performance status
Individual clinical trials of combination gemcitabine with various cytotoxic agents have failed to show a survival benefit over gemcitabine alone but significantly improved overall survival was seen when these studies were pooled (HR 0.91, 95% CI 0.85–0.97) Reserved for patients with good performance status Combination therapy also showed higher grade 3/4 toxicity: neutropenia (risk difference [RD] 5%, 95% CI 1%–10%), thrombocytopenia (RD 5%, 95% CI 2%–8%) and nausea or vomiting (RD 3%, 95% CI 0%–5%).57 Combination chemotherapy is reserved for patients with a good performance status.
 Reserved for patients with good performance status. Combination therapy also showed higher grade 3/4 toxicity: neutropenia (risk difference [RD] 5%, 95% CI 1%–10%), thrombocytopenia. (RD 5%, 95% CI 2%–8%) and nausea or vomiting (RD 3%, 95% CI 0%–5%).57 Combination chemotherapy is reserved for patients with a good. performance status.")
66
GEMCITABINE + ERLOTINIB
Targeted therapy in pancreatic cancer has centred on the epidermal growth factor pathway Erlotinib: tyrosine kinase inhibitor of EGFR

67
Kaplan-Meier curves for (A) overall survival;
(B) progression-free survival; and (C) overall survival in the 100-mg cohort.
 progression-free survival; and. (C) overall survival in the 100-mg cohort.")
68
This phase III study of the epidermal growth factor receptor inhibitor erlotinib with gemcitabine versus gemcitabine alone showed marginally increased overall survival (6.24 v mo,vs p = 0.04)58 and 1-year survival (23% [95% CI 18%–28%] v. 17% [95% CI 12%–21%], p = 0.02). combination gem - citabine/ erlotinib is considered for patients with good performance status in the metastatic setting.
![This phase III study of the epidermal growth factor receptor inhibitor erlotinib with gemcitabine versus gemcitabine alone showed marginally increased overall survival (6.24 v mo,vs p = 0.04)58 and 1-year survival (23% [95% CI 18%–28%] v. 17% [95% CI 12%–21%], p = 0.02).](http://slideplayer.com/slide/2478860/9/images/68/This+phase+III+study+of+the+epidermal+growth+factor+receptor+inhibitor+erlotinib+with+gemcitabine+versus+gemcitabine+alone+showed+marginally+increased+overall+survival+%286.24+v+mo%2Cvs+p+%3D+0.04%2958+and+1-year+survival+%2823%25+%5B95%25+CI+18%25%E2%80%9328%25%5D+v.+17%25+%5B95%25+CI+12%25%E2%80%9321%25%5D%2C+p+%3D+0.02%29..jpg "combination gem - citabine/ erlotinib is considered for patients with good performance status in the metastatic setting.")
69
GEMCITABINE + ERLOTINIB
Recommended as an option for patients with locally advanced and metastatic disease Benefit more in patients who develop skin rash

70
FOLFIRINOX FOLFIRINOX (5-FU, leuco - vorin, irinotecan and oxaliplatin) Increase in median overall survival over gemcitabine alone in metastatic pancreatic cancer (11.1 mo v. 6.8 mo; HR 0.57, 95% CI 0.45– 0.73, p < 0.001).
.")
71
FOLFIRINOX

72
Folfirinox: 11.1 months gemcitabine: 6.6 months

73
Folfirinox: 6.4 months gemcitabine: 3.3 months

74
FOLFIRINOX

76
THANK YOU