Download presentation
Presentation is loading. Please wait.

1
Spine Injuries

2
PATHOPHYSIOLOGY OF SPINE INJURIES
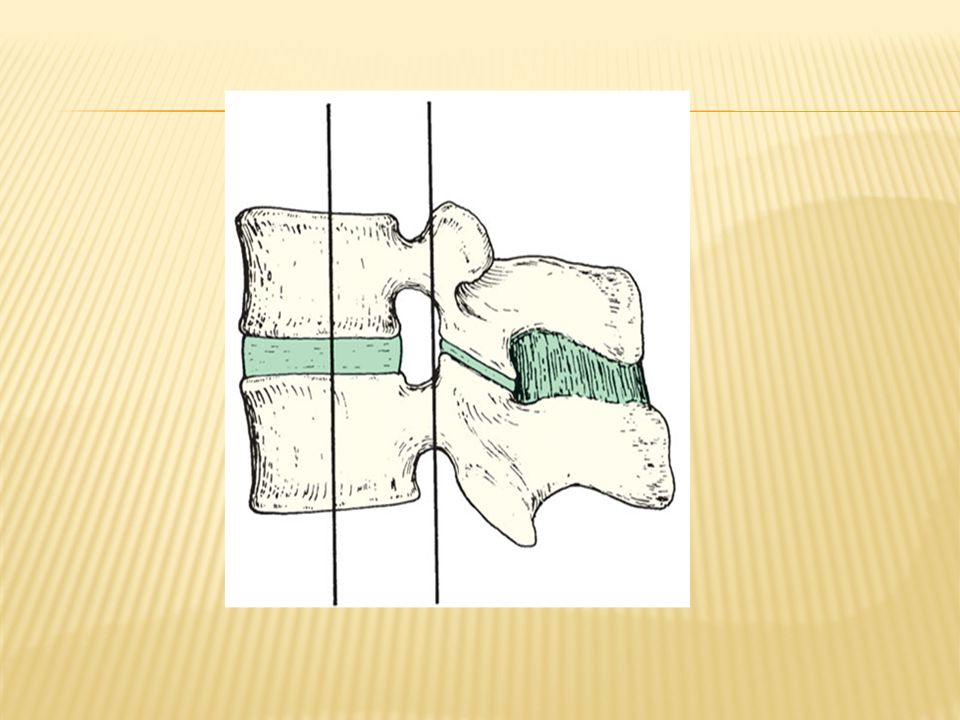
Stable and unstable injuries Spinal injuries carry a double threat: damage to the vertebral column and damage to the neural tissues. A stable injury is one in which the vertebral components will not be displaced by normal movements; there is little risk of them becoming damaged. An unstable injury is one in which there is a significant risk of displacement and consequent damage – or further damage – to the neural tissues.

4
Pathophysiology Primary changes Physical injury may be limited to the vertebral column, including its soft-tissue components, and varies from ligamentous strains to vertebral fractures and fracture-dislocations. The spinal cord and/or nerve roots may be injured, either by the initial trauma or by ongoing structural instability of a vertebral segment, Secondary changes During the hours and days following a spinal injury biochemical changes may lead to more gradual cellular disruption and extension of the initial neurological damage.

5
Mechanism of injury There are three basic mechanisms of injury: traction(avulsion), direct injury and indirect injury. Indirect injury This is the most common cause of significant spinal damage; PRINCIPLES OF DIAGNOSIS AND INITIAL MANAGEMENT Early management The adherence to the resuscitation protocol (airway with cervical spine control, breathing, circulation and haemorrhage control) supersedes the assessment of the spinal injury.
 supersedes the assessment of the spinal injury.")
6
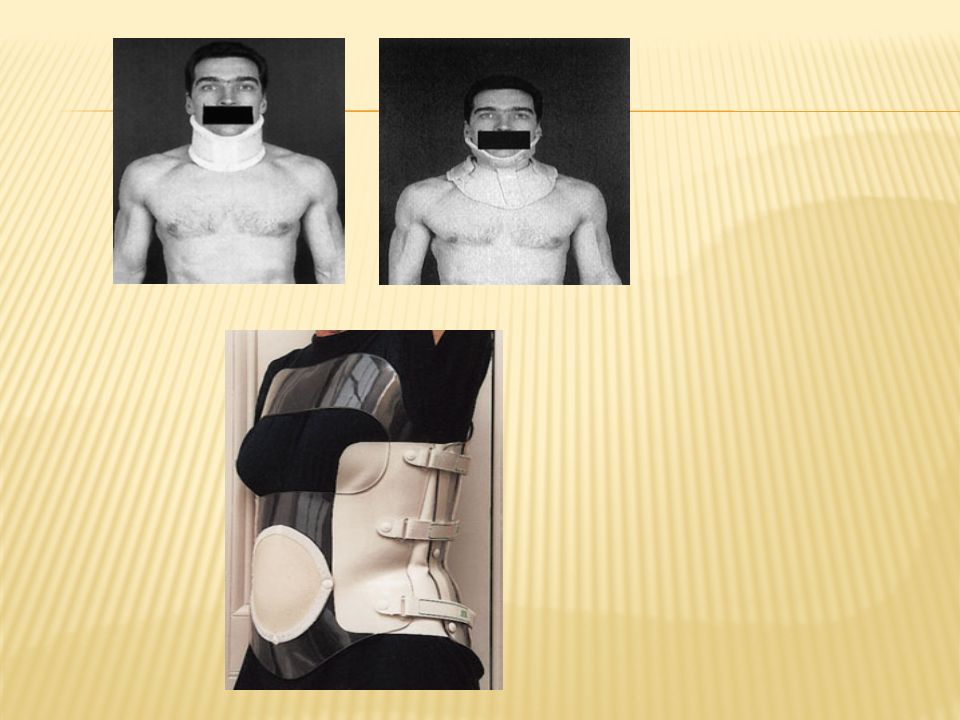
Methods of temporary immobilization
CERVICAL SPINE In-line immobilization The head and neck are supported in neutral position. QUADRUPLE IMMOBILIZATION A backboard, sandbags, a forehead tape and a semi rigid collars are applied. Thoracolumbar spine The patient should be moved without flexion or rotation of the thoracolumbar spine. A scoop stretcher and spinal board are very useful;

7
GENERAL EXAMINATION – ‘SHOCK’
DIAGNOSIS History A high index of suspicion is essential; symptoms and signs may be minimal; the history is crucial. Examination NECK BACK The patient is ‘log-rolled’ (i.e. turned over ‘in one piece’) to avoid movement of the vertebral column. GENERAL EXAMINATION – ‘SHOCK’ The ABC sequence of advanced trauma life support (ATLS) always takes precedence. Three types of shock may be encountered in patients with spinal injury: Hypovolaemic , neurogenic and spinal shock
 to avoid movement of the vertebral column. GENERAL EXAMINATION – ‘SHOCK’ The ABC sequence of advanced trauma life support (ATLS) always takes precedence. Three types of shock may be encountered in patients with spinal injury: Hypovolaemic , neurogenic and spinal shock.")
8
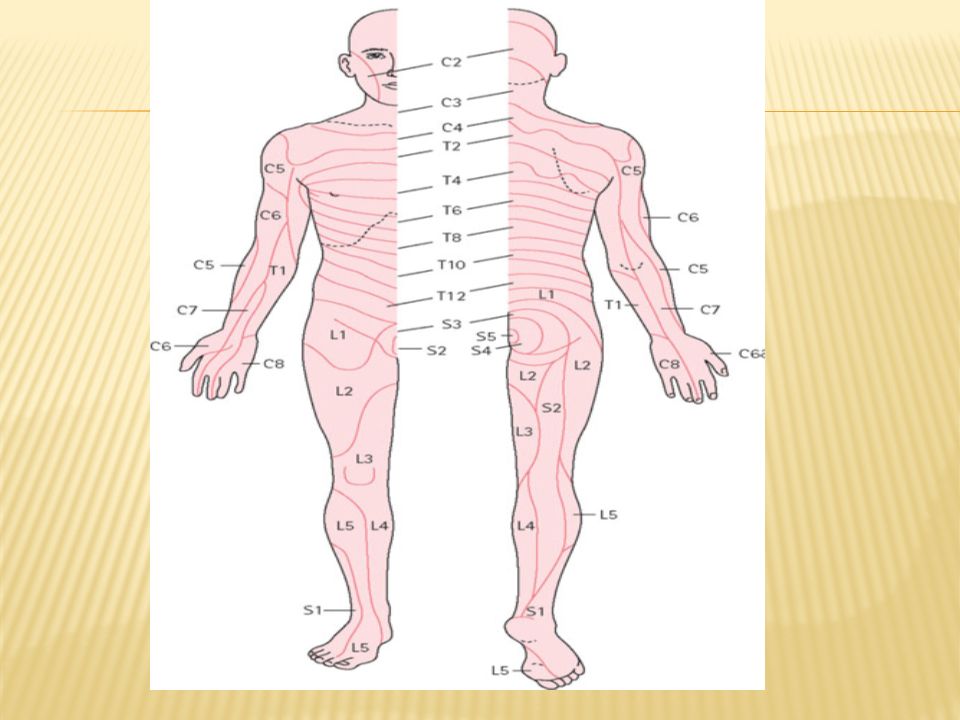
NEUROLOGICAL EXAMINATION
A full neurological examination is carried out in every case; this may have to be repeated several times during the first few days. Each dermatome, myotome and reflex is tested. The unconscious patient is difficult to examine; a spinal injury must be assumed until proven otherwise. Clues to the existence of a spinal cord lesion are a history of a fall or rapid deceleration, a head injury, diaphragmatic breathing, a flaccid anal sphincter, hypotension with bradycardia and a pain response above, but not below, the clavicle.

10
IMAGING • X-ray examination of the spine is mandatory for all accident victims complaining of pain or stiffness in the neck or back or peripheral paraesthesiae, X-ray examination should be carried out with a minimum of movement and manipulation In addition to anteroposterior and lateral views, open-mouth views are needed for the upper two cervical spines • CT is ideal for showing structural damage to individual vertebrae and displacement of bone fragments • MRI is the method of choice for displaying the intervertebral discs, ligamentum flavum and neural structures those who are considered for surgery. • Remember that the spine may be damaged in more than one place.

11
PRINCIPLES OF DEFINITIVE
TREATMENT The objectives of treatment are: • to preserve neurological function; • to minimize a perceived threat of neurological compression; • to stabilize the spine; • to rehabilitate the patient. The indications for urgent surgical stabilization are: (a) an unstable fracture with progressive neurological deficit and MRI signs of likely further neurological deterioration; and (b) controversially an unstable fracture in a patient with multiple injuries.
 an unstable fracture with progressive neurological deficit and MRI signs of likely further neurological deterioration; and. (b) controversially an unstable fracture in a patient with multiple injuries.")
12
Patients with no neurological injury
Stable injuries If the spinal injury is stable, the patient is treated by supporting the spine in a position that will cause no further strain; a firm collar or lumbar brace will usually suffice, but the patient may need to rest in bed until pain and muscle spasm subside. Unstable injuries If the spinal injury is unstable it should be held secure until the tissues heal and the spine becomes stable.

13
Patients with a neurological injury
If the spinal injury is stable (which is rare), the patient can be treated conservatively and rehabilitated With the usual unstable injury, conservative treatment can be still be used; this is highly demanding and is best carried out in a special unit Early operative stabilization is preferred by many; it facilitates nursing by inexperienced carers and reduces the risk of spinal deformity. Surgery is indicated: To facilitate and make nursing easy progressive neurological deterioration with evidence (or a serious risk) of further neural compression on MRI. Patients with incomplete lesions are also sometimes considered for operation.
, the patient can be treated conservatively and rehabilitated. With the usual unstable injury, conservative treatment can be still be used; this is highly demanding and is best carried out in a special unit Early operative stabilization is preferred by many; it facilitates nursing by inexperienced carers and reduces the risk of spinal deformity. Surgery is indicated: To facilitate and make nursing easy. progressive neurological deterioration with evidence (or a serious risk) of further neural compression on MRI. Patients with incomplete lesions are also sometimes considered for operation.")
14
Thoracolumbar spine TREATMENT METHODS Cervical spine
Collars Soft collars Tongs Halo ring At least four pins are inserted into the outer table of the skull and a ring is applied. Fixation Various operative procedures are available, depending on the level and pattern of injury. Thoracolumbar spine Beds Special beds are used in the management of spinal injuries. They are designed to avoid pressure sores. Brace Decompression and stabilization The aim of surgery is to reduce the fracture, hold the reduction and decompress the neural elements. The surgical approach can be either anterior or posterior.

16
CERVICAL SPINE INJURIES
The patient will usually give a history of a fall from a height, a diving accident or a vehicle accident in which the neck is forcibly moved. In a patient unconscious from a head injury, a fractured cervical spine should be assumed (and acted upon) until proved otherwise. Imaging Plain x-rays must be of high quality and should be inspected methodically. • In the anteroposterior view the lateral outlines should be intact, and the spinous processes andAn open-mouth view is necessary to show C1 and C2 tracheal shadow in the midline. andAn open-mouth view is necessary to show C1 and C2 tracheal shadow in the midline.
 until proved otherwise. Imaging. Plain x-rays must be of high quality and should be inspected methodically. • In the anteroposterior view the lateral outlines should be intact, and the spinous processes andAn open-mouth view is necessary to show C1 and C2 tracheal shadow in the midline. andAn open-mouth view is necessary to show C1 and C2 tracheal shadow in the midline.")
17
In the lateral view the smooth lordotic curve should be followed

18
If the cervico-thoracic junction cannot be seen, lateral view should be shoulders are pulled down.
The distance between the odontoid peg and the back of the anterior 3 mm in adults and 4.5 mm in children. • Examine the soft-tissue shadows. The retropharyngeal space may contain a haematoma; the prevertebral soft-tissue shadow should be less than 5 mm in thickness above the level of the trachea and less than one vertebral body’s width in thickness below.

19
CT scan is particularly helpful in defining the fracture.
C1 ring fracture Sudden severe load on the top of the head may cause a ‘bursting’ force which fractures the ring of the atlas(Jefferson’s fracture). the open-mouth view CT scan is particularly helpful in defining the fracture. If it is undisplaced, the injuryis stable and the patient wears a semi-rigid collar or halo-vest until the fracture unites more than 7 mm on the open-mouth view), the transverse ligament has ruptured; this injury is unstable and should be treated by a halo-vest for several weeks. If there is persisting instability on x-ray, a posterior C1/2 fixation and fusion is needed.
. the open-mouth view. CT scan is particularly helpful in defining the fracture. If it is undisplaced, the injuryis stable and the patient wears a semi-rigid collar or halo-vest until the fracture unites. more than 7 mm on. the open-mouth view), the transverse ligament has ruptured; this injury is unstable and should be treated by a halo-vest for several weeks. If there is persisting instability on x-ray, a posterior C1/2 fixation and fusion is needed.")
20
C2 Odontoid process fracture
Odontoid fractures are uncommon. They usually occur as flexion injuries in young adults after high velocity accidents or severe falls. However, they also occur in elderly, osteoporotic people as a result of low-energy trauma in which the neck is forced into hyperextension, e.g. a fall onto the face or forehead. Classification Odontoid fractures have been classified by Anderson and D’Alonzo (1974) as follows:
 as follows:")
21
Clinical features The history is usually that of a severe neck strain followed by pain and stiffness due to muscle spasm. The diagnosis is confirmed by high quality x-ray examination Neurological symptoms occur in a significant number of cases. Imaging Plain x-rays usually show the fracture, although the extent of the injury is not always obvious – e.g. there may be an associated fracture of the atlas or displacement at the occipito-atlanto level. Tomography is helpful but MRI has the advantage that it may reveal rupture of the transverse ligament; this can cause instability in the absence of a fracture.

22
Treatment Type I fractures Isolated fractures of the odontoid tip are uncommon. They need no more than immobilization in a rigid collar until discomfort subsides. Type II fractures These are often unstable and prone to non-union, especially if displaced more than 5 mm. Undisplaced fractures can be held by fitting a halo-vest or – in elderly patients – a rigid collar. Displaced fractures should be reduced by traction and can then be held by operative posterior C1/2 fusion; a drawback is that neck rotation will be restricted. Type III fractures If undisplaced, these are treated in a halo-vest for 8–12 weeks. If displaced, attempts should be made at reducing the fracture by halo traction,then 12 weeks immobilization by halo_vest.

23
Fracture-dislocations
Bilateral facet joint dislocations are caused by severe flexion or flexion–rotation injuries. One or both of the articular masses may be fractured or there may be a pure dislocation – ‘jumped facets’. The posterior ligaments are ruptured and the spine is unstable; often there is cord damage. Management The lateral x-ray shows forward displacement of a vertebra on the one below of greater than half the vertebra’s antero-posterior width.

24
treatment Skull traction is used, starting with 5 kg and increasing it step-wise by similar amounts up to about30kg; intravenous muscle relaxants and a bolster beneath the shoulders may help. X_ray follow up , M.R.I IS IMPORTANT TOO.

25
THORACOLUMBAR INJURIES
Most injuries of the thoracolumbar spine occur in the transitional area – T11 to L2 – between the somewhat rigid upper and middle thoracic column and the flexible lumbar spine.

26
The common mechanisms of injury are:
• Flexion–compression – failure of the anterior column and wedge-compression of the vertebral body. Usually stable, • Lateral compression – lateral wedging of the vertebral body resulting in a localized ‘scoliotic’ deformity. Axial compression – failure of anterior and middle columns causing a ‘burst’ fracture • Flexion–rotation – failure of all three columns and a risk of displacement or dislocation. Usually unstable. Flexion–distraction – the so-called ‘jack-knife’ injury causing failure of the posterior and middle columns and sometimes also anterior compression. Extension – tensile failure of the anterior column and compression failure of the posterior column. Unstable.

27
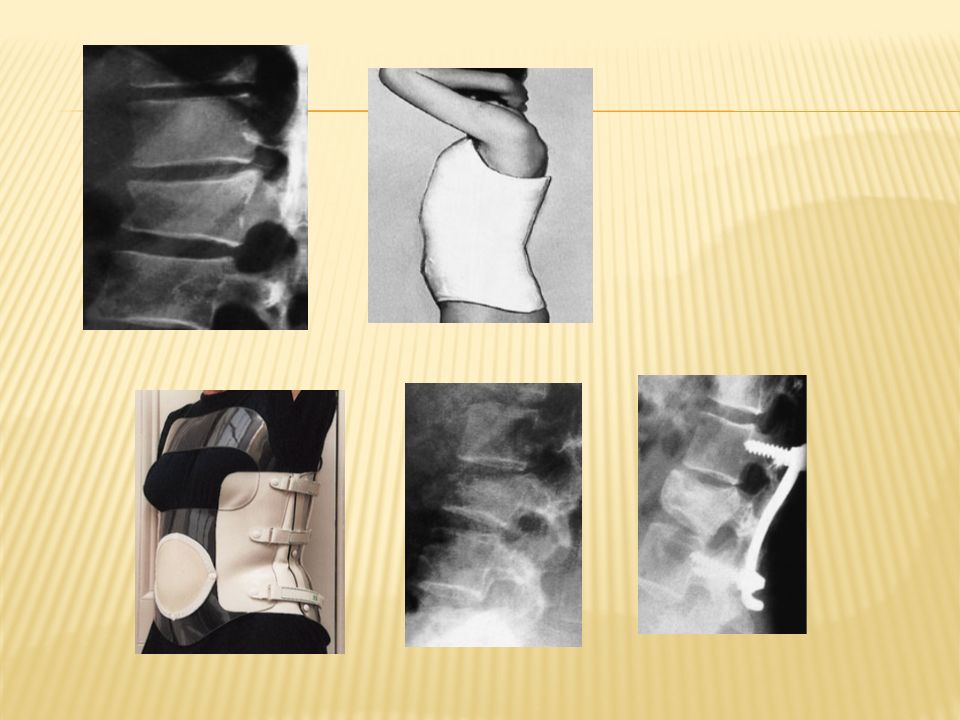
Flexion–compression injury
MAJOR INJURIES Flexion–compression injury This is by far the most common vertebral fracture and is due to severe spinal flexion, though in osteoporotic individuals fracture may occur with minimal trauma. Neurological injury is extremely rare. Management Patients with minimal wedging and a stable fracture 1w rest moderate wedging (loss of 20–40 per cent brace If loss of anterior vertebral height is greater than 40 per cent,

29
Axial compression or burst injury
Severe axial compression may ‘explode’ the vertebral body, causing failure of both the anterior and the middle columns. The posterior column is usually, but not always, undamaged. The posterior part of the vertebral body is shattered and fragments of bone and disc may be displaced into the spinal canal. The injury is usually unstable.

30
Treatment If there is minimal anterior wedging brace rest12 weeks. Any neurological symptoms such as tingling, weakness or alteration of bladder or bowel function must be reported immediately and should call for further imaging by MRI; anterior decompression and stabilization may then be needed if there are signs of present or impending

31
Jack-knife injury Combined flexion and posterior distraction may cause the mid-lumbar spine to jack-knife around an axis that is placed anterior to the vertebral column.

Similar presentations