Download presentation
Presentation is loading. Please wait.

1
Head and Neck Cancers Management
Dr. S. C. Joshi Senior Consultant Oncologist and Radiotherapist D/L : Mobile Phone : ,

2
Head and Neck Cancers Management
Dr. S. C. Joshi Senior Consultant Oncologist and Radiotherapist D/L : Mobile Phone : ,

3
Epidemiology Head and neck cancers constitute 5% of all cancers worldwide 10th most common cancer in the world World – annual incidence: 643,000 new cases Mortality of about 350,000 cases MC in India– 15.4 to per 100,000 males 2 to 51.2 per 100,000 females By: Dr.S.C.Joshi

4
Risk Factors Smoking Tobacco (Masala, kaini and others)
Viruses - Epstein-Barr Virus, HPV (16, 18) Environmental/occupational Exposures of Asbestos, Chromium, Nickel, Arsenic, Formaldehyde Salted Fish Ionizing Radiation Genetic Immunodeficiency Poor oral hygiene Alcohol Betet nut By: Dr.S.C.Joshi
 Environmental/occupational. Exposures of Asbestos, Chromium, Nickel, Arsenic, Formaldehyde. Salted Fish. Ionizing Radiation. Genetic. Immunodeficiency. Poor oral hygiene. Alcohol. Betet nut. By: Dr.S.C.Joshi.")
5
Disease Sites of the Head and Neck
Head and neck cancer may occur in diverse structures and sites: Lip Oral cavity Tongue Pharynx Larynx Nasal cavity Sinuses By: Dr.S.C.Joshi

6
Mostly Arise in The Nasopharyngeal Axis
Nasal Cavity Nasopharynx Oral Cavity Oropharynx Larynx Hypopharynx By: Dr.S.C.Joshi

7
Head and Neck Cancer Often Spreads to Regional Lymph Nodes
Lymph node involvement in up to 30%-50%. By: Dr.S.C.Joshi

8
> 75 % present with advanced disease in developing countries due to the lack of awareness, early intervention and treatment facilities By: Dr.S.C.Joshi

9
Diagnosis 70%- 80% are diagnosed having locally advanced disease (Stage III and IV) In the more advanced tumors (stage III and IV) Local recurrence –up to 50% Distant metastatic spread (approximately 10%-30%) By: Dr.S.C.Joshi
 By: Dr.S.C.Joshi.")
10
Diagnosis History General physical examination & Local ex Oral cavity
Oropharynx (palpation is very important) Nasopharynx (mirror examination) Laryngopharynx (indirect laryngoscopy) Examination of the neck for lymph nodes Direct laryngoscopy Biopsy of any suspected areas By: Dr.S.C.Joshi
 Nasopharynx (mirror examination) Laryngopharynx (indirect laryngoscopy) Examination of the neck for lymph nodes. Direct laryngoscopy. Biopsy of any suspected areas. By: Dr.S.C.Joshi.")
11
Laboratory Studies Routine blood counts. Blood chemistry profile
Urinalysis Chest radiographs, Plain radiographs of mandible (Panorex view) CT Scan / MRI / PET CT By: Dr.S.C.Joshi
 CT Scan / MRI / PET CT. By: Dr.S.C.Joshi.")
12
Surgery Radiotherapy Chemotherapy
No substantial change in survival in 25 yrs.

13
Management Guidelines for H & N Cancers
Aims Highest Loco- regional control Anatomical and functional organ preservation Treatment Principles Early Stage Single modality treatment using Surgery or Radiotherapy Late Stage Surgery + Radiotherapy Concurrent Chemoradiotherapy By: Dr.S.C.Joshi

14
Management Guidelines for H & N Cancers
When different modalities available, one with maximum chance of cure should be used When different modalities have same results, one offering better quality of life, with organ, function preservation and good cosmetic results should be used By: Dr.S.C.Joshi

15
Surgery v/s Radiotherapy
In treatment of head and neck cancers surgery and radiotherapy produce equivalent results in early stages of carcinoma In advanced stages of head and neck cancers surgery combined with pre or postoperative radiotherapy By: Dr.S.C.Joshi

16
Improving Efficacy of Treatment
Chemotherapy Radiotherapy Dose escalation schedules Altered Fractionation Schemes Biological Therapy And Molecular Targeting Continuous review during treatment By: Dr.S.C.Joshi

17
Chemotherapy Absolute benefit of Chemotherapy > 30% at 5 years
Higher For Platinum Based Regimens. Higher doses up to 70 Gy are related with better Loco regional control, however with enhanced acute and long term complications By: Dr.S.C.Joshi

18
Radiation Therapy Ionizing Radiation
High energy electromagnetic waves in the form of X-rays or gamma-rays External beam radiation Utilizes LA to generate X-rays to kill cancer cells Brachytherapy utilizes radioactive substances implanted into tumors. By: Dr.S.C.Joshi

19
How Radiation Works X-ray photons interact with matter, knocking electrons from the orbital's of atoms These high energy electrons can either directly damage DNA chemical bonds, or interact with water molecules forming free radicals that then cause DNA damage Damage to DNA may result in single or double strand breaks which can cause cell death DNA repair enzymes are more readily activated in healthy cells than in cancer cells By: Dr.S.C.Joshi

20
The Changing Paradigm Conformal radiation IMRT/IGRT/Rapid arc Clinical motivation for high-precision techniques More conformality = Better sparing By: Dr.S.C.Joshi

21
Standard Radiation Techniques (old)
Conventional external beam radiation usually consists of two opposed lateral fields and a matched anterior field that encompass the cancer and lymph nodes in the neck. Treatment is delivered daily for about 7 weeks. When this technique developed, physicians used regular X-rays or fluoroscopy to setup these fields. By: Dr.S.C.Joshi

22
CT Based Radiation Planning
With the advent of CT guided planning, a new era in RTP has emerged. We are now better able to customize our treatment plans to fit the individual patient anatomy By: Dr.S.C.Joshi

23
IMRT – Intensity Modulated Radiation Therapy
In this intensity of the radiation beam in a given treatment field is varied via multiple multi leaf blocking arrangements called segments Intensity modulation combined with multiple fields (radiation beam angles) or arcs allows for conformal radiotherapy (ie high radiation iso dose lines conform to the target volume and spare normal tissues). By: Dr.S.C.Joshi
 or arcs allows for conformal radiotherapy (ie high radiation iso dose lines conform to the target volume and spare normal tissues). By: Dr.S.C.Joshi.")
24
Intensity Modulated Radiation Therapy (IMRT)
IMRT is an advanced form of 3D-CRT technique in which a computer aided optimisation process is used to determine customised non-uniform intensity distribution through inverse planning to attain certain specified dosimetric and clinical objectives By: Dr.S.C.Joshi

25
Intensity Modulated Radiation Therapy (IMRT)
Multiple beam angles or arcs Multi-leaf collimator Accurate patient positioning and immobilization Physics quality assurance measures Well trained radiation therapy staff By: Dr.S.C.Joshi

26
Multi-leaf Collimator
The multi-leaf collimator is inside the linear accelerator. It is comprised of multiple 1 cm thick metal radiation blocks each driven by an independent motor and controlled by a central computer. The multi-leaf collimator allows for multiple blocking patterns in each radiation field which in turn allows for intensity modulation of the radiation dose. By: Dr.S.C.Joshi

27
Immobilization By: Dr.S.C.Joshi

28
Head and Neck Immobilization Devices
3 Clamp 4 Clamp 5 Clamp Random Errors with different Fixation devices By: Dr.S.C.Joshi Radiotherapy Oncology,2001

29
Time Interval Importance of the time interval between surgery and postoperative RT in the combined management of head and neck cancers PORT within 6-7 weeks / later LRC : 70% (PORT within 7 weeks) >27% (PORT more than 7 weeks) Therefore patient must be seen by oncologist immediately after surgery and HPE report. By: Dr.S.C.Joshi Bhadrasain V,IJROBP,1979
 >27% (PORT more than 7 weeks) Therefore patient must be seen by oncologist immediately after surgery and HPE report. By: Dr.S.C.Joshi. Bhadrasain V,IJROBP,1979.")
30
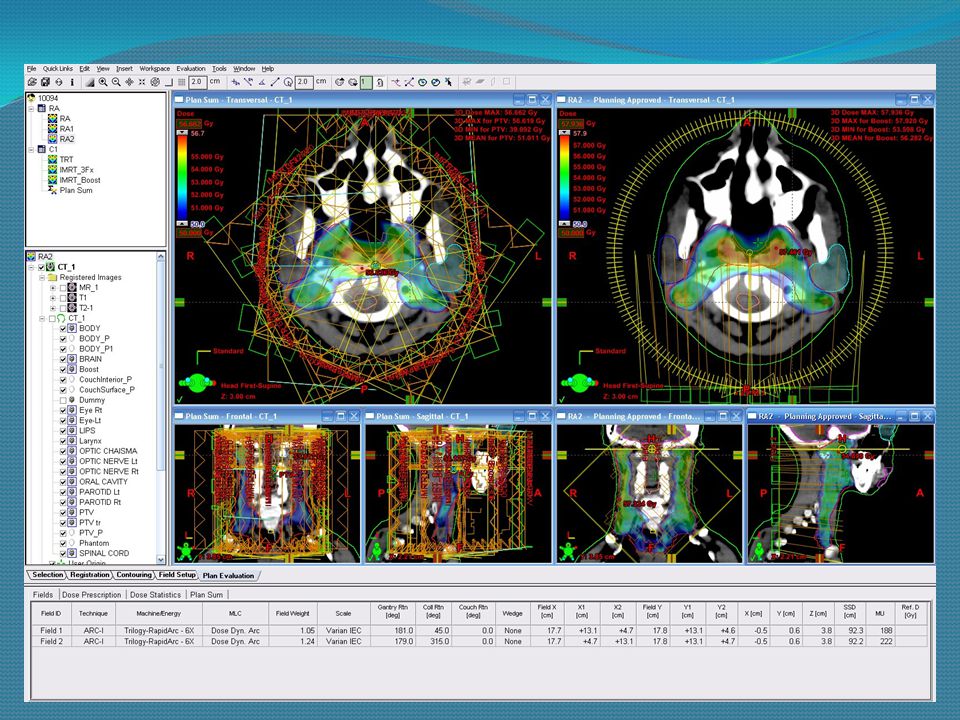
Isodose Distribution of an IMRT Plan
By: Dr.S.C.Joshi

31
IMRT - Hypopharynx By: Dr.S.C.Joshi

32
IGRT – Image Guided Radiation Therapy
Daily X-rays or CT scansAre done and overlaidwith the planning CT Millimeter adjustments are made with automatic couch position shifts Treatment becomes more accurate and consequently smaller target volumes will result in less side effects By: Dr.S.C.Joshi

33
IGRT – MV X-rays By: Dr.S.C.Joshi

34
IGRT – kV X-rays By: Dr.S.C.Joshi

35
IGRT – Cone Beam CT (CBCT)
By: Dr.S.C.Joshi

36
IGRT - CBCT By: Dr.S.C.Joshi

37
Rapid arc cases By: Dr.S.C.Joshi

39
Rapid arc cases By: Dr.S.C.Joshi

40
Rapid arc cases

41
In Developing World Infectious diseases are the main killers
Patients present in an advanced stage Fund allocation to health is less than that of developed countries No or poor social health security system Geographic clustering of facilities to urban areas Linear accelerators are expensive, with high operational costs. High precision facilities available in only selected centers. By: Dr.S.C.Joshi

42
How to Optimize Treatment for Developing Countries?

43
Optimization of Treatment
Prompt treatment in a good referral centre Optimal Infrastructure support required for implementation of CTRT/AFRT schedules Avoidance of Treatment Breaks Integration of Chemotherapy Integration of high-precision technique Good Nutritional Support. Affordable cost By: Dr.S.C.Joshi

44
Our Oncology Facilities
Linear accelerator from Varian trilogy with rapid arc Brachytherapy Chemotherapy Daycare facilities for out patient’s and isolation wards Complete nuclear medicine with Radionuclide Therapy Palliative care Cancer screening Cancer awareness program By: Dr.S.C.Joshi

45
Radiotherapy Team Consultant Oncologist Medical Physicist
Radiation Therapist Radiation Therapist Aide By: Dr.S.C.Joshi

46
By: Dr.S.C.Joshi

47
By: Dr.S.C.Joshi

48
Linac Room By: Dr.S.C.Joshi

49
By: Dr.S.C.Joshi

50
By: Dr.S.C.Joshi

51
Summary Head and neck cancer is a serious illness that affects thousands of Indians each year Smoking cessation and tobacco chewing is critical in the prevention of the disease Multimodality treatment interventions have a proven track record against the disease, but come with significant morbidity Targeted chemotherapy regimens are being developed to reduce side effects IMRT/IGRT and rapid arc have also significantly reduced the incidence of side effects from treatment. By: Dr.S.C.Joshi

52
Thank You For Your Kind Attention
Dr. Sanjeev Chandra Joshi

Similar presentations












. What is cancer? Failure of the mechanisms that control growth and proliferation of the cells Uncontrolled (often rapid) growth.>")






: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")