Download presentation
Presentation is loading. Please wait.

2
Hippocrates’ works (370 BC) The blood of females is subject to intermittent ‘agitations’ and as a result the ‘agitated blood’ makes its way from the head to the uterus whence it is expelled.3
 The blood of females is subject to intermittent ‘agitations’ and as a result the ‘agitated blood’ makes its way from the head to the uterus whence it is expelled.3")
3
four landmark stages parallel our understanding of the premenstrual disorders. From the ‘agitations’ of Hippocrates (370 BC) to premenstrual tension (PMT);1 recognition and description of symptoms From PMT to PMS;2 in this period, the link between the ovarian hormone cycles and symptoms was recognized. recognition and description of symptoms attempt to define and quantify premenstrual disorders and the theory of progesterone deficiency was explored and refuted. From PMDD to the present day; in this period there has been the realization that women are sensitive to normal levels of ovulatory progesterone, that this possibly has a neuroendocrine explanation, and that therapy can be achieved by altering neuroendocrine status with psychotropic drugs (notably selective serotonin reuptake inhibitors [SSRIs]) or by elimination of ovulation.
 to premenstrual tension (PMT);1 recognition and description of symptoms From PMT to PMS;2 in this period, the link between the ovarian hormone cycles and symptoms was recognized. recognition and description of symptoms attempt to define and quantify premenstrual disorders and the theory of progesterone deficiency was explored and refuted. From PMDD to the present day; in this period there has been the realization that women are sensitive to normal levels of ovulatory progesterone, that this possibly has a neuroendocrine explanation, and that therapy can be achieved by altering neuroendocrine status with psychotropic drugs (notably selective serotonin reuptake inhibitors [SSRIs]) or by elimination of ovulation..")
4
The diagnosis of PMS/PMDD – the current debate

5
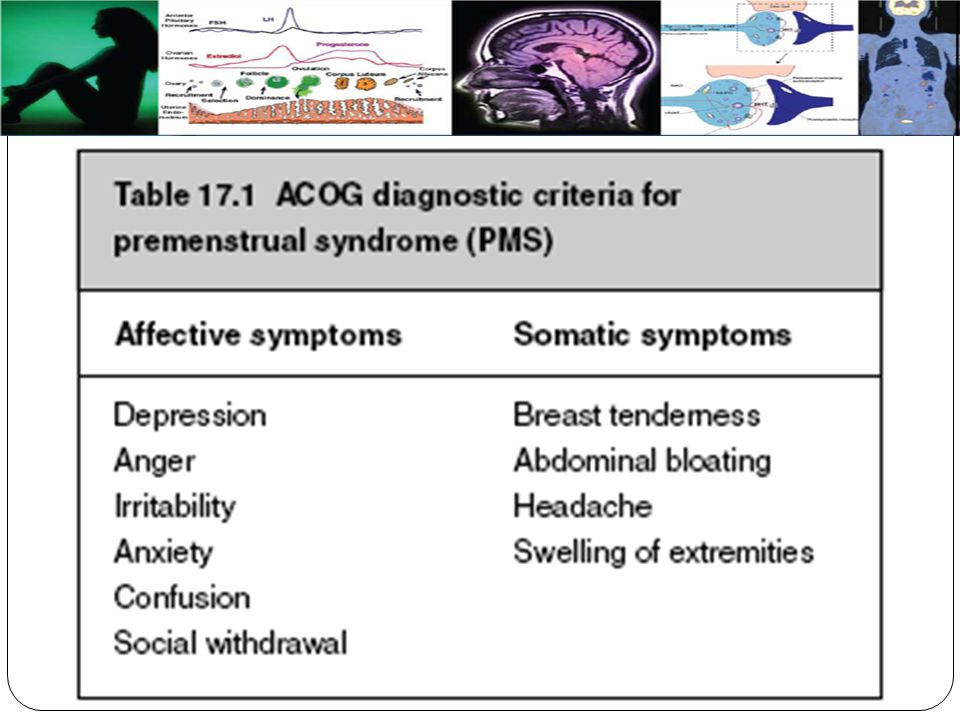
Current diagnostic criteria for PMS/PMDD ICD-10 ACOG DSM-IV

6
ACOG Occur 5 days before menses Remit within 4 days of onset of before menses No recurrence at least until day 13 of cycle

7
PMS can be diagnosed after the patient prospectively documents at least one of the affective or somatic symptoms during the 5 days prior to menses for three menstrual cycles. Symptoms should be of such severity as to impact social or economic performance. There should be no concomitant pharmacological therapy, hormone ingestion, or drug or alcohol abuse. Other psychiatric and medical disorders must have been excluded as a potential cause of the symptoms

9
DSM-IV Occur during the last week Remit within few days after No recurrence at least until onset of follicular phase

10
At least five symptoms, with at least one of: depression, anxiety, or tension, anger or irritability, and monthly swings Other qualifying symptoms are: decreased interest, difficulty concentrating, lack of energy, changed sleep, overwhelmed, out of control, change in appetite

12
Other physical symptoms such as breast tenderness, bloating headaches, pain Markedly interferes with work, social activities, relationships Most menstrual cycles during past year At least two consecutive cycles Not merely an exacerbation of another disorder Not associated with pharmacological, hormone, alcohol or drug use or abuse

13
UNSOLVED ISSUES WITH CURRENT DIAGNOSTIC CRITERIA lack of universal agreement on the nature of the PMS as well as lack of universal acceptance of the criteria per se. definition of PMDD as a diagnostic entity, independent of PMS.

14
Any mood, behavioral or physical symptom(s), or cluster(s) of symptoms that occur recurrently and cyclically during the luteal phase of the menstrual cycle. ● The symptom(s) remit(s) shortly following the beginning of menses and consistently do not exist for at least 1 week of the follicular phase of most menstrual cycles. ● The symptom(s) cause emotional or physical distress and/or suffering and/or impairment in daily functioning, and/or impairment in relationships. ● The recurrence, cyclicity, and timing of the cycle, and severity of the symptoms as well as existence of a menstrually related symptom-free period are documented by daily monitoring and/or reports.
 remit(s) shortly following the beginning of menses and consistently do not exist for at least 1 week of the follicular phase of most menstrual cycles. ● The symptom(s) cause emotional or physical distress and/or suffering and/or impairment in daily functioning, and/or impairment in relationships. ● The recurrence, cyclicity, and timing of the cycle, and severity of the symptoms as well as existence of a menstrually related symptom-free period are documented by daily monitoring and/or reports..")
17
Proposed or researched PMS treatments Non-pharmacological treatments: ● Counseling ● Relaxation therapy ● Psychotherapy ● Cognitive behavioral therapy (CBT) ● Stress management ● Homeopathy ● Intravaginal electrical stimulation ● Rest ● Isolation ● Yoga ● Aromatherapy ● Exercise ● Music therapy ● Hypnosis ● Dietary manipulation ● Salt restriction ● Self-help groups ● Agnus castus ● Irradiation of ovaries
 ● Stress management ● Homeopathy ● Intravaginal electrical stimulation ● Rest ● Isolation ● Yoga ● Aromatherapy ● Exercise ● Music therapy ● Hypnosis ● Dietary manipulation ● Salt restriction ● Self-help groups ● Agnus castus ● Irradiation of ovaries")
18
Non-hormonal pharmacological treatments: ● Tranquilizers ● Antidepressants ● Lithium ● SSRIs initial studies ● Vitamin B6 ● Beta-blockers ● Evening primrose oil ● Diuretics, spironolactone ● Magnesium, zinc, and calcium

19
Hormonal treatments: ● Progesterone (pessaries, injections, vaginal gel) ● Progestogens (norethisterone, dydrogesterone, medroxyprogesterone acetate, Depo-Provera) ● COC pill: cyclical/continuous ● Testosterone ● Bromocriptine ● Mifepristone, RU-486 ● Cyproterone acetate ● Tibolone ● Danazol, gestrinone ● Estradiol (oral, patch, implant) ● GnRH agonist analogs ● Non-steroidal anti-inflammatory drugs
 ● Progestogens (norethisterone, dydrogesterone, medroxyprogesterone acetate, Depo-Provera) ● COC pill: cyclical/continuous ● Testosterone ● Bromocriptine ● Mifepristone, RU-486 ● Cyproterone acetate ● Tibolone ● Danazol, gestrinone ● Estradiol (oral, patch, implant) ● GnRH agonist analogs ● Non-steroidal anti-inflammatory drugs")
20
Surgical treatments: ● Hysterectomy ● Hysterectomy and bilateral oophorectomy ● Endometrial ablation techniques

22
SHOULD PMS BE REGARDED AN ENDOCRINE CONDITION OR AS A BRAIN DISORDER?

23
women with premenstrual complaints differ from controls not with respect to ovarian function, but with respect to how responsive the target organs are to the influence of gonadal steroids. One important target organ for sex steroids is the central nervous system. Receptors in many brain regions including the amygdala and the hypothalamus.

24
IS PMS DUE TO SEROTONERGIC DYSFUNCTION?

25
many studies however do lend support to the notion that women with PMS/PMDD differ from controls with respect to various indices of serotonergic activity, indicating that serotonin in fact may play a significant part in the pathophysiology of this condition

26
recent pilot studies suggesting that symptomatic women differ from non-symptomatic controls with respect to uptake of a serotonin precursor and density of serotonergic 5HT1A receptors, respectively. Eriksson O, Wall A, Marteinsdottir I et al. Psychiatry Res 2006; 146:107–16. Jovanovic H, Cerin Å, Karlsson P et al. Psychiatry Res 2006; 148:185–93.

Similar presentations








)>")








 To make an accurate diagnosis of premenstrual.>")
 Jessica Sun Stress Management.>")

 is defined as “the cyclic recurrence in the luteal phase.>")


 Biological/Psychosocial???>")
>")
