Download presentation
Presentation is loading. Please wait.

1
41° Convegno CARDIOLOGIA 2007 Milano, 17/21 Settembre 2007 LA GESTIONE DELLA FIBRILLAZIONE ATRIALE NEL PAZIENTE CON INSUFFICIENZA CARDIACA: QUANDO CONSERVATIVI, QUANDO AGGRESSIVI. G. Di Tano U.O. Cardiologia Az. Osped. Papardo, Messina INCONTRI CON GLI ESPERTI

2
Wang TJ et al. Circulation 2003;107:2920 Unadjusted cumulative incidence of first CHF in individuals with AF Unadjusted cumulative incidence of first AF in individuals with CHF

4
ATRIAL FIBRILLATION : PREVALENCE INCREASE WITH SEVERITY OF HEART FAILURE Camm AJ et al. Dialog Cardiovasc Med, 2003

6
Heart Failure Atrial Remodeling Atrial Fibrillation LA pressure Angiotensin II Aldosterone Atrial Fibrosis Stretch sympathetic tone Ectopic activity

7
Paroxysmal AF Persistent AF Permanent AF Triggers ectopic foci Electrophysiologic Remodeling Chronic Substrate fibrosis Stambler et al JCE 2003;14:499 Li, Nattel et al. Circulation. 1999;100:87-95 Types of AF

8
Heart Failure Atrial Remodeling Atrial Fibrillation LA pressure Angiotensin II Aldosterone Atrial Fibrosis Stretch sympathetic tone Ectopic activity Loss of atrial contraction Irregular R-R Intervals Rapid Rate

9
Rapid heart rates depress contractility: abnormal force - frequency in relationship in heart failure 0 100 200 2060120180 NonfailingFailing Heart Rate (beats / min) % change in Force Pieske Circ Res 1999; Gwathmey JCI 1990; Mulieri Circulation 1992; Heerdt PM, Circulation. 2000;102:2713-9.

10
Cardiomyopathy can be caused by any tachycardia (>110 bpm) that occurs as little as 10-15% of day Severity related to rate and duration of HR Maximal improvement after rate control may require upto 8 months After improvement susceptibility to rapid deterioration remains if tachycardia recurs Olshansky et al Circulation 2004 Fenelon et al PACE 1996; 19:95-106 Shinbane J et al. JACC 1997; 29: 709-715 Atrial Fibrillation and Tachycardia Induced Cardiomyopathy

11
APPROCCIO CONSERVATIVO... APPROCCIO AGGRESSIVO… GESTIONE Gestione della Fibrillazione Atriale nello Scompenso Cardiaco TERAPIA OTTIMIZZATA DELLO SCOMPENSO

12
Prevention of Atrial Fib With Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers: A Meta-Analysis Healey, et al JACC 2005;45:1832 11 studies with 56,308 patients Overall, ACEIs and ARBs reduced the relative risk of AF by 28% Benefit is similar for ACE-inhibitors and AII blockers Reduction in AF was greatest in patients with heart failure (relative risk reduction 44%, p = 0.007). There appears to be a large effect after cardioversion (48% RRR), but the confidence limits are wide (95% CI 21% to 65%)
, but the confidence limits are wide (95% CI 21% to 65%).")
13
Atrial Fibrillation in Patients with Heart Failure: Management Rate control Anticoagulation Rhythm control = restore sinus rhythm or Rate control = remain in fibrillation

14
Atrial Fibrillation: Rate Control digoxin – poor efficacy but well tolerated beta - adrenergic blockers calcium channel blockers – effective but negative inotropic effects –verapamil, diltiazem amiodarone – effective but potential major toxicity

16
{

17
Atrial Fibrillation + Heart Failure Rate Control Rhythm Control (restore and maintain sinus rhythm) ? Avoidance antiarrhythmic drugs… Reduced need for repeated CVE Improved cardiac function and symptoms Improved QL Prevention TE

18
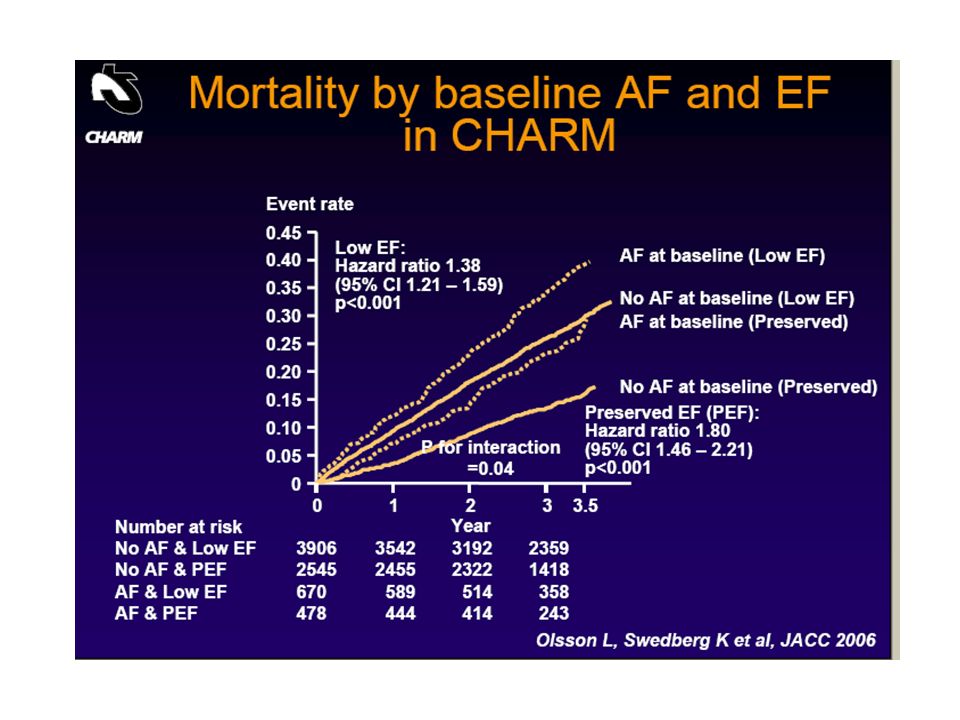
Atrial Fibrillation in Heart Failure Patients with AF have increased mortality compared to SR patients Patients who convert to SR have lower mortality than those who remain in AF Should patients with heart failure and AF be converted and maintained in sinus rhythm? Wang Circ 2003;107:2920; Middlekauff Circ 1991; 84: 40 Dries JACC. 1998; 32: 695; Deedwania Circ 1998; 98: 2574; Pozzoli JACC 1998; 32: 197; Torp-Pedersen NEJM 1999; 341: 857

19
Rate Control Rhythm Control If you were born in sinus rhythm, you should probably try to remain so. AFFIRM PIAF RACE STAF

20
AFFIRM A Comparison of Rate Control and Rhythm Control in Patients with Atrial Fibrillation NEJM 347:1825, 2002 4060 patients (age 70 yrs) Mortality at 5 yrs (p = 0.06): rhythm control 23.8% vs 21.3% rate control Rhythm control (RS only in 63%) increased hospitalizations increased exposure to drug adverse effects did not reduce strokes did not improve functional capacity or quality of life Most strokes occurred after warfarin had been stopped or was subtherapeutic
 Mortality at 5 yrs (p = 0.06): rhythm control 23.8% vs 21.3% rate control Rhythm control (RS only in 63%) increased hospitalizations increased exposure to drug adverse effects did not reduce strokes did not improve functional capacity or quality of life Most strokes occurred after warfarin had been stopped or was subtherapeutic")
21
AFFIRM was not a Heart Failure Trial Prior CHF: 23.1% Mean EF: 55% Normal LV ejection fraction in 74% - Presence of RS carried a small, but statically significant, improvement in NYHA functional class at follow-up. Chung MK et al, J Am Coll Cardiol 2005;46:1891 - 939 HF pts: no benefit of a strategy of rhythm control.

22
Is rhythm control superior to rate control in patients with atrial fibrillation and congestive heart failure? Al-Khatib SM et al., Am J Cardiol 2004;94:797 In 1,009 patients with AF and congestive heart failure, the 1-year mortality rate was identical (both 21%) and at 2-year mortality rate was 31% in patients treated with rate control (n = 505) versus 29% in patients treated with rhythm control (n = 504). After adjusting for differences in baseline characteristics and medications, no significant difference in mortality was found between the 2 groups (p=.79)
 and at 2-year mortality rate was 31% in patients treated with rate control (n = 505) versus 29% in patients treated with rhythm control (n = 504). After adjusting for differences in baseline characteristics and medications, no significant difference in mortality was found between the 2 groups (p=.79).")
23
Am Heart J 2005:149;1106

24
Motivi della mancata efficacia della strategia Rhythm control Effetto deleterio degli antiarimici (minor efficacia, azione proaritmica - aritmie ventricolari, aumentato FCV durante AF, bradiaritmie -, inotropi negativi, tossicità) Interazioni farmacologiche Conversione di episodi di FA sintomatici in episodi silenti … Sospensione anticipata TAO Class I antiarrhythmic drugs increase mortality in patients with heart failure and AF - (post-hoc analysis) SPAF, JACC 1992
 Interazioni farmacologiche Conversione di episodi di FA sintomatici in episodi silenti … Sospensione anticipata TAO Class I antiarrhythmic drugs increase mortality in patients with heart failure and AF - (post-hoc analysis) SPAF, JACC 1992")
25
Rate Control vs Rhythm Control Favor rate control Asymptomatic, old, pts in atrial fibrillation Contraindication to amiodarone Favor attempts to maintain sinus rhythm First or infrequent episodes of persistent AF Significant symptoms in AF Difficult rate control Contraindication to long term warfarin

29
Class I anti-arrhythmic drugs should be avoided as they may provoke fatal ventricular arrhythmias, have an adverse hemodynamic effect and reduce survival in heart failure Level of evidence B, class III

33
Background Amiodarone is effective in maintaining sinus rhythm in atrial fibrillation but is associated with potentially serious toxic effects. Dronedarone is a new antiarrhythmic agent pharmacologically related to amiodarone but developed to reduce the risk of side effects. Methods In two identical multicenter, double-blind, randomized trials, one conducted in Europe and one conducted in the United States, Canada, Australia, South Africa, and Argentina, we evaluated the efficacy of dronedarone, with 828 patients receiving 400 mg of the drug twice daily and 409 patients receiving placebo. Rhythm was monitored transtelephonically on days 2, 3, and 5; at 3, 5, 7, and 10 months; during recurrence of arrhythmia; and at nine scheduled visits during a 12-month period. The primary end point was the time to the first recurrence of atrial fibrillation or flutter. Results In the European trial, the median times to the recurrence of arrhythmia were 41 days in the placebo group and 96 days in the dronedarone group (P=0.01). The corresponding durations in the non-European trial were 59 and 158 days (P=0.002). At the recurrence of arrhythmia in the European trial, the mean (±SD) ventricular rate was 117.5±29.1 beats per minute in the placebo group and 102.3±24.7 beats per minute in the dronedarone group (P<0.001); the corresponding rates in the non-European trial were 116.6±31.9 and 104.6±27.1 beats per minute (P<0.001). Rates of pulmonary toxic effects and of thyroid and liver dysfunction were not significantly increased in the dronedarone group. Conclusions Dronedarone was significantly more effective than placebo in maintaining sinus rhythm and in reducing the ventricular rate during recurrence of arrhythmia. 18% dei pz era in classe NYHA I - II III - IV classe esclusi ANDROMEDA: Trial in pz con SC interrotto per > rischio di mortalità nei trattati
. The corresponding durations in the non-European trial were 59 and 158 days (P=0.002). At the recurrence of arrhythmia in the European trial, the mean (±SD) ventricular rate was 117.5±29.1 beats per minute in the placebo group and 102.3±24.7 beats per minute in the dronedarone group (P<0.001); the corresponding rates in the non-European trial were 116.6±31.9 and 104.6±27.1 beats per minute (P<0.001). Rates of pulmonary toxic effects and of thyroid and liver dysfunction were not significantly increased in the dronedarone group. Conclusions Dronedarone was significantly more effective than placebo in maintaining sinus rhythm and in reducing the ventricular rate during recurrence of arrhythmia. 18% dei pz era in classe NYHA I - II III - IV classe esclusi ANDROMEDA: Trial in pz con SC interrotto per > rischio di mortalità nei trattati.")
34
SHOCK BIFASICO (energie minori; a 150 J successo >90%) OTTIMIZZAZIONE DELLA CARDIOVERSIONE ELETTRICA ESTERNA PLACCHE ANTERO-POSTERIORE AMIODARONE 400 mg/die, 1 mese prima e 1-2 mesi dopo CVE: aumenta percentuale di RS e recidive FA a 1m CONTROINDICAZIONI: No TAO Temporanee: Trombosi atriale Terapia digitalica Ipertiroidismo…
 OTTIMIZZAZIONE DELLA CARDIOVERSIONE ELETTRICA ESTERNA PLACCHE ANTERO-POSTERIORE AMIODARONE 400 mg/die, 1 mese prima e 1-2 mesi dopo CVE: aumenta percentuale di RS e recidive FA a 1m CONTROINDICAZIONI: No TAO Temporanee: Trombosi atriale Terapia digitalica Ipertiroidismo…")
35
IPERTIROIDISMO SUB-CLINICO E FIBRILLAZIONE ATRIALE Bassa concentrazione di TSH (-soppresso-, < 0.01 µIU/ml) con normali livelli di FT 3 e FT 4, in pazienti asintomatici. Prevalenza dell11.8% tra gli anziani (0.5% - 3.9% negli adulti) Framingham (< 65 a): a 10 anni: - FA nel 28% in pz con SCHyp 11% nei normali Sawin CT, Thyroid 2002
 Framingham (< 65 a): a 10 anni: - FA nel 28% in pz con SCHyp 11% nei normali Sawin CT, Thyroid")
37
Cosa mi aspetta al rientro… Uomo, 57 anni, professionista, senza FR, CMD primitiva 01/04: insorgenza SC con FA ad elevata FCVm, BBSn, NYHA III; ECO: FE 25%, ipoc glob; DTD 62mm; IM ++, IT+++, dilatazione biatriale. Terapia: diuretici, ace-i; digitale; TAO. Migliorato, - 8 Kg, BNP in calo 03/04: Ricovero: coronarie normali, biopsia (neg); ECO: FE 30%, IM +; I T++, RS dopo CVE; profilassi con amiodarone ; inizia carvedilolo. - Ipotensione sintomatica: sospende ace-i; passa a bisoprololo - Progressiva stabilità. BNP 230 07/04: Ipertiroidismo iatrogeno. Sospende amiodarone. Resta in TAO - ECO: FE 35%, DTD: 58mm; AS: 19cm2. 02/05: Stabile; NYHA 1-2; Ormoni tiroidei normali; ECO: FE 35-40%, TAO
; ECO: FE 30%, IM +; I T++, RS dopo CVE; profilassi con amiodarone ; inizia carvedilolo. - Ipotensione sintomatica: sospende ace-i; passa a bisoprololo - Progressiva stabilità. BNP /04: Ipertiroidismo iatrogeno. Sospende amiodarone. Resta in TAO - ECO: FE 35%, DTD: 58mm; AS: 19cm2. 02/05: Stabile; NYHA 1-2; Ormoni tiroidei normali; ECO: FE 35-40%, TAO.")
38
12/06: Recidiva FA. (cardiopalmo, dispnea lieve…), BNP 373 01/07: CVE efficace (shock bifasico, 75J): RS. Terapia confernata… 06/07: Stabile; ECO: FE 38%,DTD 54mm, AS:42mm, AD:23cm2, IM+, IT+; BNP 250. 07/07: Riscontro occasionale di recidiva FA (60 b/m); asintomatico, BNP = 08/07: Persiste FA (FVm: 58b/m); asintomatico; non dispnea da sforzo. 09/07: Astenia, dispnea da sforzo…. Cosa fare ?
, BNP /07: CVE efficace (shock bifasico, 75J): RS. Terapia confernata… 06/07: Stabile; ECO: FE 38%,DTD 54mm, AS:42mm, AD:23cm2, IM+, IT+; BNP /07: Riscontro occasionale di recidiva FA (60 b/m); asintomatico, BNP = 08/07: Persiste FA (FVm: 58b/m); asintomatico; non dispnea da sforzo. 09/07: Astenia, dispnea da sforzo…. Cosa fare .")
Similar presentations





















 patients Policy.>")







 Trial>")