Download presentation
Presentation is loading. Please wait.

2
Ovarian Cystic Masses Atoosa Adibi MD. Department of radiology
Isfahan University Of Medical Sciences

3
The finding of an adnexal cyst causes considerable anxiety in women due to the fear of malignancy. However, the vast majority of adnexal cysts - even in postmenopausal women - are benign

4
Step 1 If a cystic pelvic mass is present, the first step is to find out if it is ovarian or non-ovarian in origin.

5
Step 2 The next step is to determine if the lesion can be categorized as one of the common, benign ovarian masses (simple cyst, hemorrhagic cyst, endometrioma or mature cystic teratoma), or is indeterminate.
, or is indeterminate.")
6
Step 3 To aid in selecting the proper work-up, the final step is to determine whether a patient falls into a low-risk category (i.e. premenopausal women without additional risk factors) or a high-risk category (i.e. post- menopausal or premenopausal with additional risk factors).
 or a high-risk category (i.e. post- menopausal or premenopausal with additional risk factors)..")
7
Based on these steps we can determine further management: ignore, follow-up with US, further evaluation with MRI or excision.

10
Role of imaging

11
Role of Ultrasound For characterization of ovarian masses, ultrasound is often the first- line method of choice, especially for distinguishing cystic from complex cystic-solid and solid lesions.

12
Role of CT CT is useful for the N- and M-staging of proven malignant lesions.

13
Role of MRI For complex lesions, primary evaluation with ultrasound is often followed by MRI. Even with MRI it is often not possible to make an accurate diagnosis of neoplastic subtype. By using MRI as an adjunct to sonography a delay in the treatment of potentially malignant ovarian lesions is prevented. This is not only beneficial to the small number of women who do have ovarian cancer, but also a proven cost-effective approach to the management of sonographically indeterminate adnexal lesions.

14
If a cystic adnexal mass is present and you suspect an ovarian origin, the first thing to do is try to identify the ovaries. If the gonadal vessels lead to the lesion with no separately identifiable normal ovaries, then most likely you are dealing with an ovarian lesion. If both ovaries are separately identifiable from the lesion, you are dealing with a non-ovarian cystic lesion, or a lesion that mimics a cystic mass.

15
The next step would be to check if there is uni- or bilateral disease and to look for any solid components that may indicate malignancy. Also look for secondary findings like ascites, enlarged lymph nodes and peritoneal deposits.

17
MDCT Scan A helpful tool to identify the ovaries is to follow the ovarian veins caudally. Scroll through the CT- images and follow the right ovarian vein from where it joins the inferior vena cava, and the left ovarian vein where it joins the left renal vein, until you identify the ovaries.

18
Ultrasound pattern recognition

19
Simple cyst Anechoic lesion with posterior acoustic enhancement
Unilocular Thin, smooth walls No solid or well-vascularized components None of these isolated unilocular cysts turned out to be ovarian cancer

21
In women of reproductive age, cysts up to 3 cm are a normal physiologic finding. These simple physiologic cysts do not need to be described in the imaging report and do not require follow-up

22
Cysts up to 7 cm in both pre- and postmenopausal woman are almost certainly benign.
Cysts larger than 7 cm may be difficult to assess completely with US and therefore further imaging with MR or surgical evaluation should be considered.

24
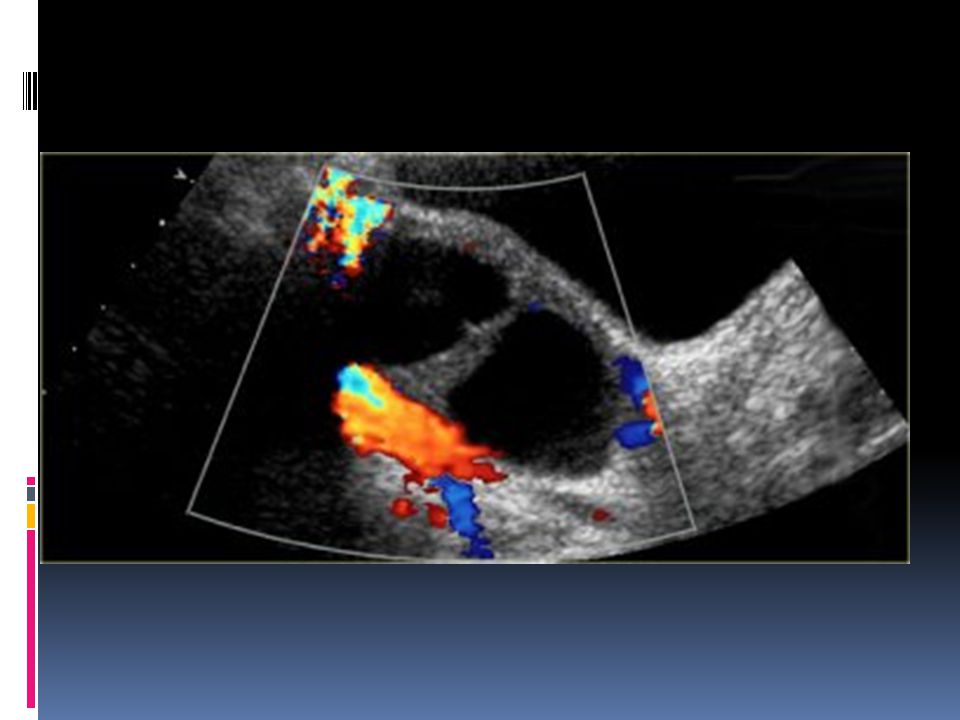
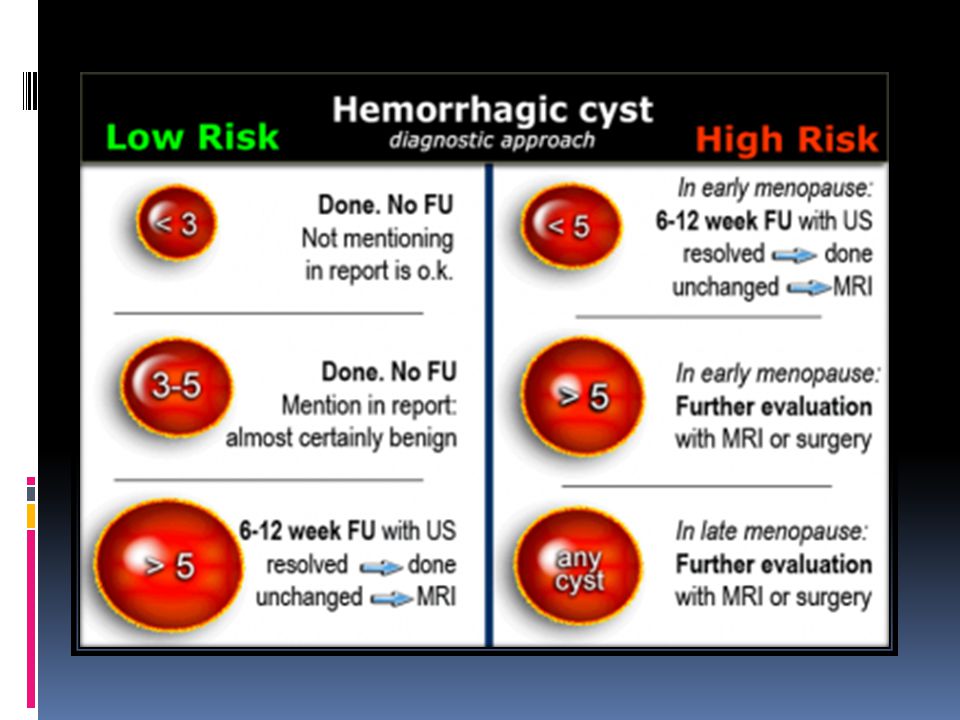
hemorrhagic ovarian cyst are:
Low risk patient Cystic mass < 5 cm with a reticular pattern due to fibrin strands or with diffuse low-level echoes The cyst may contain a solid- appearing area with good through-transmission, without internal flow at color Doppler, and typically with concave margins, consistent with a blood clot

26
Differential diagnosis
When hemorrhagic cysts present with diffuse low- level echoes, their appearance can be similar to that of endometriomas. In the acute phase may be completely filled with low-level echoes, simulating a solid mass. Clot in a hemorrhagic cyst may occasionally mimic a solid nodule in a neoplasm. ( concave borders VS outwardly convex borders) In both cases there will be no internal flow at Doppler US and there will be good through- transmission. Hemorrhagic cysts typically resolve within 8 weeks.
 In both cases there will be no internal flow at Doppler US and there will be good through- transmission. Hemorrhagic cysts typically resolve within 8 weeks.")
28
Hemorrhagic ovarian cyst

29
Endometrioma Homogeneous and hypoechoic mass
Diffuse low-level echoes (ground-glass) No internal flow at color Doppler No enhancing nodules or solid masses In 30% echogenic foci are seen within cyst wall In women of any age, probable endometriomas require initial 6-12 week follow-up to rule out a hemorrhagic cyst. Until surgically removed, endometriomas require follow-up with ultrasound, for example on a yearly basis.
 No internal flow at color Doppler. No enhancing nodules or solid masses. In 30% echogenic foci are seen within cyst wall. In women of any age, probable endometriomas require initial 6-12 week follow-up to rule out a hemorrhagic cyst. Until surgically removed, endometriomas require follow-up with ultrasound, for example on a yearly basis.")
32
Mature cystic teratoma
Hypoechoic mass with hyperechoic nodule (Rokitansky nodule or dermoid plug) Usually unilocular (90%) May contain calcifications (30%) May contain hyperechoic lines caused by floating hair May contain a fat-fluid level, i.e. fat floating on aqueous fluid
 Usually unilocular (90%) May contain calcifications (30%) May contain hyperechoic lines caused by floating hair. May contain a fat-fluid level, i.e. fat floating on aqueous fluid.")
35
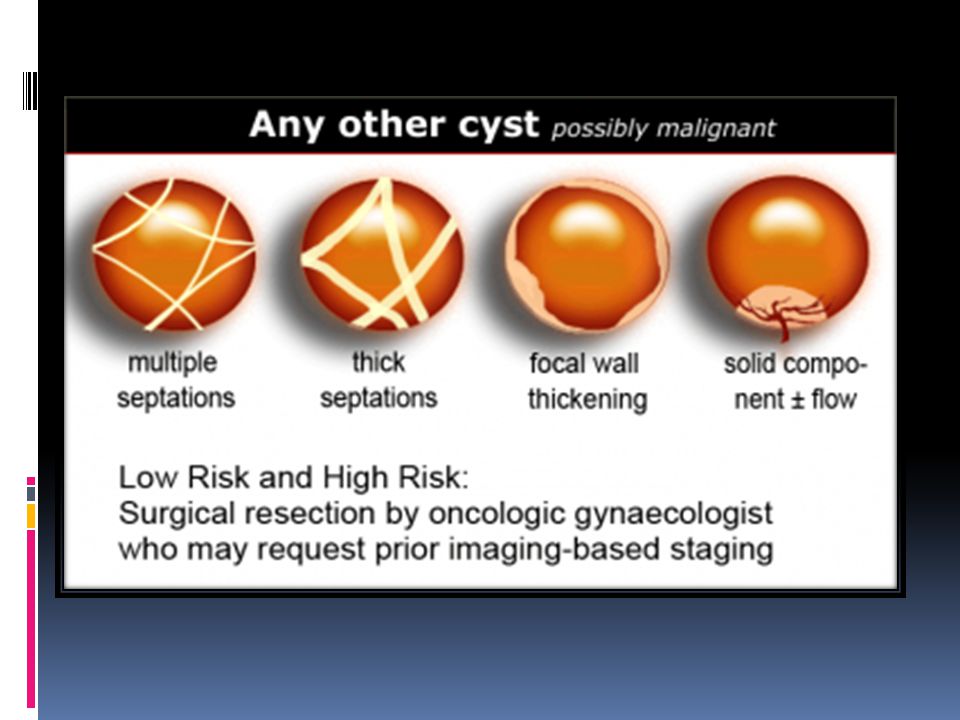
Any other cyst - possible neoplasm
All other cystic lesions are regarded as possibly neoplastic and therefore possibly malignant. Surgical resection is needed by an oncologic gynaecologist, who may request prior imaging-based staging.

37
Findings indicating possible neoplasm:
Large size While benign lesions can be very large, the likelihood that a lesion is neoplastic increases with size. Also the likelihood that a neoplastic lesion is malignant, increases with the size of the lesion. Vascularized septations The presence of septations indicates a possible neoplasm. When septations have a thickness of more than 3mm and are well-vascularized - while non-specific - both increase the likelihood that a neoplasm is malignant. Vascularized solid components Vascularized nodularities, papillary projections, or frank solid masses all increase the likelihood of a neoplastic nature.

38
Vascularized thick, irregular wall Lesions with thin walls are more often benign and lesions with thick, irregular walls are more often malignant. However, there is some overlap, making wall thickness a less useful criterion. For example a corpus luteum cyst may also have a thickened, vascularized wall. Secondary findings associated with malignant lesions: Large quantities of ascites, lymphadenopathy and peritoneal deposits are strongly associated with an increased likelihood of malignancy.

40
The final decision to ignore, follow or excise a cystic ovarian lesion is based on:
Morphology of the lesion on US, CT or MRI Risk group (low versus high) Symptomatic lesion versus incidental finding Additional findings such as ascites, lymphadenopathy or peritoneal implants
 Symptomatic lesion versus incidental finding. Additional findings such as ascites, lymphadenopathy or peritoneal implants.")
41
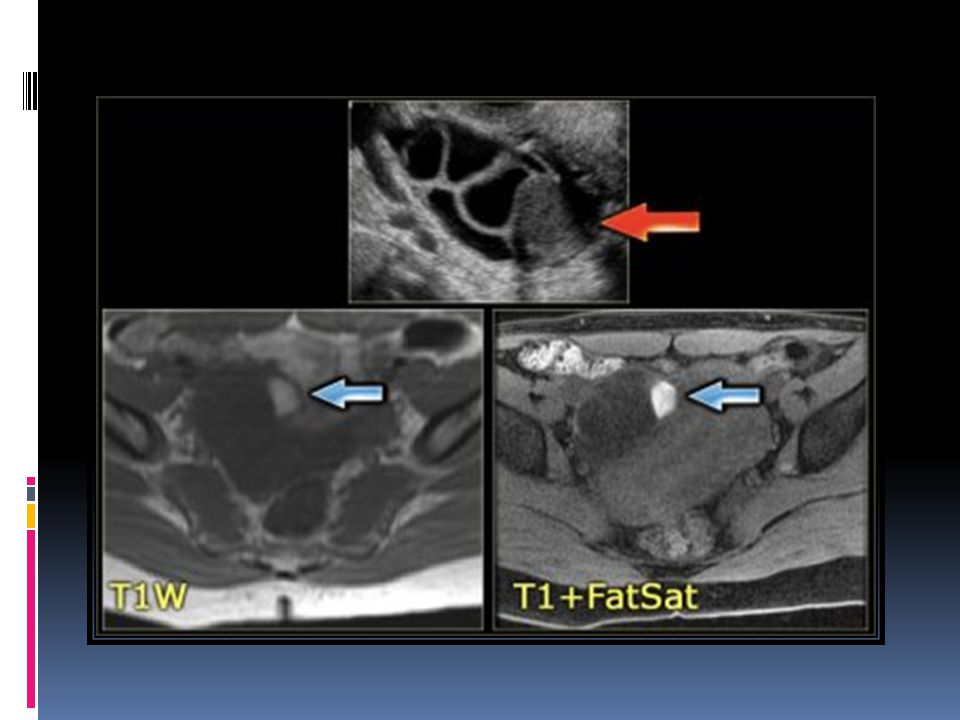
MR imaging is a valuable adjunct to US, as it allows identification of blood products within hemorrhagic masses that may mimic solid tumor at US. Fat-suppressed T1-weighted MR images may reveal small amounts of fat, which allows the diagnosis of a mature teratoma ('dermoid'). Contrast-enhanced T1-weighted MR imaging depicts features of malignancy such as enhancing mural nodules and/or enhancing solid areas with or without necrosis .
. Contrast-enhanced T1-weighted MR imaging depicts features of malignancy such as enhancing mural nodules and/or enhancing solid areas with or without necrosis ..")
45
Ovarian hyperstimulation syndrome - Theca lutein cysts

46
PID with tubo-ovarian abscess

47
Cystadenoma and cystadenofibroma
Cystadenoma and cystadenofibroma are also common benign ovarian tumors. They can be either serous or mucinous. At imaging a serous cystadenoma is most often unilocular and anechoic, and may look like a simple cyst. Mucinous cystadenomas are most often multilocular with thin (< 3 mm) septations. The locules may contain complex fluid, due to proteinaceous debris or hemorrhage, or both. The finding of papillary projections should raise the suspicion of a possible borderline malignancy or a cystadenocarcinoma.
 septations. The locules may contain complex fluid, due to proteinaceous debris or hemorrhage, or both. The finding of papillary projections should raise the suspicion of a possible borderline malignancy or a cystadenocarcinoma.")
50
On the posterior wall a solid mural nodule is found, which is avascular. No secondary signs of malignancy The lesion was resected and was found to be a cystadenofibroma

51
Malignant cystic ovarian neoplasms
guide decisions on further management

53
serous ovarian cystadenocarcinoma.

54
Mucinous ovarian cystadenocarcinoma

55
complex solid-cystic lesion

56
CT of the same patient confirms large bilateral complex solid-cystic lesions, bulging into the abdomen. The purpose of the CT is not to confirm what was already known from the ultrasound, but to stage disease.

57
Endometrioid ovarian carcinoma

58
Note that while peritoneal implants are M0 (do not count as metastatic disease), the finding of a peritoneal implant < 2cm such as this, immediately bumps the patients to a stage T3b (FIGO IIIB), which significantly influences management and prognosis.
, the finding of a peritoneal implant < 2cm such as this, immediately bumps the patients to a stage T3b (FIGO IIIB), which significantly influences management and prognosis.")
59
Cystic metastases to the ovaries
most commonly solid - such as for example Krukenbergs metastases - cystic ovarian metastases do occur. The CT image shows complex cystic masses in both ovaries. While a serous cystadenocarcinoma may very well be bilateral, they are more often unilocular than multilocular.

60
a circumferential colorectal cancer (blue arrow)
a circumferential colorectal cancer (blue arrow). cystic implants on the peritoneal reflection (red arrow). These were cystic ovarian metastases of a colorectal cancer
. cystic implants on the peritoneal reflection (red arrow). These were cystic ovarian metastases of a colorectal cancer.")
Similar presentations