Download presentation
Presentation is loading. Please wait.

1
폐렴으로 오인할 수 있는 폐렴 외 질환 호흡기 내과 R3 최 문 찬

2
Nonresolving Pneumonia Non-infectious mimics of CAP
Contents 1 Nonresolving Pneumonia 2 Non-infectious mimics of CAP

3
Introduction NORMAL VERSUS DELAYED RESOLUTION OF PNEUMONIA
- Patients typically note subjective improvement within 3 to 5 days of treatment - “Slow resolution” often being defined as the persistence of radiographic abnormalities for greater than one month in a clinically improved host

4
Nonresolving Pneumonia
Comorbidities Age Severity Infectious agent Non-infectious etiology

5
Nonresolving Pneumonia
Comorbidities * Only 20 to 30 percent of patients with a comorbid condition will clear Chest X-ray by 4 weeks

6
Nonresolving Pneumonia
Age - Only 30% of patients older than 50 years of age show radiographic resolution by 4 weeks Severity - Radiographic resolution of severe pneumonia is estimated at 10 weeks, compared with 3 to 4 weeks for mild to moderate pneumonia Infectious agent - Resolution is more rapid with Mycoplasma pneumoniae, non-bacteremic Streptococcus pneumoniae, Chlamydia species, and Moraxella catarrhalis than with other organisms

7
Nonresolving Pneumonia

8
Nonresolving Pneumonia
MISDIAGNOSIS OF NONBACTERIAL PATHOGENS - Unusual pathogens causing nonresolving pneumonia Pathogen Population at risk Myocobacterium tuberculosis Elderly, immigrants, HIV Atypical myobacteria (Bronchiectasis) COPD, HIV Nocardia (Nocardiasis) Immunocompromised host Actinomyces israelii (Actinomycosis) Aspiration risk, chest wall involvement Aspergillus (Aspergillosis)
 COPD, HIV. Nocardia (Nocardiasis) Immunocompromised host. Actinomyces israelii. (Actinomycosis) Aspiration risk, chest wall involvement. Aspergillus. (Aspergillosis)")
11
Nonresolving Pneumonia
RESISTANT BACTERIAL PATHOGENS - Penicillin-resistant S. pneumoniae

12
Nonresolving Pneumonia
RESISTANT BACTERIAL PATHOGENS - Suspicion of Penicillin-resistant S. pneumoniae 1) Prior treatment with a beta-lactam antibiotic (within 6 months) 2) Previous pneumonia within the past year 3) Hospitalization within the past three months 4) Hospital-acquired (nosocomial) infection
 Prior treatment with a beta-lactam antibiotic (within 6 months) 2) Previous pneumonia within the past year. 3) Hospitalization within the past three months. 4) Hospital-acquired (nosocomial) infection.")
13
Nonresolving Pneumonia
DEVELOPMENT OF COMPLICATIONS FROM THE INITIAL PNEUMONIA - Empyema ; Rare complication of CAP ; Demonstration of any significant amount of pleural fluid should prompt consideration of a diagnostic thoracentesis to rule out empyema - Lung abscess ; Alcoholism, seizures, poor oral hygiene, and aspiration ; Chest CT scan is more sensitive for diagnosis

14
To assess noninfectious or unusual infectious diseases that may be misdiagnosed as CAP that progresses with treatment failure 180 patients with presumptive diagnosis of CAP

15
Respiratory Medicine (2004) 98, 488–494
 98, 488–494")
16
Respiratory Medicine (2004) 98, 488–494
 98, 488–494")
17
NONINFECTIOUS ETIOLOGIES
Neoplastic disorders Drug toxicity - Bronchogenic carcinoma Pulmonary vascular abnormalities - Bronchoalveolar cell carcinoma Congestive heart failure - Lymphoma Pulmonary embolism Immunologic disorders - Vasculitis : Wegener’s granulomatosis Diffuse alveloar hemorrhage - Bronchiolitis obliterans-organizing pneumonia (BOOP) - Eosinophilic pneumonia syndromes : Acute eosinophilic pneumonia Chronic eosinophilic pneumonia - Acute interstitial pneumonia - Pulmonary alveolar proteinosis - Sarcoidosis
 - Eosinophilic pneumonia syndromes : Acute eosinophilic pneumonia. Chronic eosinophilic pneumonia. - Acute interstitial pneumonia. - Pulmonary alveolar proteinosis. - Sarcoidosis.")
18
Neoplastic disorders Bronchogenic carcinoma
- Compromises the airway lumen either through endobronchial involvement or extrinsic compression - Range from 0 to 8 % as cause of nonresolving pneumonia Carcinoid tumor - Cause endobronchial obstruction, postobstructive pneumonia - Young or nonsmoking patient

19
Neoplastic disorders Bronchioloalveolar cell carcinoma and Lymphoma in the lung - May present as a focal infiltrate, often with air bronchograms BAC Lymphoma

20
Inflammatory disorders
Systemic vasculitis or a connective tissue disorders - Can cause fever, dyspnea, and pulmonary infiltrates - Wegener’s granulomatosis and alveolar hemorrhage syndromes

21
Inflammatory disorders
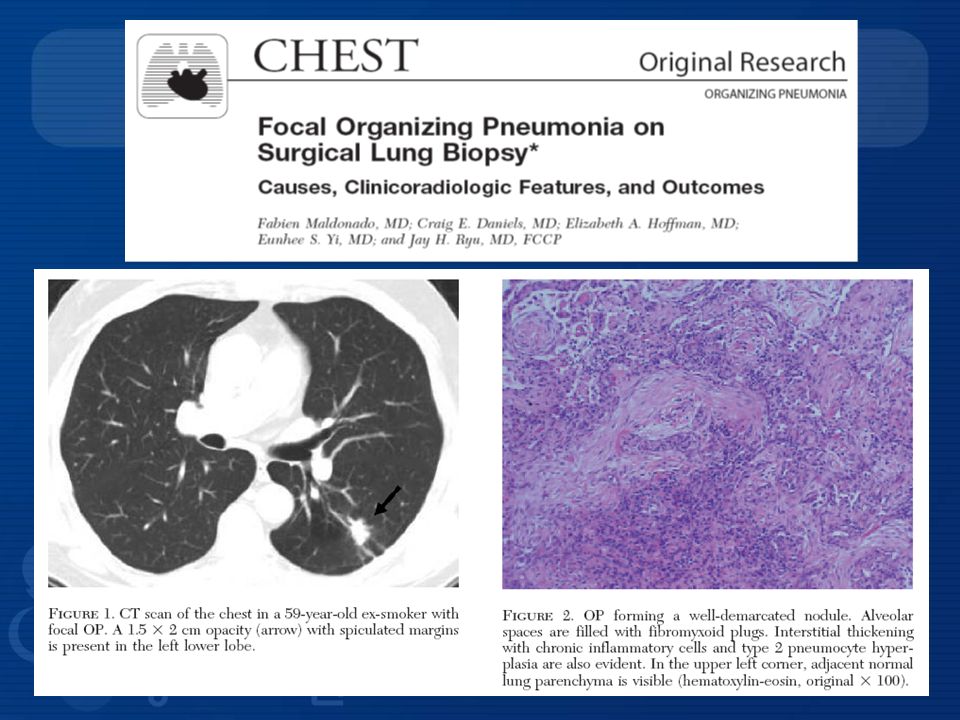
Bronchiolitis obliterans organizing pneumonia (BOOP) - Begins with a flu-like illness mimicking an atypical (community-acquired) pneumonia, with fever, malaise, fatigue, dyspnea, and dry cough - Patchy alveolar infiltrates are typically present on chest radiograph
 - Begins with a flu-like illness mimicking an atypical (community-acquired) pneumonia, with fever, malaise, fatigue, dyspnea, and dry cough. - Patchy alveolar infiltrates are typically present on chest radiograph.")
23
Inflammatory disorders
Eosinophilic pneumonias - Chronic eosinophilic pneumonia ; Subacute illness with cough, fever, dyspnea, weight loss, wheezing, night sweats, and radiographic infiltrates appearing over weeks to months ; Patchy, nonsegmental alveolar infiltrates that predominantly affect the periphery of the lungs - Acute eosinophilic pneumonia ; Subtle reticular or ground-glass infiltrates, which can progress to bilateral diffuse alveolar disease

24
Drug-induced Lung Disease
Amiodarone pulmonary toxicity - Can confused with an infectious pneumonia - May have acute presentation with focal alveolar infiltrates

25
Summary Approach to nonresolving pneumonia

Similar presentations
 Infections (pneumonia, airways disease)>")











 Dr. Meg-angela Christi Amores.>")






