Download presentation
Presentation is loading. Please wait.

1
“Walk A Mile In My Shoes”
An interactive workshop on learning disabilities Melissa Rowbotham, M.Ed Copyright © 2010 by Integra Foundation MP to start Our goal for the training: To get some receptivity to the idea that behavior may not just reflect disobedience - to convey respect and openness to any of their concerns about security (we get that these kids can be hard – but we don’t know what that’s like): start a relationship with them/ begin to engage Take home message for the day: Can’t Do vs Won’t Do (also support vs. punishment) Figure out what might be going on in behavior It is hard to do things that are hard – when faced with that – behaviors & emotions Change to include our audience
: start a relationship with them/ begin to engage. Take home message for the day: Can’t Do vs Won’t Do (also support vs. punishment) Figure out what might be going on in behavior. It is hard to do things that are hard – when faced with that – behaviors & emotions. Change to include our audience.")
2
_ to _% of children/youth have a LD
___% of children who have an LD also have a social, emotional or behavioural problem _ to _ % of kids with ADHD also have a LD ___% of children with ADHD who also have anxiety 1 in __ children and youth in Canada have a mental health disorder (which includes anxiety and depression) Co-morbid – explain term “roommates” ADHD has a lot of room mates (Behaviour and LDs most common) ADHD most likely suggested by teachers as an issue – because it is BEHAVIOURAL and can be observed. Not always the full story – teacher/school staff are in the best position to observe and watch for changes in behaviour, mood, trauma especially if there is a relationship however teachers need more info and training. You don’t need to solve/fix/diagnose. Need to observe, suggest and support.
 Co-morbid – explain term roommates ADHD has a lot of room mates (Behaviour and LDs most common) ADHD most likely suggested by teachers as an issue – because it is BEHAVIOURAL and can be observed. Not always the full story – teacher/school staff are in the best position to observe and watch for changes in behaviour, mood, trauma especially if there is a relationship however teachers need more info and training. You don’t need to solve/fix/diagnose. Need to observe, suggest and support.")
3
“Walk A Mile In My Shoes”
Learning Objectives: To introduce the concepts of Learning Disabilities (LDs) To experience what it might feel like to have LDs To talk about resources around anxiety and depression Brief introductions (recognition of their expertise in residential treatment); we have done this workshop for … but new to residential. Help us to understand what the kids day looks like, recognize that security is key Eliciting problem behaviors: What are the behaviors that are problematic / that wears you out/down? Want to elicit typical problems rather than horror stories Looking for top 10 Examples – telling a kid 10 times to their chores; not finishing the stuff they start;
 To experience what it might feel like to have LDs. To talk about resources around anxiety and depression. Brief introductions (recognition of their expertise in residential treatment); we have done this workshop for … but new to residential. Help us to understand what the kids day looks like, recognize that security is key. Eliciting problem behaviors: What are the behaviors that are problematic / that wears you out/down Want to elicit typical problems rather than horror stories. Looking for top 10. Examples – telling a kid 10 times to their chores; not finishing the stuff they start;")
4
What are learning disabilities?
Neurologically based disorders Affect the ability to take in, understand, remember or express information. Specific, not global impairments Found in individuals who possess average to above average thinking and reasoning skills Lifelong disorders

5
What are learning disabilities?
LDs reflect neurobiological factors, including genetics, congenital or acquired conditions LDs are not due to differences in culture, language, SES, motivation

6
What are learning disabilities?
Impairments in one or more of the following psychological processes: Language processing Phonological processing Visual-spatial processing Processing Speed Memory & attention Executive functioning Self disclosure Lingo is fluid – words – but meanings change, people use terms differently, Process – what is that word? Talk about phonol processing – what does this mean? Our experience like LD – read and may not get meaning – level of language is so dense – tackle it together And giving you a cheat sheet – use with clients, will go back to it Demonstrate this is our knowledge – not belonging to psychologists only in a report Talk about first 3 today – and next three in context of lD/ADHD For each one – activity first, discussion, info: terms, why NB in general, why for your kids? (what are implications/strategies)
")
7
What are learning disabilities?
Impairments may affect learning in the areas of: Reading Oral language Written language Math Dx of LD made when have average intelligence but problem with one of those processes we just listed. And the problem affects school skills – can be in one or more than one of these areas. As we go through the processes, we’ll try to show why the processes get in the way of reading or writing or math, for example.

8
What Do LDs Affect? LDs come in many forms & affect everyone differently Possible problems in social situations: Understanding sarcasm Figuring out how someone is feeling from their body language or facial expressions Understanding the unwritten social rules Participating in groups Marjory to lead

9
If a large solid-hoofed mammal becomes available to you without compensation, refrain from casting your faculty for seeing into the oral cavity of such a creature. Melissa to lead

10
Demystifying Processes
Term Description Application Verbal Reasoning Verbal Comprehension General Verbal Ability Ability to think through problems using words Ability to understand words and connected language Understanding instructions, lessons, stories Logical thinking and problem-solving Understanding word meanings Expressing ideas in words MP Link to exercise to underscore the following concepts: Need integration of processes to work out the answer – including: vocabulary (long-term memory), Logical Reasoning / strategies – how did you figure out how to start the problem? E.g., look for words you know, like mammal = animal Abstract reasoning – understanding metaphors & words with multiple meanings, eg even if figure out each word separately, may not have meaning Culture – age, context – how many don’t recognize the proverb? Anyone know of a similar saying in another language or culture?
, Logical Reasoning / strategies – how did you figure out how to start the problem E.g., look for words you know, like mammal = animal. Abstract reasoning – understanding metaphors & words with multiple meanings, eg even if figure out each word separately, may not have meaning. Culture – age, context – how many don’t recognize the proverb Anyone know of a similar saying in another language or culture")
11
Demystifying Processes
Term Description Application Perceptual processing Visual-spatial Ability to make sense of what one sees Putting together visual information Noticing & understanding facial expressions Understanding a chart or graph Reading a map

14
Demystifying Processes
Term Description Application Non-Verbal Reasoning Perceptual reasoning Visual-spatial Perceptual-organizational Performance Visual problem-solving Ability to organize, put together or orient visual information Ability to form and mentally manipulate images Understanding concept words related to time, space Building according to a plan or model Judging space and distance Math (geometry, shapes, measurement) Following sewing patterns, IKEA instructions
 Following sewing patterns, IKEA instructions.")
15
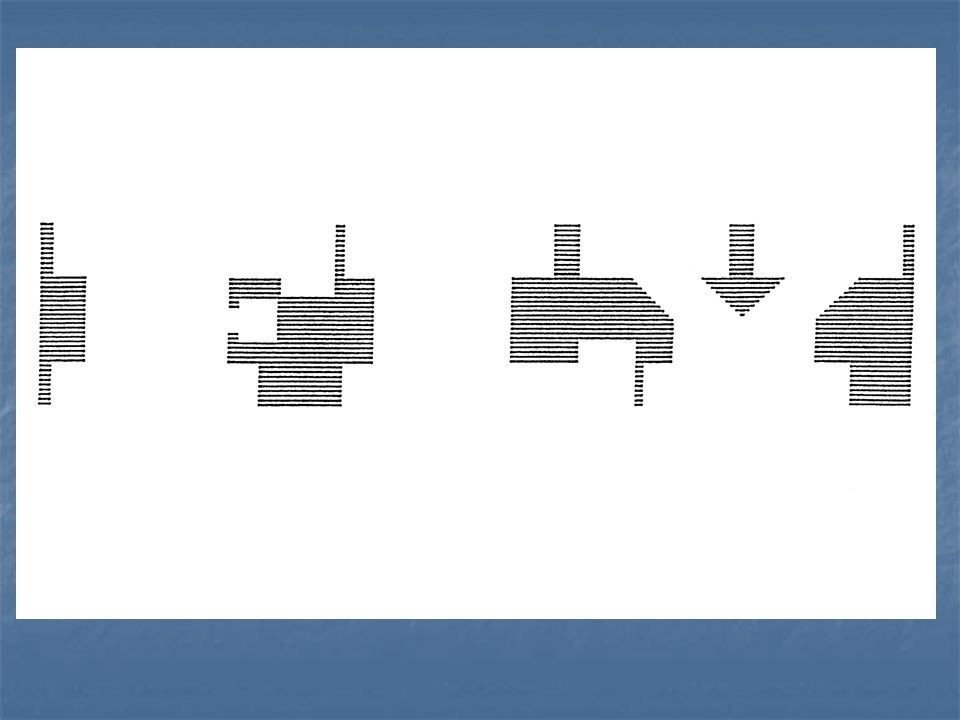
What symbol has to come next in the sequence of the five symbols on the left? Can you sketch this sixth figure? Answer is back-to-back 6 Cover up one side of each mirrored figure – elicit discussion about problem solving strategies. 15

16
What symbol has to come next in the sequence of the five symbols on the left? Can you sketch this sixth figure? MP to lead if time

17
Kids with LDs and other disabilities are at risk – why?
Frustration at not being able to do what child knows he/she should be able to do Feelings about having a “disability” Sense that others’ expectations are not being met (parents, teachers) Peers’ responses Lack of others’ understanding/responses Responses to others’ feelings & anxieties
 Peers’ responses. Lack of others’ understanding/responses. Responses to others’ feelings & anxieties.")
18
Invisible Disabilities
Neurobiological impairments are invisible. Mental Health Issues are invisible Behaviour may be are only clue. Where else can we look? OSR, past reports, grades, parents, teachers and kids OSR Ontario School Record – what is your equivalent?

19
What is Anxiety/worry? Diffuse uncomfortable sense of apprehension, often accompanied by autonomic symptoms” (Barlow, 2002) Basic human emotion Part of normal development Can be adaptive Lots of definitions of anxiety, depending on who you read. I like Barlow’s because it captures the uncomfortable nature of anxiety One of the basic human emotions – we all experience anxiety at some times, or at some stages of our lives. e.g., public speaking – one of the most common anxiety-producing experiences, Part of normal development – dependency to autonomy – exposed to new situations and learn to master your fear e.g. sleeping with light off as kid, starting new school, first day of high school, job interview Also has an important function – we need anxiety: Safety mechanism – hard-wired response to perceived danger – when we perceive threat, there is an increase in autonomic nervous system reactions – palms sweat, breath faster or more shallowly, feel butterflies in stomach – that works as an early warning mechanism – tells us something is up Cave man times – fight or flight

20
What is an Anxiety Disorder?
Symptoms interfere with the youth’s ability to function in everyday life Persistent Intensity of reactions is severe Anxiety disorders are relatively common in childhood: Prevalence rate of >10% Can look like skipping, lack of motivation, withdrawal, externalizing behaviour, “aggressive avoidance” So if anxiety is normal and we all have it, how do you know when it is a problem, especially a problem for your child or teen? Short answer: When it seriously interferes with the child’s ability to do the tasks of everyday life – e.g., restricts their ability to go to school or hang out with friends at the mall, or interferes with their concentration – can’t think about school work, can’t sleep When it is persistent – not just a period of time when a big change is happening – like child not sleeping well & distracted in grade eight, worrying about starting high school When the intensity of the child’s responses are outside the norm – when doing an assessment and making a diagnosis, we usually try to get information about the child from a variety of sources – the parents, school, sometimes extended family, watching the child in the assessment – often, people will notice something Research into anxiety disorders suggests that some of the anxiety disorders start fairly early , put a child vulnerable to developing other psychiatric problems, and if untreated, can persist into adulthood.

21
Types of Anxiety Disorders in Childhood
Generalized Anxiety Disorder (GAD) Social Phobia Specific Phobia Post-traumatic Stress Disorder (PTSD) Panic Disorder Obsessive-Compulsive Disorder (OCD) Separation Anxiety Disorder (SAD) TGeneralized Anxiety Disorder (GAS) % Obsessive-Compulsive Disorder (OCD) 1-3% Panic Attacks Rare in children, unless part of another anxiety disorder but more common in adolescents with specific phobias, Social phobia, SAD or GAD Posttraumatic Stress Disorder 1% of adults, unknown in children Separation Anxiety % of children under 7 These are the Anxiety Disorders in the Diagnostic and Statistical Manual (DSM) system – psychologists, psychiatrists use criteria to make a diagnosis. Diagnosis can be helpful for a couple of reasons: Short hand way of communicating information – Research – group kids with particular cluster of symptoms together – can do careful studies and learn what symptoms are part of the disorder and what are unique to the child – predict what to watch out for; and most importantly, to learn how to help these kids – what works and what doesn’t work Also – diagnosis is not the end point, though. Usually, understanding a child from a broader perspective – issues /stresses, how does a child feel; how do they cope? Bio-psycho-social model useful hese are the Anxiety Disorders in the Diagnostic and Statistical Manual (DSM) system – psychologists, psychiatrists use criteria to make a diagnosis.
 Social Phobia. Specific Phobia. Post-traumatic Stress Disorder (PTSD) Panic Disorder. Obsessive-Compulsive Disorder (OCD) Separation Anxiety Disorder (SAD) TGeneralized Anxiety Disorder (GAS) 2-5% Obsessive-Compulsive Disorder (OCD) 1-3% Panic Attacks. Rare in children, unless part of another anxiety disorder but more common in adolescents with specific phobias, Social phobia, SAD or GAD. Posttraumatic Stress Disorder 1% of adults, unknown in children. Separation Anxiety 3-5% of children under 7. These are the Anxiety Disorders in the Diagnostic and Statistical Manual (DSM) system – psychologists, psychiatrists use criteria to make a diagnosis. Diagnosis can be helpful for a couple of reasons: Short hand way of communicating information – Research – group kids with particular cluster of symptoms together – can do careful studies and learn what symptoms are part of the disorder and what are unique to the child – predict what to watch out for; and most importantly, to learn how to help these kids – what works and what doesn’t work. Also – diagnosis is not the end point, though. Usually, understanding a child from a broader perspective – issues /stresses, how does a child feel; how do they cope Bio-psycho-social model useful. hese are the Anxiety Disorders in the Diagnostic and Statistical Manual (DSM) system – psychologists, psychiatrists use criteria to make a diagnosis.")
22
What is Distress/sadness
Always associated with a trigger, event or situation Will improve with environmental accommodation or removal of stressor Functional impairment usually mild Professional psychiatric treatment not usually necessary Counselling and therapy will often help Social supports (friendships and family) will often help Medications would not be normally used
 will often help. Medications would not be normally used.")
23
What is Depression? Referred to as Major Depressive Disorder -MDD
Characterized by: Feelings of hopelessness, sadness Loss of interest in activities Vegetative signs: change in eating or sleeping, low energy or fatigue Poor concentration, difficulty making decisions Persistent Interferes with daily living Rare in children under 12 years old -

24
Depression in Childhood
Diagnosis of Depression is often overlooked in childhood: Some symptoms are more typical of children than of adults (e.g., irritability) High co-occurence with other disorders (such as ADHD & behavioual issues) may mask the symptoms Certain features of Depression are more typical at different ages Perception that kids don’t get depressed. Also – really hard to diagnose accurately. What it looks like changes over time. - e.g., depressed mood – feeling sad or hopeless & looking tearful for younger kids, often is manifest as irritable mood. Loss of interest in activities – may not be in all activities with kids. Can have a kid who still plays his DS every day but does not want to play with other kids or may not take pride in his ability to get to the next level, eg.
 High co-occurence with other disorders (such as ADHD & behavioual issues) may mask the symptoms. Certain features of Depression are more typical at different ages. Perception that kids don’t get depressed. Also – really hard to diagnose accurately. What it looks like changes over time. - e.g., depressed mood – feeling sad or hopeless & looking tearful for younger kids, often is manifest as irritable mood. Loss of interest in activities – may not be in all activities with kids. Can have a kid who still plays his DS every day but does not want to play with other kids or may not take pride in his ability to get to the next level, eg.")
25
When to ask for more help
When you are concerned about safety or well being of student Watch for obvious indicators of mood issues: Crying, shaking, avoidance Freezing in classroom situations Angry Outbursts & Increased Irritation Physical Evidence of Self-Harm or Decline Watch for changes: In behaviour In Hygiene In peer interactions In interactions with teachers and school staff When

26
What would help worry/distress at school?
Involve student in problem-solving process (they have great ideas!) Acknowledge effort even if output is weak Encourage & support accountability Address barriers caused by LD, ADHD, OT, Note taking Scheduling Planning & Organizing (Support Self-Reliance)
 Acknowledge effort even if output is weak. Encourage & support accountability. Address barriers caused by LD, ADHD, OT, Note taking. Scheduling. Planning & Organizing (Support Self-Reliance)")
27
What would help worry/distress at school?
Make sure learning style is understood Are accommodations appropriate and sufficient? Watch for bullying or peer difficulties Teach pro-social skills to entire class and be clear about classroom expectations Discuss Fair versus Equal

28
What would help worry/distress at school?
Find out what is overwhelming them in the school setting & accommodate Set up student for success and mastery to build self-esteem Watch for activities/subjects/projects that are “too hard” Empower them by encouraging and being receptive to attempts at self-advocacy

29
Support & Listen Reach Out - Ask student if they’re alright
Ask about any changes in their life Check in with other teachers, peers, their family Be Real about limits of confidentiality Always encourage parental involvement May chose to state policy outright Never promise you won’t tell anyone

30
Suggest Help In school support
School Team (rule out learning issues, bullying, or situation within class) Social Workers Guidance Special Education Administrators
 Social Workers. Guidance. Special Education. Administrators.")
31
Suggest a Referral Inform family and student of your concern
Enlist the help of your team Encourage a thorough assessment Be open to school involvement in treatment Outside Referral for Assessment & Treatment: Hospital Clinic or Program Children’s Mental Health Clinic GP

32
Resources GP’s will know local referral sources: Hospital Clinics
Children’s Mental Health Clinics Specialty Clinics (Integra, Sick Kids Anxiety Groups, CAMH First Episode Clinic) Pediatricians and specializing psychiatrists and psychologists Private practitioners (play therapists, social workers, therapists) – only after a thorough assessment
 Pediatricians and specializing psychiatrists and psychologists. Private practitioners (play therapists, social workers, therapists) – only after a thorough assessment.")
33
Resources – Websites & Books
Sick Kids – Information and Resources – “Trusted Answers” Information on Referral Sources Resources for Teachers TeachADHD The ABCs of Mental Health – A Teacher Resource Orientation to Children’s Mental Heath – Teachers Guide Learning Disability Association of ON

Similar presentations