Download presentation
Presentation is loading. Please wait.

1
Journal Club 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi 2016 年 1 月 7 日 8:30-8:55 8階 医局 Pfeffer MA, Claggett B, Diaz R, Dickstein K, Gerstein HC, Køber LV, Lawson FC, Ping L, Wei X, Lewis EF, Maggioni AP, McMurray JJ, Probstfield JL, Riddle MC, Solomon SD, Tardif JC; ELIXA Investigators. Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome. N Engl J Med. 2015 Dec 3;373(23):2247-57. doi: 10.1056/NEJMoa1509225. Zaccardi F, Htike ZZ, Webb DR, Khunti K, Davies MJ. Benefits and Harms of Once-Weekly Glucagon-like Peptide-1 Receptor Agonist Treatments: A Systematic Review and Network Meta-analysis. Ann Intern Med. 2015 Dec 8:1-12. doi: 10.7326/M15-1432. [Epub ahead of print]
: doi: /NEJMoa Zaccardi F, Htike ZZ, Webb DR, Khunti K, Davies MJ. Benefits and Harms of Once-Weekly Glucagon-like Peptide-1 Receptor Agonist Treatments: A Systematic Review and Network Meta-analysis. Ann Intern Med Dec 8:1-12. doi: /M [Epub ahead of print].")
2
DPP4 阻害薬、 GLP-1 受容体作動薬、 SGLT2 阻害薬の心血管障害への影響 1.Scirica BM, Bhatt DL, Braunwald E, Steg PG, Davidson J, Hirshberg B, Ohman P, Frederich R, Wiviott SD, Hoffman EB, Cavender MA, Udell JA, Desai NR, Mosenzon O, McGuire DK, Ray KK, Leiter LA, Raz I; SAVOR- TIMI 53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med 2013;369:1317–1326. 2.White WB, Cannon CP, Heller SR, Nissen SE, Bergenstal RM, Bakris GL, Perez AT, Fleck PR, Mehta CR, Kupfer S, Wilson C, Cushman WC, Zannad F; EXAMINE Investigators. Alogliptin after acute coronary syndrome in patients with type 2 diabetes. N Engl J Med 2013;369:1327–1335. European Heart Journal doi:10.1093/eurheartj/ehv239 12

3
From the Cardiovascular Division, Brigham and Women’s Hospital, and Harvard Medical School — both in Boston (M.A.P., B.C., E.F.L., S.D.S.); Estudios Clínicos Latinoamérica, Rosario, Argentina (R.D.); University of Bergen, Stavanger University Hospital, Stavanger, Norway (K.D.); McMaster University, Hamilton, ON, Canada (H.C.G.); Rigshospitalet Copenhagen University Hospital, Copenhagen (L.V.K.); Sanofi U.S., Bridgewater, NJ (F.C.L., L.P., X.W.); Research Center of the Italian Association of Hospital Cardiologists, Florence (A.P.M.); British Heart Foundation Cardiovascular Research Centre, University of Glasgow, Glasgow, United Kingdom (J.J.V.M.); University of Washington Medical Center, Seattle (J.L.P.); Oregon Health and Science University, Portland (M.C.R.); and Montreal Heart Institute, Université de Montréal, Montreal (J.C.T.). N Engl J Med 2015;373:2247-57. DOI: 10.1056/NEJMoa1509225

4
Background Cardiovascular morbidity and mortality are higher among patients with type 2 diabetes, particularly those with concomitant cardiovascular diseases, than in most other populations. We assessed the effects of lixisenatide, a glucagon-like peptide 1– receptor agonist, on cardiovascular outcomes in patients with type 2 diabetes who had had a recent acute coronary event.

5
Methods We randomly assigned patients with type 2 diabetes who had had a myocardial infarction or who had been hospitalized for unstable angina within the previous 180 days to receive lixisenatide or placebo in addition to locally determined standards of care. The trial was designed with adequate statistical power to assess whether lixisenatide was noninferior as well as superior to placebo, as defined by an upper boundary of the 95% confidence interval for the hazard ratio of less than 1.3 and 1.0, respectively, for the primary composite end point of cardiovascular death, myocardial infarction, stroke, or hospitalization for unstable angina.

6
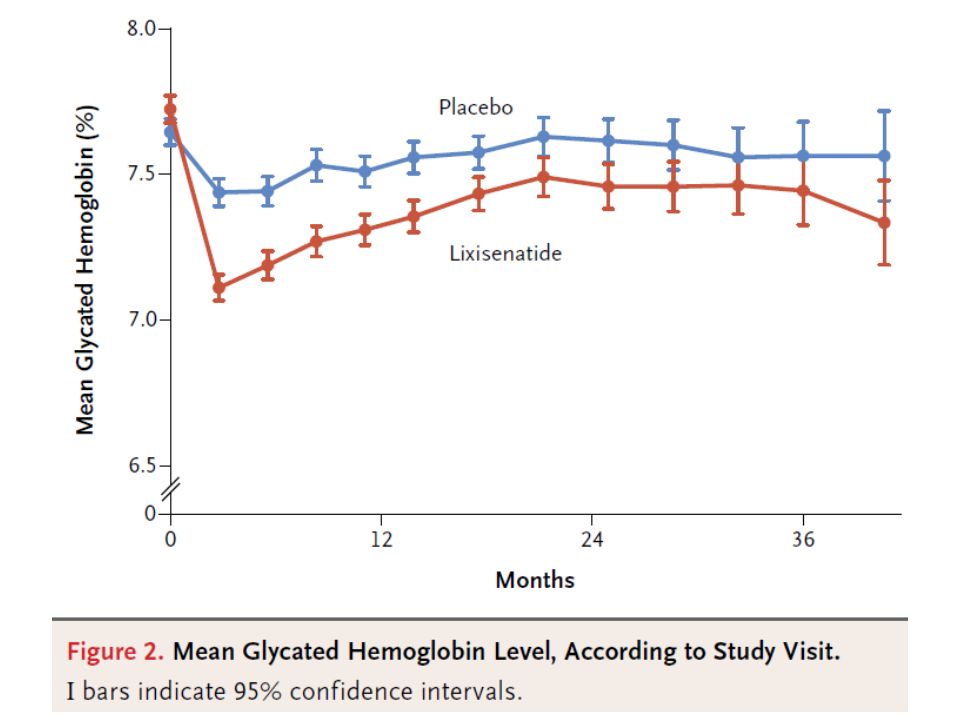
* Plus–minus values are means ±SD. There were no significant between-group differences at baseline, except with respect to age (P = 0.005), estimated glomerular filtration rate (eGFR; P = 0.006), glycated hemoglobin level (P = 0.02), and prior stroke (P = 0.01). To convert the values for cholesterol to millimoles per liter, multiply by 0.02586. ACS denotes acute coronary syndrome, HDL high-density lipoprotein, LDL low-density lipoprotein, NSTEMI non–ST-segment elevation myocardial infarction, and STEMI ST-segment elevation myocardial infarction. † The body-mass index is the weight in kilograms divided by the square of the height in meters. ‡ Race and ethnic group were self-reported. § Peripheral arterial disease included amputation due to a cause other than trauma.. Albumin was measured in milligrams and creatinine in grams. N Engl J Med 2015;373:2247-57.
, estimated glomerular filtration rate (eGFR; P = 0.006), glycated hemoglobin level (P = 0.02), and prior stroke (P = 0.01). To convert the values for cholesterol to millimoles per liter, multiply by ACS denotes acute coronary syndrome, HDL high-density lipoprotein, LDL low-density lipoprotein, NSTEMI non–ST-segment elevation myocardial infarction, and STEMI ST-segment elevation myocardial infarction. † The body-mass index is the weight in kilograms divided by the square of the height in meters. ‡ Race and ethnic group were self-reported. § Peripheral arterial disease included amputation due to a cause other than trauma.. Albumin was measured in milligrams and creatinine in grams. N Engl J Med 2015;373:")
10
* Events were assessed with the use of the classifications in the Medical Dictionary for Regulatory Activities (MedDRA), version 15.0. † Adjudicated cardiovascular events were not required to be submitted as serious adverse events unless they were considered by the investigator to be possibly drug-related. ‡ Investigations included abnormal results on laboratory tests or physical examination. The most common MedDRA preferred terms used were “alanine aminotransferase increased” (in seven patients in the placebo group and in two in the lixisenatide group) and “blood glucose increased” (in four in the placebo group and in one in the lixisenatide group). N Engl J Med 2015;373:2247-57.
 and blood glucose increased (in four in the placebo group and in one in the lixisenatide group). N Engl J Med 2015;373:")
11
Results The 6068 patients who underwent randomization were followed for a median of 25 months. A primary end-point event occurred in 406 patients (13.4%) in the lixisenatide group and in 399 (13.2%) in the placebo group (hazard ratio, 1.02; 95% confidence interval [CI], 0.89 to 1.17), which showed the noninferiority of lixisenatide to placebo (P<0.001) but did not show superiority (P=0.81). There were no significant between-group differences in the rate of hospitalization for heart failure (hazard ratio in the lixisenatide group, 0.96; 95% CI, 0.75 to 1.23) or the rate of death (hazard ratio, 0.94; 95% CI, 0.78 to 1.13). Lixisenatide was not associated with a higher rate of serious adverse events or severe hypoglycemia, pancreatitis, pancreatic neoplasms, or allergic reactions than was placebo.
 in the lixisenatide group and in 399 (13.2%) in the placebo group (hazard ratio, 1.02; 95% confidence interval [CI], 0.89 to 1.17), which showed the noninferiority of lixisenatide to placebo (P<0.001) but did not show superiority (P=0.81). There were no significant between-group differences in the rate of hospitalization for heart failure (hazard ratio in the lixisenatide group, 0.96; 95% CI, 0.75 to 1.23) or the rate of death (hazard ratio, 0.94; 95% CI, 0.78 to 1.13). Lixisenatide was not associated with a higher rate of serious adverse events or severe hypoglycemia, pancreatitis, pancreatic neoplasms, or allergic reactions than was placebo..")
12
Conclusions In patients with type 2 diabetes and a recent acute coronary syndrome, the addition of lixisenatide to usual care did not significantly alter the rate of major cardiovascular events or other serious adverse events. (Funded by Sanofi; ELIXA ClinicalTrials.gov number, NCT01147250.)
.")
13
Message 急性冠症候群( ACS )を最近発症した 2 型糖尿病 患者 6068 例を対象に、通常治療+リキシセナチ ド併用による心血管転帰を無作為化試験で検証 ( ELIXA 試験)。主要複合評価項目(心血管死、 心筋梗塞、脳卒中、不安定狭心症による入院)発 生率で、リキシセナチドはプラセボに対し非劣性 ではあったが( 13.4 %対 13.2 %、ハザード比 1.02 ; 95 % CI, 0.89 - 1.17 、 P < 0.001 )、 優越性は示されなかった( P = 0.81 )。 https://www.m3.com/clinical/journal/16068
を最近発症した 2 型糖尿病 患者 6068 例を対象に、通常治療+リキシセナチ ド併用による心血管転帰を無作為化試験で検証 ( ELIXA 試験)。主要複合評価項目(心血管死、 心筋梗塞、脳卒中、不安定狭心症による入院)発 生率で、リキシセナチドはプラセボに対し非劣性 ではあったが( 13.4 %対 13.2 %、ハザード比 1.02 ; 95 % CI, 、 P < )、 優越性は示されなかった( P = 0.81 )。")
15
alogliptin Dipeptidyl peptidase-4 阻害薬/ GLP-1 受容体作動薬 sitagliptin vildagliptin ExenatideLixisenatide linagliptin saxagliptinteneligliptin anagliptin trelagliptin LiraglutideDulaglutide omarigliptin Semaglutide 演者編集 taspoglutide albiglutide

16
Drs. Zaccardi, Htike, Webb, Khunti, and Davies: Diabetes Research Centre, Leicester General Hospital, Gwendolen Road, Leicester LE5 4PW, United Kingdom. Ann Intern Med. Published online 8 December 2015 doi:10.7326/M15-1432

17
Background: Once-weekly glucagon-like peptide-1 receptor agonists (GLP-1RAs) are new drugs for the treatment of type 2 diabetes. Purpose: To summarize evidence for the cardiometabolic efficacy and adverse effects of once-weekly GLP-1RAs in adults with type 2 diabetes.

18
Data Sources: Electronic databases (PubMed, Web of Science, Cochrane Central Register of Controlled Trials, U.S. Food and Drug Administration, European Medicines Agency, ClinicalTrials.gov) and congress abstracts from inception through 26 September 2015. Study Selection: Randomized, controlled trials (≥24 weeks of follow-up) studying albiglutide, dulaglutide, once-weekly exenatide, semaglutide, and taspoglutide and reporting a cardiometabolic (primary outcome, hemoglobin A1c [HbA1c]) or safety outcome. Data Extraction: Extraction was done in duplicate, and risk of bias was assessed. No language restriction was applied.
 and congress abstracts from inception through 26 September Study Selection: Randomized, controlled trials (≥24 weeks of follow-up) studying albiglutide, dulaglutide, once-weekly exenatide, semaglutide, and taspoglutide and reporting a cardiometabolic (primary outcome, hemoglobin A1c [HbA1c]) or safety outcome. Data Extraction: Extraction was done in duplicate, and risk of bias was assessed. No language restriction was applied..")
23
Nodes represent the treatments being compared; their size is proportional to the number of participants. Edges represent the available direct comparisons between pairs of treatments, and their width is proportional to the number of trials comparing every pair. ALB = albiglutide; BASAL = basal insulin; dGLP1 = daily glucagon-like peptide- 1 receptor agonists; DUL 0.75 = dulaglutide, 0.75 mg; DUL 1.5 = dulaglutide, 1.5 mg; EOW = exenatide once-weekly; GLIM = glimepiride; HbA1c = hemoglobin A1c; HDL = high-density lipoprotein; LDL = low-density lipoprotein; MET = metformin; PIO = pioglitazone; PLA = placebo; RAPID = rapid insulin; SITA = sitagliptin; TAS 10 = taspoglutide, 10 mg; TAS 20 = taspoglutide, 20 mg. Ann Intern Med. Published online 8 December 2015 doi:10.7326/M15-1432

24
Data are reported as mean differences (95% CIs) and indicate differences versus the reference drug (for example, compared with dulaglutide, 1.5 mg, albiglutide increases HbA1c by 0.40% [CI, 0.17% to 0.63%]). ALB = albiglutide; DUL 0.75 = dulaglutide, 0.75 mg; DUL 1.5 = dulaglutide, 1.5 mg; EOW = exenatide once-weekly; HbA1c = hemoglobin A1c; HDL = high- density lipoprotein; LDL = low- density lipoprotein; TAS 10 = taspoglutide, 10 mg; TAS 20 = taspoglutide, 20 mg. * To convert values to mg/dL, divide by 0.0555. † To convert values to mg/dL, divide by 0.0259. ‡ To convert values to mg/dL, divide by 0.0113.
![Data are reported as mean differences (95% CIs) and indicate differences versus the reference drug (for example, compared with dulaglutide, 1.5 mg, albiglutide increases HbA1c by 0.40% [CI, 0.17% to 0.63%]).](http://images.slideplayer.com/32/9906275/slides/slide_24.jpg "ALB = albiglutide; DUL 0.75 = dulaglutide, 0.75 mg; DUL 1.5 = dulaglutide, 1.5 mg; EOW = exenatide once-weekly; HbA1c = hemoglobin A1c; HDL = high- density lipoprotein; LDL = low- density lipoprotein; TAS 10 = taspoglutide, 10 mg; TAS 20 = taspoglutide, 20 mg. * To convert values to mg/dL, divide by † To convert values to mg/dL, divide by ‡ To convert values to mg/dL, divide by")
29
Zaccardi and colleagues (5) conducted a network meta-analysis of randomized trials that could yield, directly or indirectly, estimates of comparative efficacy between once-weekly glucagon-like peptide-1 receptor agonists. They found these trials to have inadequate blinding (which could affect co-interventions that may affect hemoglobin A 1c level and weight outcomes) and substantial loss to follow-up. The estimates for each direct, indirect, and network comparison and their quality ratings were not reported separately and hindered appraisal. Data on outcomes of importance to patients, including quality of life, treatment burden, and morbidity and mortality, were sparse or nonexistent. Network inspection shows that the 2 leading options, once-weekly exenatide and 1.5 mg-dulaglutide, were compared mostly to daily exenatide and 0.75 mg-dulaglutide (both products are from the same company). Because of the low reliability of the evidence summarized (7), claims of differences between agents should be met with skepticism, including rankings that suggest that, within the once-weekly preparations, exenatide and dulaglutide are associated with the biggest reduction in hemoglobin A 1c level and weight while being well-tolerated.57 Ann Intern Med. Published online 8 December 2015 doi:10.7326/M15-2610
 and substantial loss to follow-up. The estimates for each direct, indirect, and network comparison and their quality ratings were not reported separately and hindered appraisal. Data on outcomes of importance to patients, including quality of life, treatment burden, and morbidity and mortality, were sparse or nonexistent. Network inspection shows that the 2 leading options, once-weekly exenatide and 1.5 mg-dulaglutide, were compared mostly to daily exenatide and 0.75 mg-dulaglutide (both products are from the same company). Because of the low reliability of the evidence summarized (7), claims of differences between agents should be met with skepticism, including rankings that suggest that, within the once-weekly preparations, exenatide and dulaglutide are associated with the biggest reduction in hemoglobin A 1c level and weight while being well-tolerated.57 Ann Intern Med. Published online 8 December 2015 doi: /M")
30
Data Synthesis: 34 trials (21 126 participants) were included. Compared with placebo, all once-weekly GLP-1RAs reduced HbA1c and fasting plasma glucose; taspoglutide, 20 mg, once-weekly exenatide, and dulaglutide, 1.5 mg, reduced body weight. Among once-weekly GLP-1RAs, the greatest differences were found between dulaglutide, 1.5 mg, and taspoglutide, 10 mg, for HbA1c (-0.4% [95% CI, -0.7% to -0.2%]), once-weekly exenatide and albiglutide for fasting plasma glucose (-0.7 mmol/L [CI, -1.1 to -0.2 mmol/L]; -12.6 mg/dL [CI, -19.8 to -3.6 mg/dL]), and taspoglutide, 20 mg, and dulaglutide, 0.75 mg, for body weight (-1.5 kg [CI, -2.2 to -0.8]). Clinically marginal or no differences were found for blood pressure, blood lipid levels, and C-reactive protein levels. Once-weekly exenatide increased heart rate compared with albiglutide and dulaglutide (1.4 to 3.2 beats/min). Among once-weekly GLP-1RAs, the risk for hypoglycemia was similar, whereas taspoglutide, 20 mg, had the greatest risk for nausea (odds ratios, 1.9 to 5.9).
, once-weekly exenatide and albiglutide for fasting plasma glucose (-0.7 mmol/L [CI, -1.1 to -0.2 mmol/L]; mg/dL [CI, to -3.6 mg/dL]), and taspoglutide, 20 mg, and dulaglutide, 0.75 mg, for body weight (-1.5 kg [CI, -2.2 to -0.8]). Clinically marginal or no differences were found for blood pressure, blood lipid levels, and C-reactive protein levels. Once-weekly exenatide increased heart rate compared with albiglutide and dulaglutide (1.4 to 3.2 beats/min). Among once-weekly GLP-1RAs, the risk for hypoglycemia was similar, whereas taspoglutide, 20 mg, had the greatest risk for nausea (odds ratios, 1.9 to 5.9)..")
31
Limitation: Data were unavailable for semaglutide, definitions of outcomes were heterogeneous, the last-observation-carried-forward imputation method was used in 73% of trials, and publication bias is possible. Conclusion: Compared with other once-weekly GLP-1RAs, dulaglutide 1.5 mg, once-weekly exenatide, and taspoglutide, 20 mg, showed a greater reduction of HbA1c, fasting plasma glucose, and body weight. Taspoglutide, 20 mg, had the highest risk for nausea; risk for hypoglycemia among once-weekly GLP-1RAs was similar. Primary Funding Source: Sanofi Aventis (grant to the University of Leicester).
..")
32
スイス Roche 社、糖尿病治療薬候補品タスポ グルチドの権利を返還、子会社の中外製薬も 国内開発を中止に 2011 年 2 月 3 日 08:27 semaglutide dulaglutide once-weekly exenatide taspoglutide albiglutide 日本GSKがAlbiglutideを発売するかどうかは2015年7月現在未定である。なぜなら、GSKのMRリストラが急速な勢 いで進んでいるからである。2015年3月末現在の日本GSKのMR数は前年度から600人規模で減少。同社はノバル ティスとグローバルで事業スワップを実施しており、日本国内ではGSKのがん事業がノバルティスに譲渡された。こ れにより、同事業に携わるMRや研究開発部門といったメンバーのほとんどが、3月中にノバルティスファーマへ転籍 した模様だ。GSKは同時にグローバルでMRの個人売上目標をなくすといった営業刷新を行っており、日本でも今年 から実施している。併せて早期退職者を募集したとされている。しかしながら、移転先のノバルティスファーマも 500人以上削減したとみられている。この外資2社がMR削減の2強だ。このあおりを受け、Tanzeumの日本国内発 売も見通しが立たなくなっているのだ。 http://funabashi-tounyou.blogspot.jp/2014/06/gskglp-1-tanzeum-albiglutide.html April 15, 2014 albiglutide ( Tanzeum 、 GLP-1 受容体作動薬)が、米国食品医薬品局( FDA )により承認された。 FDA は、 albiglutide と甲状腺腫瘍の因果関係の可能性や、小児における有効性、および心血管系に対するリスクを評 価する承認後試験をいくつか行うよう求めている。 http://dm-rg.net/news/2014/04/014572.html
が、米国食品医薬品局( FDA )により承認された。 FDA は、 albiglutide と甲状腺腫瘍の因果関係の可能性や、小児における有効性、および心血管系に対するリスクを評 価する承認後試験をいくつか行うよう求めている。")
33
Message 2 型糖尿病患者への週 1 回投与のグルカゴン様ペプチド -1 受容体 作動薬( GLP-1RA ) 5 剤の効果と安全性を見た無作為化比較試験 34 件(対象計 2 万 1126 人)のシステマティックレビューとネッ トワークメタ解析で検証。 GLP1-RA は 5 剤すべてでプラセボに比 べ HbA1c と空腹時血糖を低下させていた。 Taspoglutide 20mg 、デュラグルチド 1.5mg 、週 1 回エキセナチドは他剤より 血糖改善効果が大きく、体重減少も認められた。ただし Taspoglutide 20mg は嘔気リスクが最も高く、低血糖リスクも 高かった。 https://www.m3.com/clinical/journal/16074 すでに taspoglutide, albiglutide は日本では製品化はないよう である。デバイスで週 1 回エキセナチドが負けている。そうなる と週一の GLP1-RA は Lilly のデュラグルチド ( トルリシティ / アテ オス ) が独り勝ちになりそう( 2015 年 7 月 3 日製造販売が承認)。 長期処方が可能になるのが今年の夏以降がどうなるのか?
 5 剤の効果と安全性を見た無作為化比較試験 34 件(対象計 2 万 1126 人)のシステマティックレビューとネッ トワークメタ解析で検証。 GLP1-RA は 5 剤すべてでプラセボに比 べ HbA1c と空腹時血糖を低下させていた。 Taspoglutide 20mg 、デュラグルチド 1.5mg 、週 1 回エキセナチドは他剤より 血糖改善効果が大きく、体重減少も認められた。ただし Taspoglutide 20mg は嘔気リスクが最も高く、低血糖リスクも 高かった。 すでに taspoglutide, albiglutide は日本では製品化はないよう である。デバイスで週 1 回エキセナチドが負けている。そうなる と週一の GLP1-RA は Lilly のデュラグルチド ( トルリシティ / アテ オス ) が独り勝ちになりそう( 2015 年 7 月 3 日製造販売が承認)。 長期処方が可能になるのが今年の夏以降がどうなるのか?")
Similar presentations












 ( 独 ) 農業・食品産業技術総合研究機 構 東北農業研究センター 菅野洋光.>")





行列式の定義には、数学的な概念がいろいろ必要である。まずそれらを順に見ていく。>")

 を、出現から消滅まで 全天 X 線監視装置 MAXI (マキシ)で観測したところ、 新種のブラックホール新星であることが判明した。 従来のブラックホールを、 多量のガスを一気に飲み込む「肉食系」と.>")




を体験したことにより興味を惹かれ るきっかけとなった。主な目的は、これ.>")



を生かした 確かな学力を形成する授業づく り ② 家庭との連携を図った家庭学習の習慣化.>")

