Download presentation
Presentation is loading. Please wait.

1
The Aging Process from a Quality of Life Perspective Ingalill Rahm Hallberg, Professor, Director of the Swedish Institute for Health Sciences Assistant Vice Chancellor at Lund University 2/29/2016

2
Greetings from Lund University; 38 000 students at graduate and postgraduate level (about 3000) 2/29/2016 Ingalill Rahm Hallberg, professor
 2/29/2016 Ingalill Rahm Hallberg, professor")
3
Sweden and the population aging 9,3 million inhabitants 17,5% 65 years or above- 21% 2020 5 % 80 years or above 7% 2030 The health care, long term care and social service – financed through taxes – in solidarity and distributed in accordance to needs Ingalill R Hallberg, 2008-06-20 3

4
4

6
6

7
Reasons for the development Low and decreased fertility Increased life expectancy – 82,7 for women and 78, 4 for men (2004 - Swe) Large birth cohorts approaching retirement and later on approaching the time were they need help for activities of daily living
 Large birth cohorts approaching retirement and later on approaching the time were they need help for activities of daily living")
8
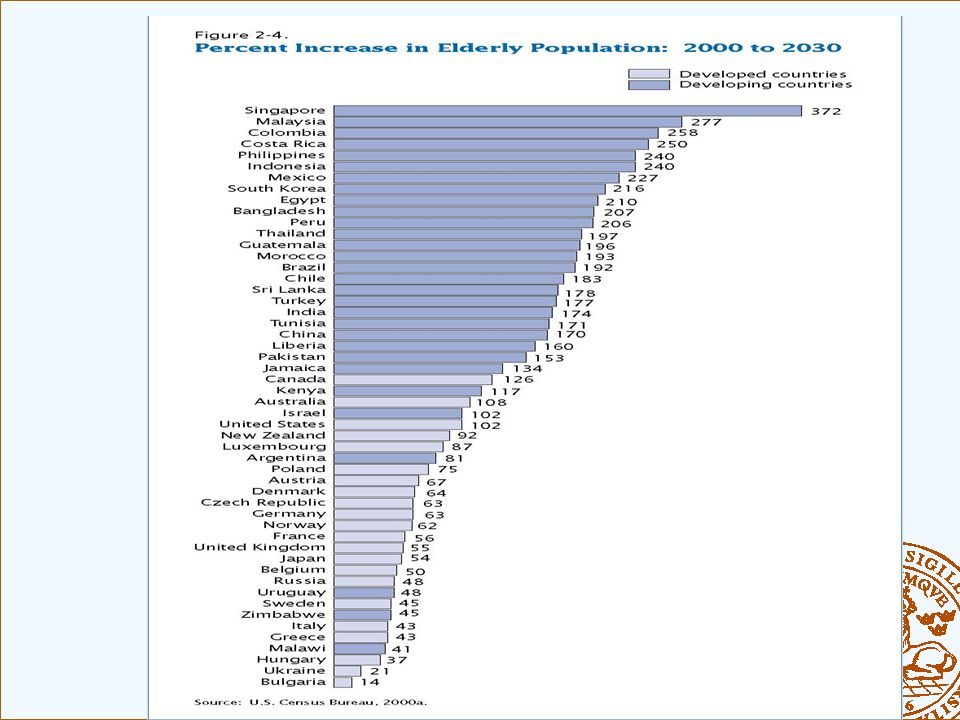
Mainly a win – win situation ? The problem is not the increased proportion of people 60 - 65 years and above - It is in fact a societal resource! The problem is mainly that the cohorts are large and will at the same time reach the age were functional disability is prevalent For instance percent 80+ increases from 21% to 40% between 2000-2030 in Japan – similar figures in Sweden and in many other countries Thereafter a drop in the size of the population!! Ingalill R Hallberg, 2008-06-20 8

9
What do we get with regard to increased life expectancy? Postponement of morbidity – about the same length and severity of morbidity? Compression of morbidity – a shorter compressed period of morbidity? Expansion of morbidity – a longer period of morbidity and also a longer period of impaired functional ability May be a combination of postponement and expansion – but not neccessarily a problem due to medical development

10
The popularity of the concept of quality of life The post modern society, away from survival and towards living conditions and people’s standard of living The development in health care sector –emphasis on evidence based medicine showed mortality and survival to be blunt measures of treatment quality and effectiveness The development in treatment meaning that people survive but have to live with chronic diseases or long term complications not dying from them. The ability to treat more effectively also very old people and very premature babies 2/29/2016 Ingalill Rahm Hallberg, professor

11
Model explaining quality of life or life satisfaction Social Resources;social network & social support Material Security; education, income, savings Cognitive Efficacy; personality, intellectual resources Physical Health & Functional Status Life Activity; active involvement in life/society 2/29/2016 Ingalill Rahm Hallberg, professor

12
The European study of Adult well-being Factors contributing to aging well in 6 European countries: 2002-03; people 50-90 years of age The model explained about 30-57% of the variance SWE: Material security – strongest predictor.53 Followed by; Health.20, Social support resources.19, Life activity.09 Self worth were predicted by health material security, social support resources and life activities 2/29/2016 Ingalill Rahm Hallberg, professor

13
The process of aging from a QoL perspective The period from retirement to death is marked by different phases – with different values and different living conditions. 1.Healthy, active, mobile and in most cases with high quality of life – in our studies about 15-20 % report low QOL 2.Increased morbidity, sometimes multimorbidity, increasingly higher number of health complaints – not neccessarily low QOL

14
Cont 3. Increasingly dependent on others for daily living due to limitations in functional ability, aging per se and negative impact from diseases, multimorbidity, or other health problems – a turning point with increasingly high risk of low QOL 4.Last period of life – increased risk for low QOL

15
Age of retirement and life expectancy Ingalill R Hallberg, 2008-06-20 15 YearWomen’s life expectancy Men’s life expectancy Age of retirement in the pension system 191358 year56 year67 year 200983 year79 year67 (but using the 1913 equation should be 92 year) 2060 (acc to SCB) 87 year85 yearIf using the 1913 equation should be 96 year
 2060 (acc to SCB) 87 year85 yearIf using the 1913 equation should be 96 year")
16
Prevalence of long term disease 2002-04 SWE Age group 55-64 Age group 65-74 Age group 75-84 Age group 85+ Endocrine diseases like diabetes 12,113,816,414,5 Circulatory diseases 26,542,553,956,6 Diseases related to mobility 21,522,521,322,2 Ingalill R Hallberg, 2008-06-20 16 From Living conditions of the elderly: work, economy, health and social networks 1980 – 2003; SCB 2006

17
Functional limitations and QOL 10-15 % of the time after 65 years of age is marked by such a functional impairment that help from others is needed to manage daily living Functional impairment developes around 80 years of age or thereafter Healthy life style can postpone this development

18
Health complaints at high age contributes more to low QOL than diseases; prevalence in people 75 years and above

19
Functional ability; development over time; SWE percent change from 1980- 2003 Age 55-64Age 65-74Age 75-84Age 85+ Self reported health poor -1,1-3,2*-4,9*-0,3 Long term disease+2,2+6,6*+4,0*+4,0 Severe complaints+1,9-0,1+0,4-2,6 Continous medication+7,8*+12,6*+13,6*+10,6 Decreased work ability -0.9-5.9*-7,3*-2.0 Mobility restrictions * Means significant change -4,6*-8,3*-14,2*-3,5 Ingalill R Hallberg, 2008-06-20 19 From; Living conditions of the elderly: work, economy, health and social networks 1980 – 2003; SCB 2006

20
Health promotion strategies in the early stage of the aging process Activity and independency for ADL Physically active Social involvement and activities Nutrition and not undernourished or obese Security and safety Cognitively active No abuse of food, alcohol or the like Ingalill R Hallberg, 2008-06-20 20

21
Mean age at exit from labour market in 15 EU countries From Living conditions of the elderly: work, economy, health and social networks 1980 – 2003 SCB 2006 Ingalill R Hallberg, 2008-06-20 CountryMean age at exit Sweden Ireland 63 Portugal Spain 62 Denmark Norway 62 Germany Netherlands 61 Italy EU 15 61 Greece Belgium 60 France Austria Luxembourg 60 58-59

22
Factors determining retirement Expected standard of living after retirement including disability pension Labourmarket and working conditions Being in the labour market means structure to life provides social relationships means working towards and participating in producing societal goals Ingalill R Hallberg, 2008-06-20 22

23
The current trends In the beginning of the 1990 a decreasing participation in the labour market From 2000 an increasing participation among 55+ among men and women – in particular among those 63-64 years of age Sweden the highest retirement age and participation in labour market Perhaps the answer is; Flexibel labour market and working conditions towards the end of working life Ingalill R Hallberg, 2008-06-20 23

24
Older peoples’ views A majority wants to end before 65 years old Desire more leisure time (80%) Declining health (30%) Positive attitude towards work means wanting to go on longer Poor health and socioeconomic conditions means low will to stay on longer Physical demands in the working environment means wanting to leave earlier Among women, weak social support means low will to go on longer Ingalill R Hallberg, 2008-06-20 24
 Declining health (30%) Positive attitude towards work means wanting to go on longer Poor health and socioeconomic conditions means low will to stay on longer Physical demands in the working environment means wanting to leave earlier Among women, weak social support means low will to go on longer Ingalill R Hallberg,")
25
Thank you for your attention!

Similar presentations