Download presentation
Presentation is loading. Please wait.

1
Mike Gibson Glasgow Post Orthopaedic Training Program February 2011 Thoraco-Lumbar Fractures

2
Immediate Care and Assessment Investigation Classification Non Operative Treatment Surgical Treatment Cases

3
IMMEDIATE CARE ATLS Protocol –lateral XR’s thoracic and lumbar spine Spinal board Log rolling –enough people (5) High Index of Suspicion
 High Index of Suspicion")
4
Assessment of Spinal Fracture History Examination Imaging X Rays CT MRI

5
Examination Vertebral assessment – Log Roll –Inspection of spine Bruising, deformity –Palpation Localised tenderness, step-off, anal tone & sensation

6
Examination Neurological Assessment –Motor - voluntary contraction of muscles, graded In unconscious involuntary movement to pain Compare both sides of body –Sensation – soft touch in dermatomes –Autonomic function – bladder/bowel control, priapism

7
Clinical Features of Spinal Cord Injury Neurogenic Shock –Disruption of descending sympathetic pathways –Bradycardia, loss of smooth muscle tone →hypotension (fluid overload : inotropes) Spinal Shock –Loss of all cord function after injury causing flaccidity & loss of reflexes Abnormal Breathing –Lower Cx/upper thorx cause abd breathing & use of intercostals
 Spinal Shock –Loss of all cord function after injury causing flaccidity & loss of reflexes Abnormal Breathing –Lower Cx/upper thorx cause abd breathing & use of intercostals")
8
Trunk Control Patient will comfortably roll themselves around the bed Useful sign of Stability ? Not early post injury Not in Intoxicated Not in Head injured or confused

9
Investigation of Spinal Trauma Plain X Rays, CT to Characterise the Fracture MRI if Neurological Deficit Standing X rays

10
Definition of Instability When subjected to normal physiological forces the fracture will not displace sufficiently to produce neurological deficit or a significant deformity. DEFINITION OF INSTABILITY

12
CLASSIFICATION SYSTEMS Convey information Produce treatment plan Monitor patient progress Research tool

13
CLASSIFICATION SYSTEMS Spinal Column Injury Spinal Cord Injury

14
2 Column Classifications Holdsworth AO

15
3 Column Classification Denis Anterior - Ant 1/3 of disc /VB + ALL Middle - Post 1/3 of disc/VB + PLL Posterior - Post Elements

16
Spinal Cord Injury Accurately Document Neurological Status Remember SPINAL SHOCK Prognosis of deficit at 48hours

17
Spinal Cord Injury FRANKEL ANo motorNo sensation BNo motorMin. sensation CMotor(2-3)Sensation DMotor(4-5)Sensation ENormalNormal
Sensation DMotor(4-5)Sensation ENormalNormal.")
19
Spinal Cord Injury A.S.I.A. AComplete - no motor or sensation BIncomplete - sensation, no motor CIncomplete - sensation, motor<3 DIncomplete - sensation, motor 3 ENormal

20
Spinal Cord Injury Clinical Syndromes: Central Cord Anterior Posterior Brown-Sequard Conus/Cauda Equina

21
Spinal Cord Injury- Power MRC Grade 0 1 2 3 4 5 none visible contraction contracts, not against gravity contracts against gravity not resistance contracts against resistance normal

22
CONCLUSIONS Core knowledge allows transfer of accurate information Monitor patients neurological status Remember SPINAL SHOCK Research tool

23
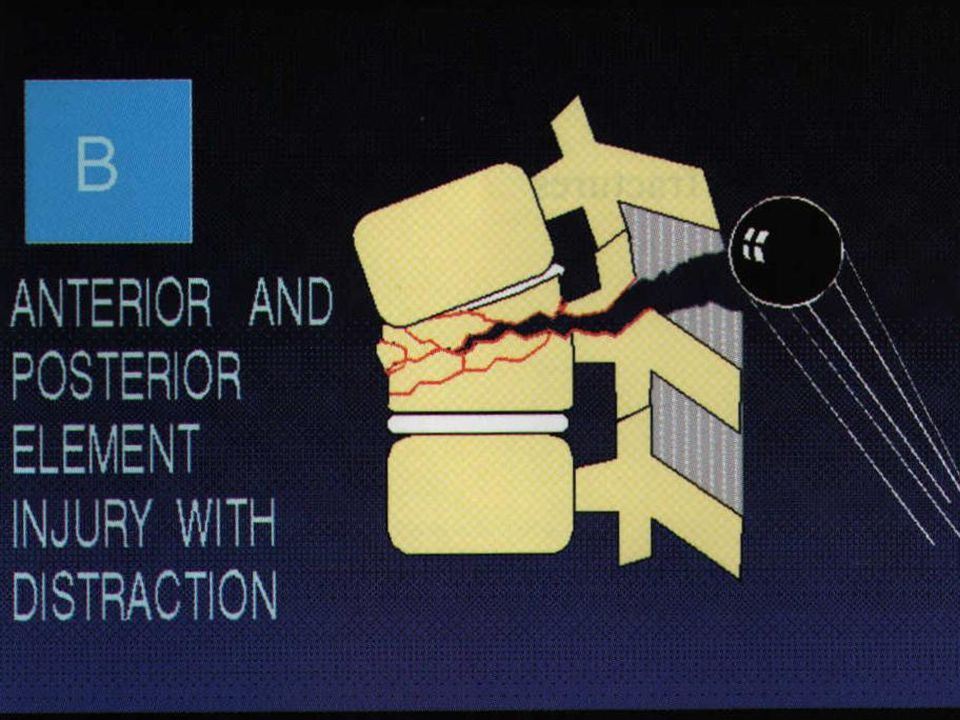
AO Classification AO 1994 (Magerl et al) Type A = vertebral body compression posterior column intact Type B = anterior and posterior column injuries with distraction Type C = anterior and posterior column injuries with rotation
 Type A = vertebral body compression posterior column intact Type B = anterior and posterior column injuries with distraction Type C = anterior and posterior column injuries with rotation")
24
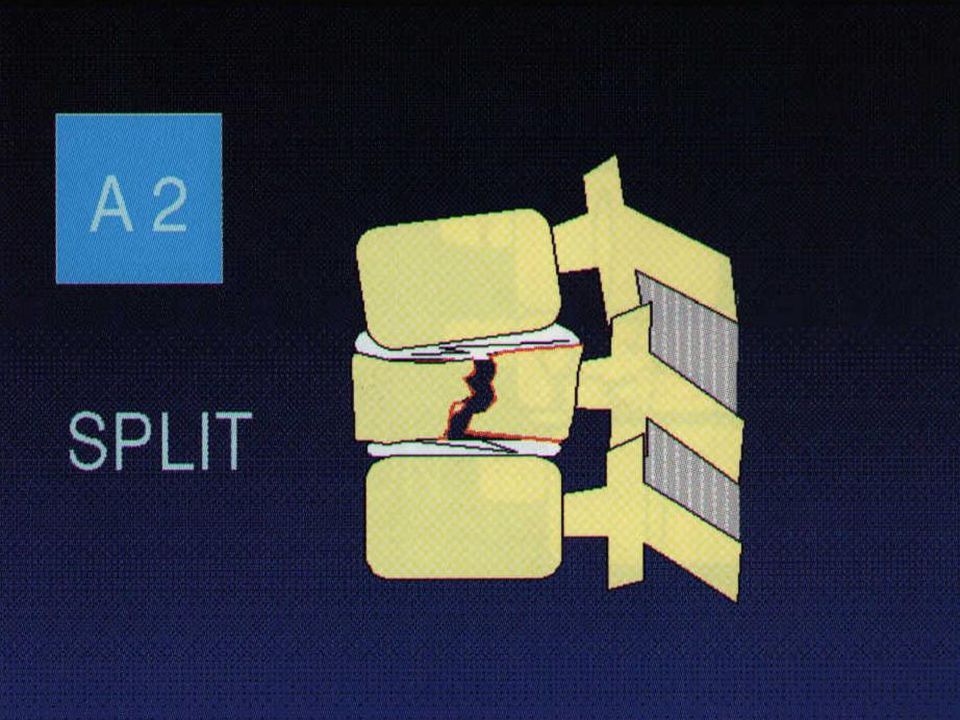
AO Classification A A1 =Impaction # (wedge) A2 =Coronal split # A3 =Burst # axial compression forces +/- flexion mainly vertebral body no translation
 A2 =Coronal split # A3 =Burst # axial compression forces +/- flexion mainly vertebral body no translation")
30
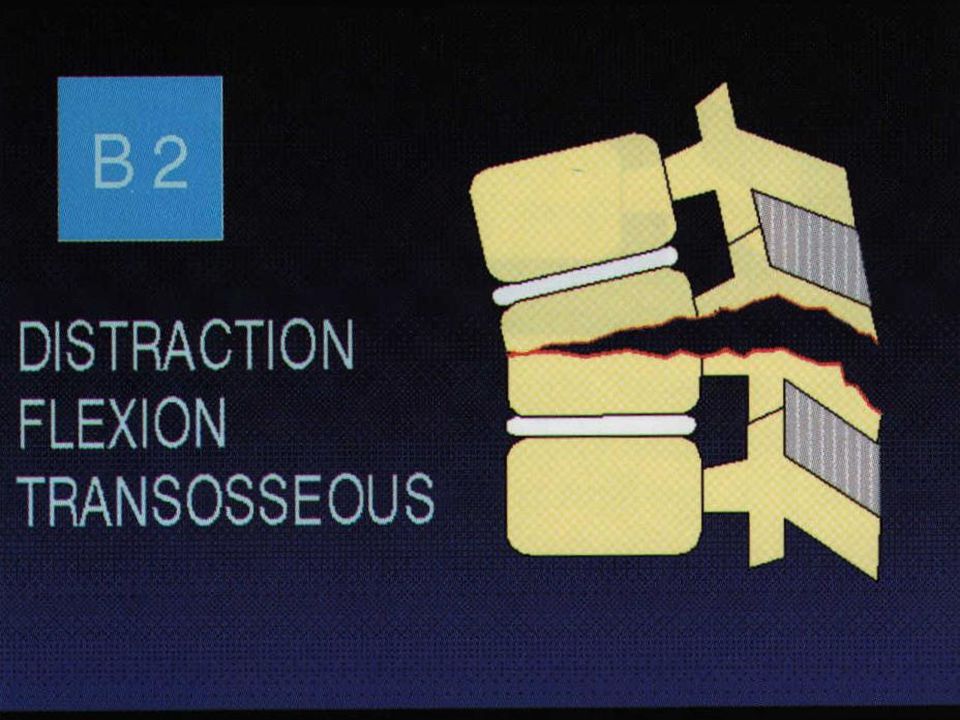
AO Classification B B1 = posterior ligamentous mainly (flex-distract) B2 =posterior osseous mainly (flex-distract) B3 =anterior disc disruption (hyperextend-shear) bilateral subluxation/ dislocation facet fractures frequent neurological injury
 B2 =posterior osseous mainly (flex-distract) B3 =anterior disc disruption (hyperextend-shear) bilateral subluxation/ dislocation facet fractures frequent neurological injury")
35
AO Classification C C1 =type A with rotation C2 =type B with rotation C3 =rotational shear injuries high neural injury rate rotation and translation facets, TPs, ribs, neural arch #s all ligaments discs

40
AO alphanumeric system Type A – vert body compression 1 impaction 2 split 3 burst Type B – ant & post element inj with distraction 1 ligament 2 bony 3 + ant disruption Type C – ant & post element inj with rotation 1 Type A + rotation 2 Type B + rotation 3 rotational sheer

41
Non – Operative Treatment Options No treatment advice / restrict activity Spinal ‘immobilisation’ Bed rest Lumbar pillow / Log rolling Casting / Bracing Combination treatment

42
THE AIMS OF TREATMENT Prevent neurological deterioration Minimise spinal deformity Fracture healing Minimise complications Acceptable function

43
Indications - Clinical Other skeletal injuries Co-existing medical problems (Unfit) Co-operative patient Normal Trunk Control Age of patient Patient preference
 Co-operative patient Normal Trunk Control Age of patient Patient preference")
44
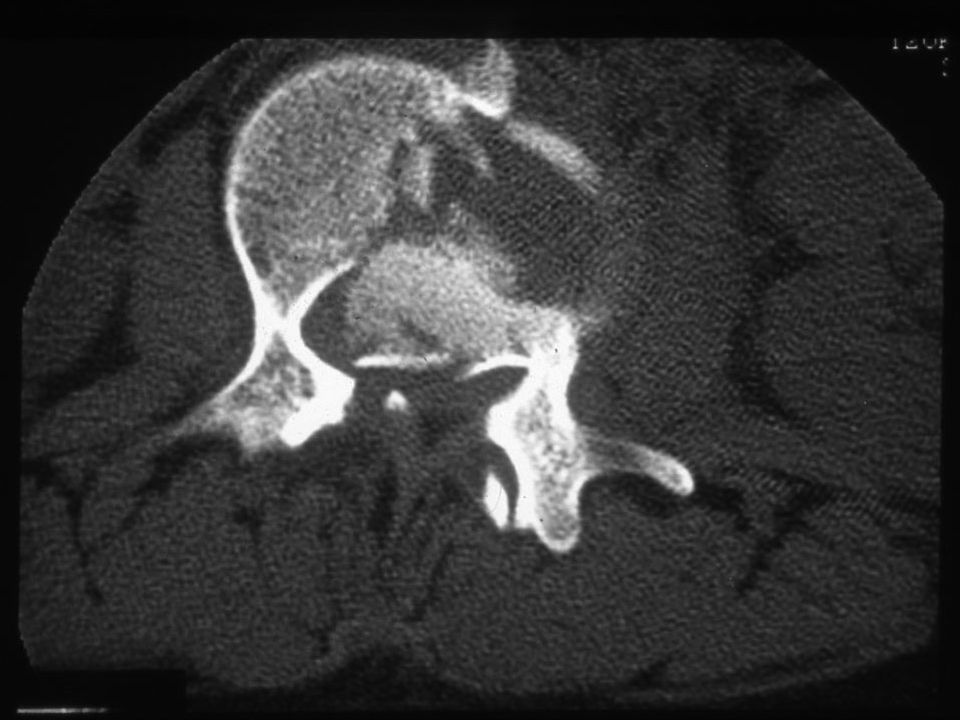
Stable Burst Fracture (A3)
")
45
Stable A3 Fracture Bed Rest until Normal Trunk Control Standing X Rays ? Use extension Brace or Cast

46
Time for Conservative Treatment Bed rest range: 1 - 8 weeks usual: 4 - 6 weeks TLSO range: 6 - 26 weeks usual: 6 - 12 weeks

47
Complications Bed rest sequelae Respiratory compromise Worsening of deformity Neurological deterioration

48
Thoraco-Lumbar Fractures Unstable Displaced Neurological Deficit Surgical Management

49
Advantages of Instrumentation Simplify care Early mobilisation Improve anatomical result Better neurological recovery? SPINAL TRAUMA

50
Scoliosis Research Society Multicentre Spine Fracture Study Gertzbein Spine Vol 17;528-540

51
Gertzbein- Neurology Surgical had greater % improvement in Function. At one year surgical group signifigantly greater relative improvement in motor score. Score 69.2% vs 14 (p<0.00001) At 2 yrs Score 59% vs 16 (p,0.00003)
 At 2 yrs Score 59% vs 16 (p, ).")
52
Gertzbein - Pain Kyphotic Deformity < 30 degrees@ 2 yrs had significantly more pain Overall surgical group had less pain than non surgical group.

53
Neurological recovery improved?

56
Fixation Techniques for T/L Spine

57
Choice of Approach Provide optimal exposure, Anatomically based, Extensile, Appropriate to pathology, Safe, Low morbidity, Fast and simple.

58
Extensile Approach Exposure that will vie effectively with the “Great arsenal of chance” must be a match for every shift, and therefore have a range, extensile like the tongue of the chameleon, to reach where it requires. Henry A.K. 1957 Extensile Exposure. Livingstone, Edinburgh.

59
Posterior Fixation of Fractures Short Segment Fixation Restoration of Sagittal Alignment Stable Fixation Maintain Correction

60
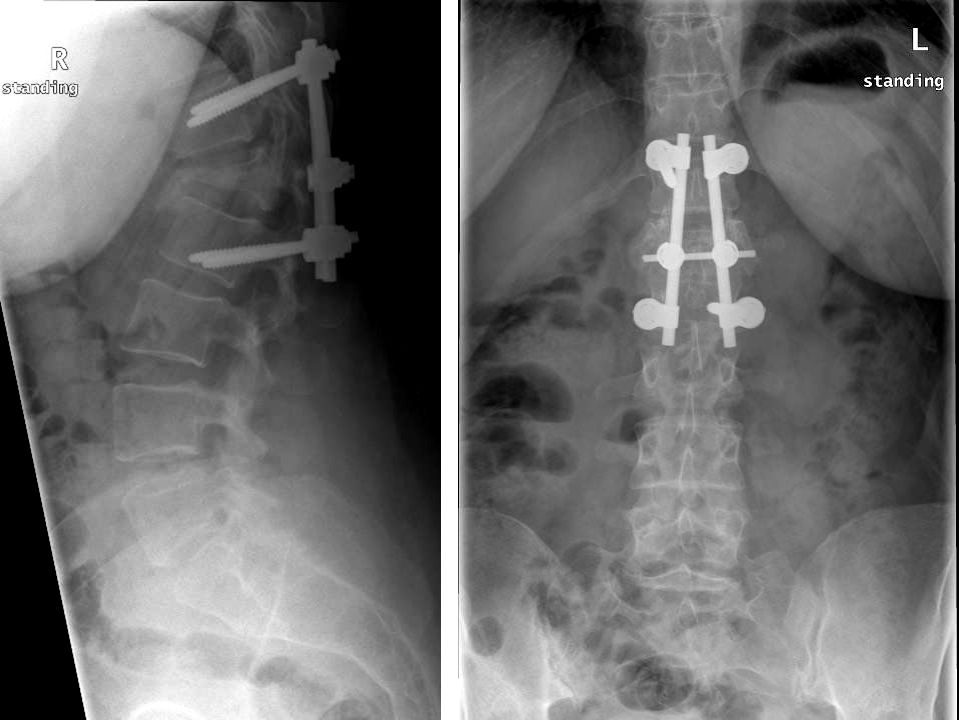
USS2 Fracture Set – Fixation of A3 Fracture

61
Treatment of A fractures A1 Conservative A2 Mostly Conservative (Depends on Displacement on Standing X Rays) A3 ?Conservative if posterior column intact
 A3 Conservative if posterior column intact")
62
Treatment of A3 Fractures Retropulsed fragment relevant only if neuro deficit! (Fidler 1987) Middle column does not exist
 Middle column does not exist.")
63
A3 Fractures Indications for surgery Neuro Deficit Loss of 50% Ant body height Kyphosis > 25 degrees Canal Encroachment > 50% Persistent Post Tenderness Slow to regain trunk control

64
Posterior ligamentous disruption

66
A3 Fracture

68
Neurological Deficit Complete -Stable Short Segment Fixation usually Front and back Incomplete- Posterior fixation repeat CT scan if necessary second stage anterior decompression

69
Canal Clearance post Surgery Plus Transpedicular Bone Grafting

70
Treatment of B Fractures Difficult to diagnose Easy to fix Close gap in posterior elements to restore tension band function of posterior elements

73
Anterior Ligamentous Injury

75
Treatment of C Fractures Grossly Unstable Comminuted Rotational Injuries Usually Require either; Longer Fixation Front & Back Fixation

76
C Type Fracture L2

79
24 yr old cyclist 5 level spinal injuries

82
Timing of Surgery Optimal Conditions usually next day Influence of Associated Injuries Beware early Anterior Surgery

83
Displaced Unstable Thoracic Fractures 50% have neurological deficit All have associated chest injury Chest condition deteriorates after 1 st 24 hrs Early surgery simplifies patient care Displaced Sternal fracture always exclude upper thoracic fracture

86
Indications in spinal trauma Anterior compression with progressive neuro deficit. Late surgery. Anterior decompression required. Anterior column support in comminuted # ANTERIOR INSTRUMENTATION

87
Anterior Compression with Progressive Neurological Deficit

88
Late Surgery

91
Post traumatic kyphus + partial Neuro Deficit

93
Thoraco-Lumbar Fractures Unstable Displaced Neurological Deficit Surgical Management

95
Spinal Trauma Case 1 15 year old girl jumped/fell 30 feet Skull fracture small extradural Alert, orientated but irritable with headache and minor meningism No neurological function below fracture

99
Spinal Trauma 50 year old woman Referred to spinal surgeon 3 weeks post fracture Mechanism fall down 3 stairs Bilateral foot drops but still ambulant Neurological deficit apparently increased

104
Spinal Trauma 15 year old RTA Neurologically intact 2 Previous attempts at fixation failed Referred for conservative treatment

107
Spinal Trauma 19 Year old Skiing Accident Fracture L1 Treated in France Neurologically Normal Undisplaced A3 Fracture Neurosurgical fixation

108
Spot the 7 mistakes

109
The 7 Errors Didn’t need Fixing Didn’t need Decompression Rods too thin Screws too short Screws too thin Screws in fractured vertebra Left L2 screw missed

112
Denis’ 3 columns

Similar presentations