Download presentation
Presentation is loading. Please wait.

1
SONG QIANG Department of Radiology, Affiliated Hospital of Xuzhou Medical College Urinary tract and male reproductive system

2
Investigation of a renal mass P130

3
The goals of imaging a suspected renal mass 1.Confirmation of presence and site of mass. 2.Classification into simple cyst, complicated cyst or solid mass. 3.Assessment of contents, in particular the presence of fat. 4.Differentiation of benign from malignant. 5.Diagnosis of complications such as local invasion, venous invasion, lymphadenopathy and metastases.

5
The commonest cause of a renal mass in an adult is a renal cyst. Renal cysts are usually small and asymptomatic, and usually discovered incidentally on CT or US examinations of the abdomen.

6
Renal cysts are commonly encountered lesions in daily radiological practice. Usually these are simple benign cysts, but they can become complicated in case of hemorrhage, infection and ischemia. When this occurs it can be difficult to differentiate these complicated cysts from cystic renal cell carcinomas (10% of all renal cell carcinomas)
.")
7
Since the only treatment for renal cell carcinoma is surgery or ablation, we need to recognize these cystic renal cell carcinomas. Imaging is a reliable means for differentiating benign from malignant cystic lesions.

8
They may be found anywhere in the renal parenchyma but most often develop within the cortical layer. Occasionally, haemorrhage or infection may thicken the cyst. On CT a simple cyst usually appears as a well-defined rounded mass with an attenuation value of 0–20 Hu (Hounsfield Unit ), with an imperceptible wall and no enhancement after injection of contrast medium.
, with an imperceptible wall and no enhancement after injection of contrast medium..")
9
The MRI appearance of a simple renal cyst is characterized by a sharply demarcated, homogeneous, hypointense mass on T1-weighted images, which becomes uniformly hyperintense on T2-weighted images and shows no enhancement following contrast medium administration.

10
Radiological Interpretation Although the final differentiation of cystic renal masses is based upon histologic diagnosis, there are imaging findings that tell you that a cyst is not a simple cyst and whether it is probably benign or malignant. The following imaging features indicate that a cyst is NOT simple: - Calcification - Hyperdense / high signal - Septations - Multiple locules - Enhancement - Nodularity / wall thickening

11
calcification There is a small punctate calcification that we can ignore. On the bottom of the cyst there is a layer of calcium typical for milk of calcium. This is also a benign calcification that we can ignore.

12
a patient with nefrolithiasis( 肾结石 ). RIGHT: NECT with a smooth linear calcification and nodular calcification. LEFT : Enhanced CT shows enhancement...... Excise There is also a cystic lesion with linear and nodular calcification. If there were only these linear calcifications we could ignore the lesion. In case of nodular calcification we can follow it, if there is no enhancement. In this case however we see enhancement, so this lesion has to be excised.

13
Hyperdense or High signal On CT hyperdense means: > 20 HU on a NECT On MRI hyperintense means all that has higher signal intensity than water on a T1 weighted image. Hyperdensity or hyperintensity usually indicates hemorrhage or high protein content of the cyst. Ignore all lesion with sharp margins; lesions On US they have to be clearly cystic Follow all lesions that are totally intrarenal, because you can not appreciate the wall and follow all lesions > 3 cm, because there is at the moment not much experience with these lesions. All these lesions must show no enhancement. Excise all lesions that are poorly defined or heterogenous or show enhancement. Also when ultrasound shows that the lesion is solid, the lesion should be excised.

14
RIGHT : NECT shows a lesion with a density of 27 HU.....Ignore LEFT : MRI shows a intrarenal lesion that is hyperintense on T1: higher signal than water...... Follow On the left we see a hyperdense cystic lesion on CT and a hyperintense lesion on a T1-weighted MR. Both lesions have a sharp margin and are homogeneous, although there is some noise in the CT image. On the enhanced scans (not shown) the lesions didn't show any enhancement. We therefore can ignore the lesion on the left and we have to follow the lesion on the right, because it is totally intrarenal.
 the lesions didn t show any enhancement. We therefore can ignore the lesion on the left and we have to follow the lesion on the right, because it is totally intrarenal..")
15
Septations Ignore thin septations ( Follow all septations that are only slightly greater than hairline. They still have to show no enhancement. Excise all septations that are thick, irregular or nodular and all septations that show enhancement.

16
RIGHT : thin, smooth septation.....Ignore LEFT : thick enhancing septation..... Excise There is a cystic lesion with a thin smooth non enhancing septation that we can ignore. The other case is a thick enhancing septation that has to be excised.

17
Enhancement Enhancement is our best predictable sign of malignancy. So we have to excise all lesions, that clearly show enhancement. The only exception is infection.

18
Enhanced CT shows enhancement of a thick wall and a central area.....excise The case on the left doesn't shows much on the NECT. However when we give contrast we can appreciate a thick wall and we see enhancement both of the wall and of a central area in the medial part of the cystic lesion. We should never see this in an benign cyst, so this is a surgical lesion.

19
Multiloculated Masses with three or more septa are not called multiseptated but multiloculated. All multiloculated lesions should be excised, unless there is clear evidence of infection.

20
In the adult, the two most common multiloculated masses are MLCN (multilocular cystic nephroma) which is usually benign, but sometimes malignant and MLRCC (multilocular renal cell carcinoma) which is always malignant. On imaging there is no way that we can separate these two and therefore, all multiloculated masses are surgical (unless infection).
..")
21
Nodularity Ignore: none Follow: only very small nonenhancing nodules, and follow carefully Excise: all other nodular lesions

22
Very small non enhancing nodules.....Follow The case on the left shows very small nodules on a CECT and a T2WI. From all the other images we could tell that they were not enhancing. So we can probably follow this lesion. If they start to grow or show any enhancement, then we have to excise the lesion.

23
Cystic lesion with a big enhancing nodule..... Excise There is a big nodule with enhancement, so this lesion has to be excised. Even if there was no enhancement, the lesion still had to be excised.

24
Wall thickening All lesions with a thickened wall, with or without enhancement, should be excised, unless there is clear evidence of infection. In these latter cases the lesions should be followed.

25
Two cystic lesions with a regular thick wall..... Excise we see two renal lesions that are cystic. The lesion on the right clearly shows a thickened wall. This is easy to appreciate because part of the lesion is exterarenal. The cystic lesion next to it is totally interarenal, which makes it harder to appreciate, but there is wall thickening. So both lesions have to be excised, whether there is enhancement of the wall or not. The only exception would be if there were evident signs of infection.

26
Cystic lesion with a thick irregular enhancing wall..... Excise The cystic lesion on the right is clearly a surgical lesion. It has a thick irregular wall, it is exterarenal and shows enhancement.

27
The presence of a soft-tissue mass in association with a cyst usually implies a cystic renal cell carcinoma.

28
Angiomyolipomas AMLs are usually small and asymptomatic and as with cysts, are often discovered incidentally.

29
Angiomyolipomas contain fat, giving them a characteristic appearance on CT. Eighty percent of AMLs occur sporadically; 20 percent occur in association with tuberous sclerosis 结节性硬化 and are often multiple.

30
Angiomyolipomas

31
Contrast-enhanced CT is used for further characterization of a solid lesion or complex cyst. Computed tomography is more accurate than US for characterization of internal contents of a mass, particularly to show areas of fat confirming the diagnosis of AML.

32
renal cell carcinoma. The commonest malignant renal mass is renal cell carcinoma.

33
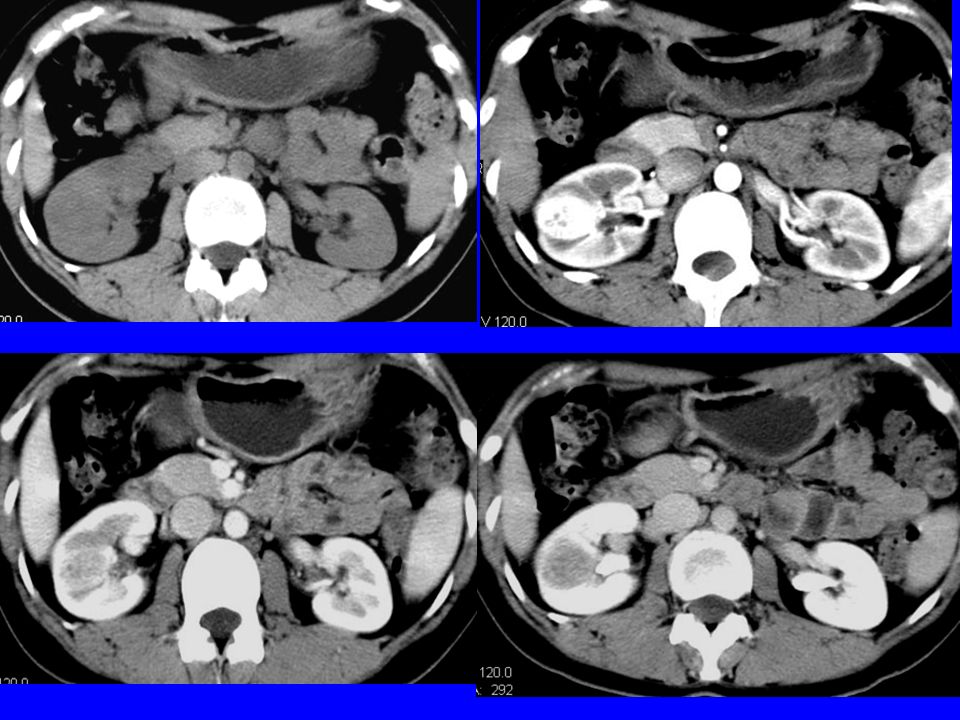
The more common appearance of renal cell carcinoma is a heterogeneous soft-tissue mass that enhances with intravenous contrast material.

34
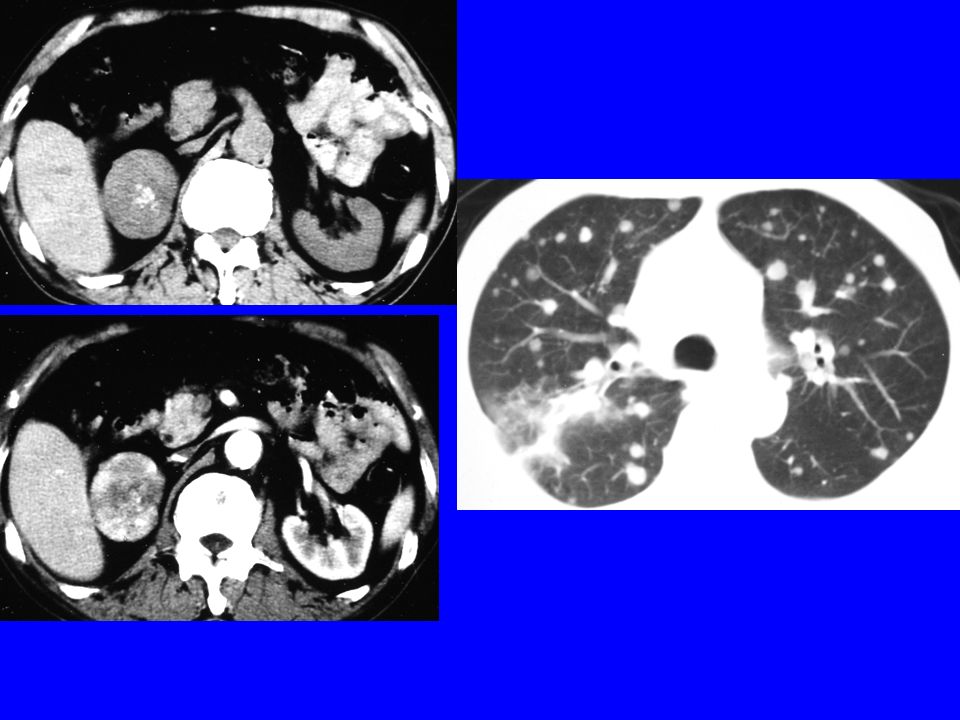
Computed tomography is also used for staging of renal cell carcinoma. Factors relevant to staging detected on CT include invasion of local structures such as psoas muscle, vascular invasion of renal vein or IVC, lymphadenopathy, metastases in the liver and tumour in the other kidney.

35
The differential diagnosis for multiple non- fat-containing renal masses would include lymphoma and metastases.

37
Magnetic resonance imaging MRI gives similar information to CT in the detection, classification and staging of renal cysts and tumours. Because MRI is able to difine soft-tissue septations and masses.

38
MRI can be used to detect and stage renal cell carcinoma, with a similar sensitivity to CT. However, CT is better at detecting small foci of calcification. The signal characteristics of renal carcinoma are variable, with tumours appearing isointense or hypointense compared to the renal cortex on T1 sequences, and slightly hyperintense on T2-weighted sequences. Following administration of gadolinium, heterogeneous enhancement occurs immediately, decreasing on delayed images.

39
The advantages of MRI in imaging renal masses 1. Iodinated contrast material is not required, though gadolinium is injected. 2. More accurate for assessing venous invasion. 3. Multiplanar imaging gives more accuracy in assessing the renal poles, and for showing invasion of surrounding structures.

40
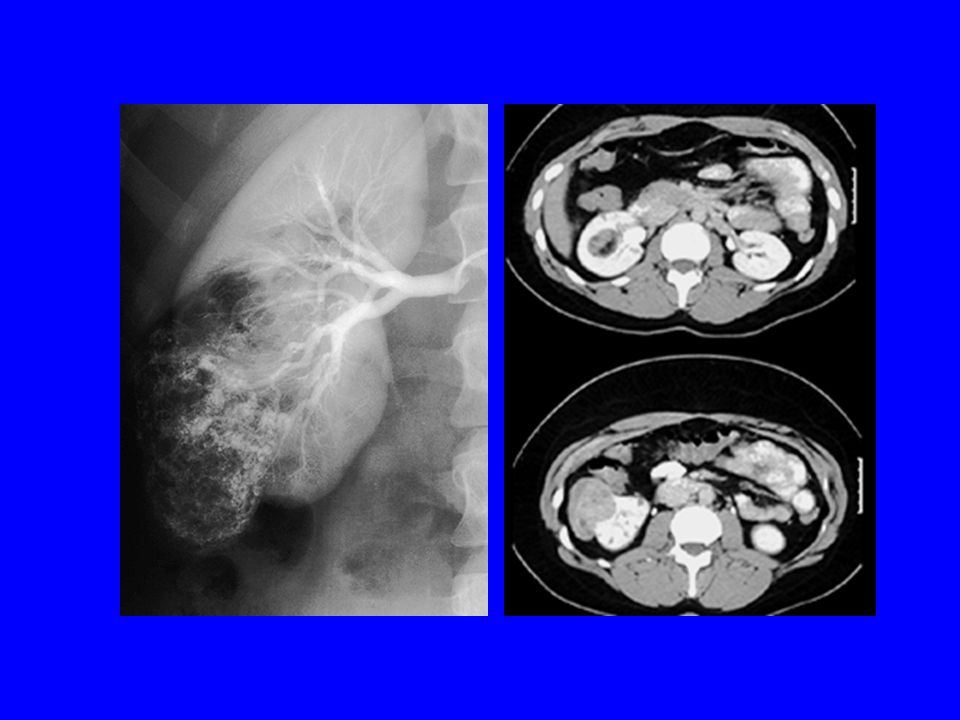
Angiography Catheter angiography may be performed if tumour embolization is required before surgery. This may be done for haemorrhage complicating a large angiomyolipoma or with a highly vascular renal cell carcinoma.

42
Thanks for Your Attention

Similar presentations


















 MRCS Urology SpR Edith Cavell Hospital.>")
