Download presentation
Presentation is loading. Please wait.

1
The theme of the lecture: “Bronchial asthma
The theme of the lecture: “Bronchial asthma. Chronic obstructive pulmonary disease. The syndrome of hyperinflation of lungs. Pulmonary emphysema" Ass-prof.N.Bilkevych

3
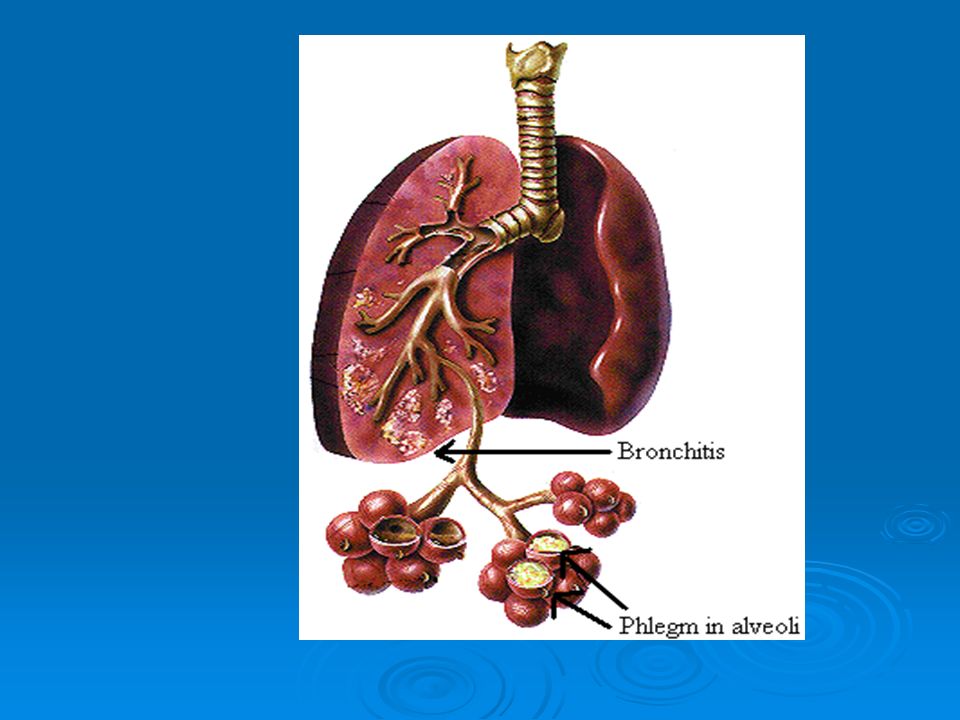
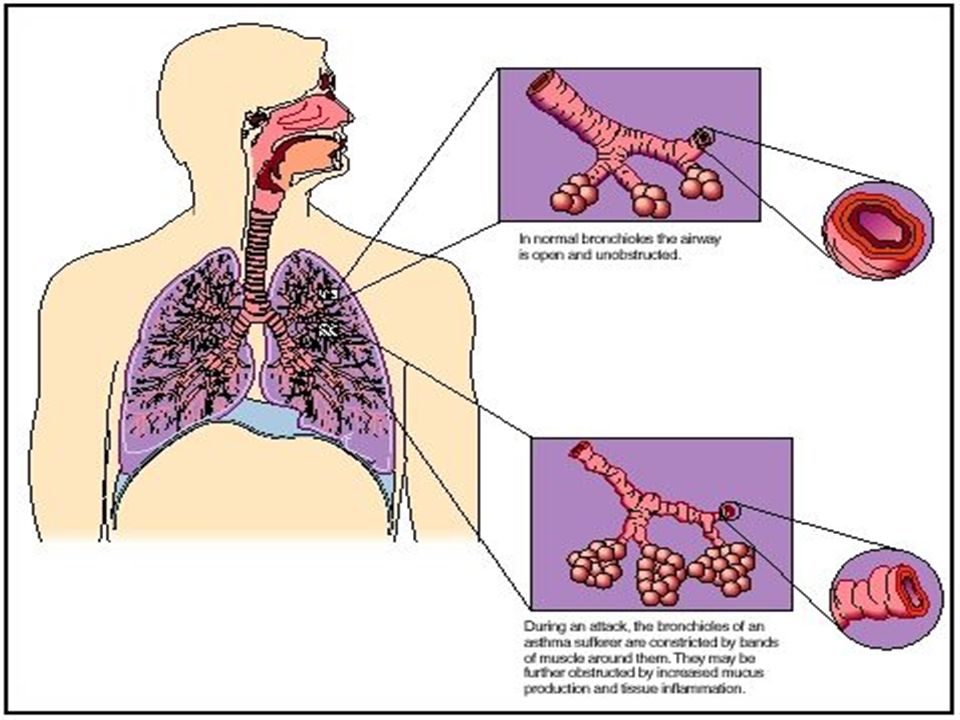
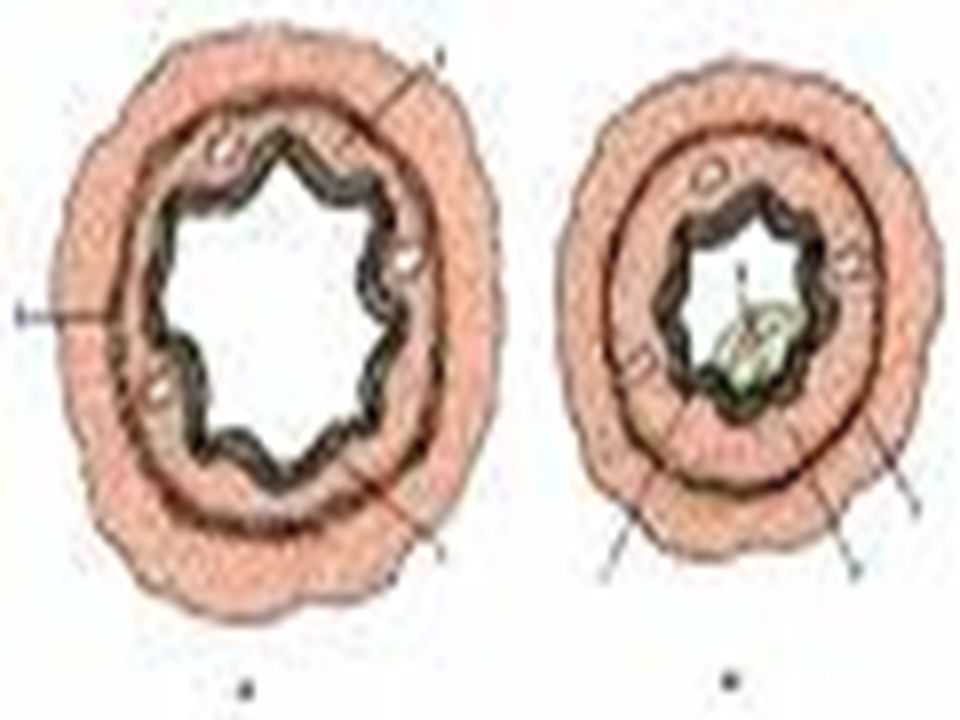
The syndrome of bronchial obstruction
Obstructio (lat.) – barrier, obstracle. Causes of bronchial obstruction: - accumulation of fluid in fine bronchi; - edema of bronchial mucosa; - spasm of bronchial smooth muscles; - poor elasticity of lungs.
 – barrier, obstracle. Causes of bronchial obstruction: - accumulation of fluid in fine bronchi; - edema of bronchial mucosa; - spasm of bronchial smooth muscles; - poor elasticity of lungs.")
4
Pulmonary emphysema

5
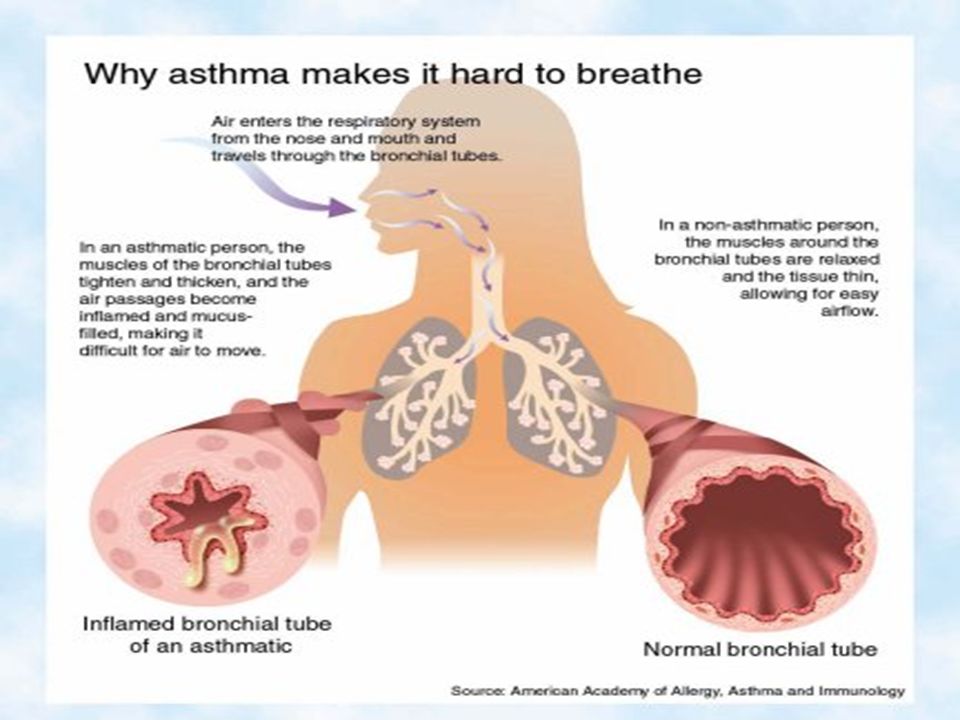
Respiratory system anatomy

6
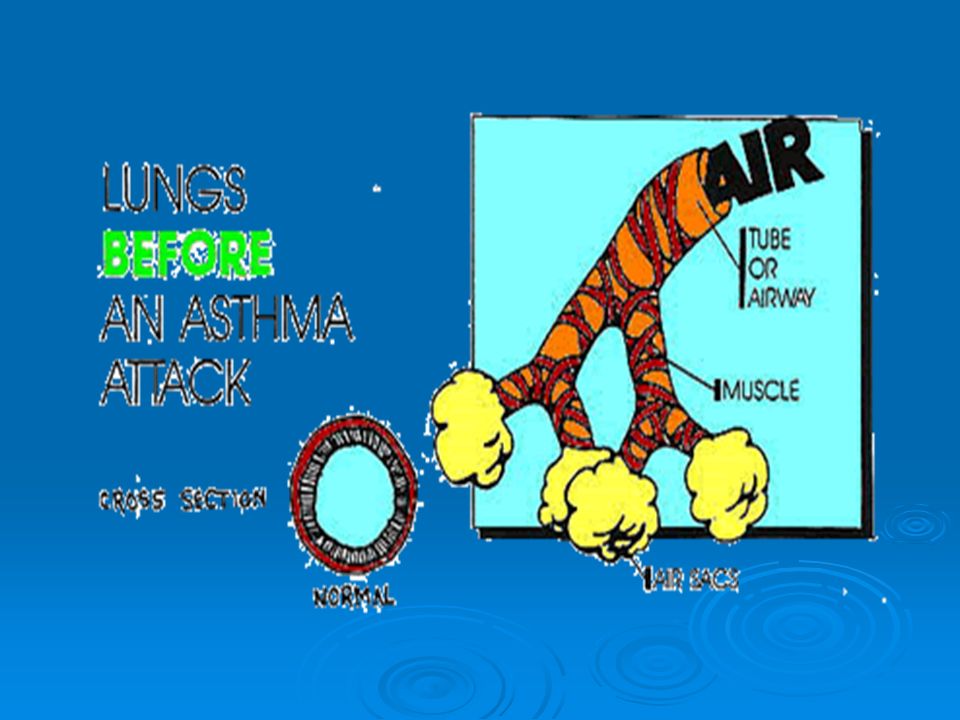
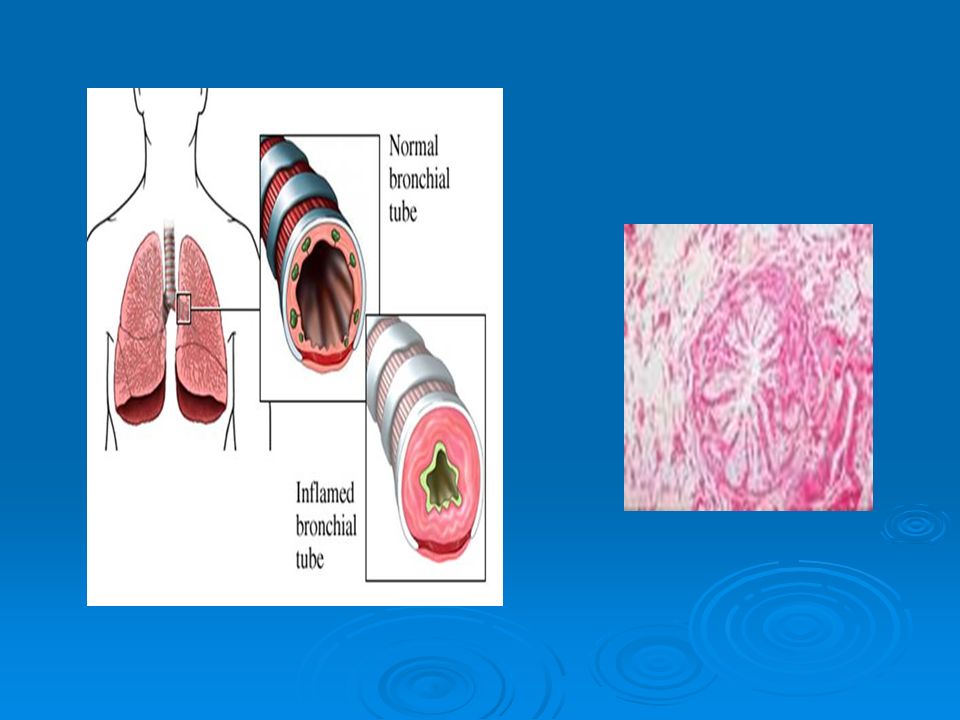
Bronchial asthma Asthma is a bronchial hypersensitivity disorder characterized by reversible airway obstruction, produced by a combination of mucosal edema, constriction of the bronchial musculature, and excessive secretion of viscid mucus, causing mucous plugs. Essentials of Diagnosis: • Recurrent acute attacks of dyspnea, cough, and mucoid sputum, usually accompanied by wheezing. • Prolonged expiration with generalized wheezing and musical rales. • Bronchial obstruction reversible by drugs

7
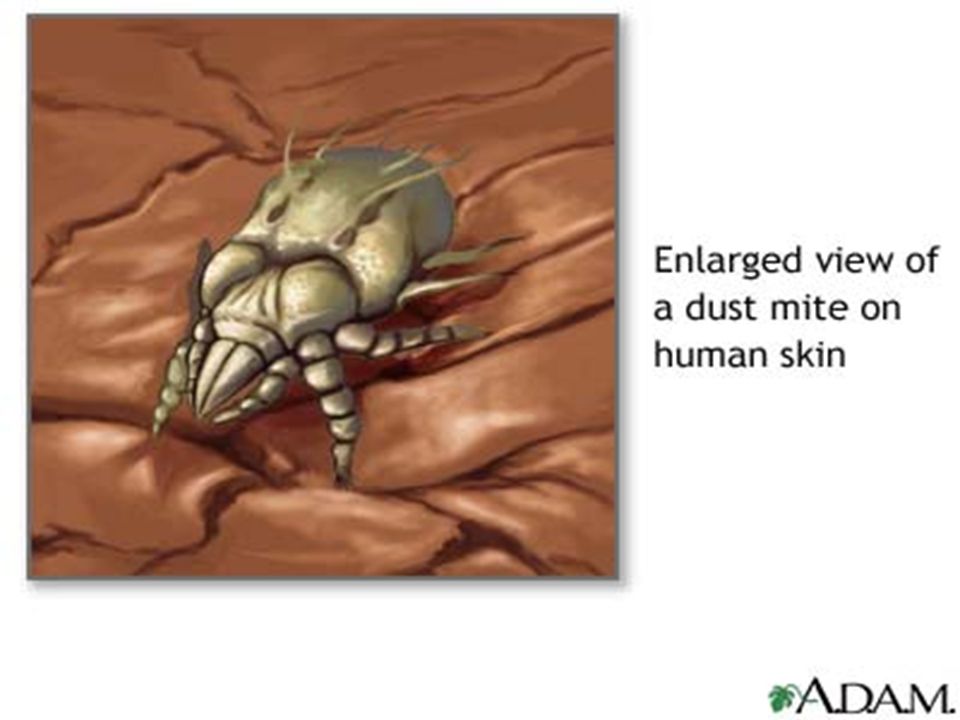
Ethiology 40-80 % of patients has heredital predisposition Acquired ethiological factors Domestic allergens ( dust, insect allergens, fungi, animal wool, epidermis) Environmental allergens ( fungi, insect allergens, pollen etc) Food allergy ( milk, flour, fish, chemical admixtures to food) drugs ( antibiotics, enzymes, aspirin) bacterial allergens ( neisseria, Staphylococcus aureus, Candida albicans, mycoplasma, helmints)
 Environmental allergens. ( fungi, insect allergens, pollen etc) Food allergy. ( milk, flour, fish, chemical admixtures to food) drugs. ( antibiotics, enzymes, aspirin) bacterial allergens. ( neisseria, Staphylococcus aureus, Candida albicans, mycoplasma, helmints)")
30
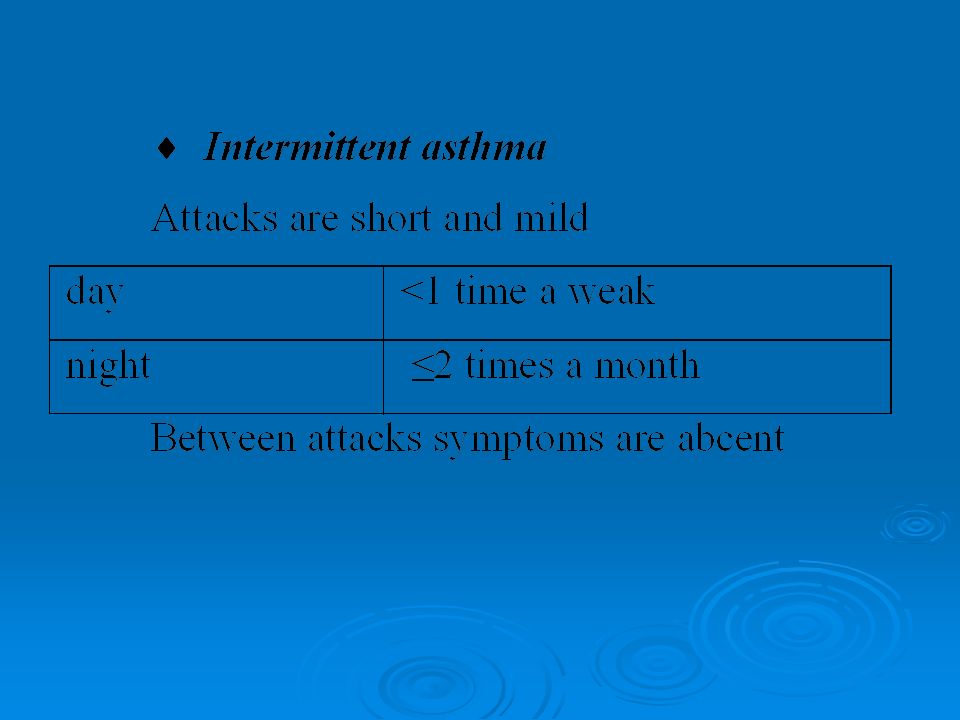
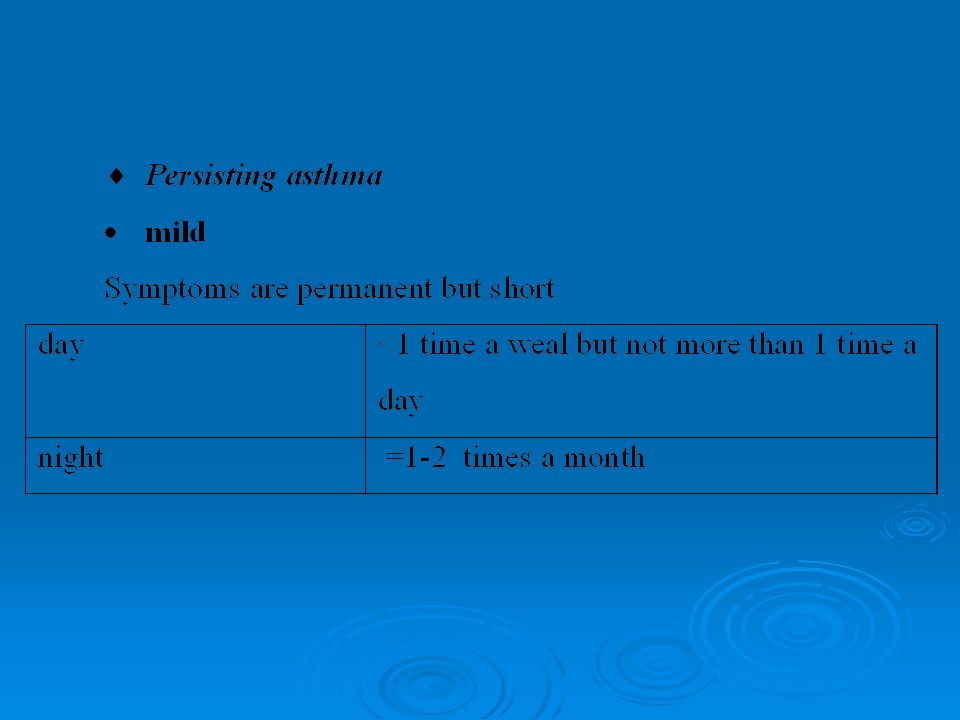
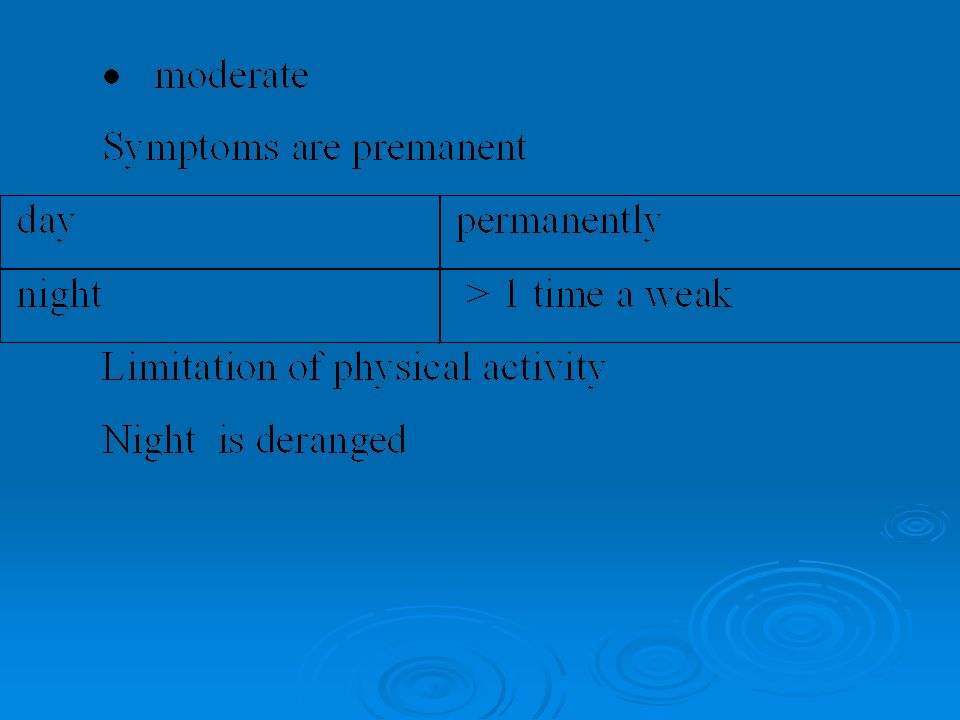
Clinical pattern

32
Appearance of a patient during attack of asthma

36
Дослідження харкотиння

37
спірограма

40
Chest X-ray in asthma

41
X-ray shows pulmonary emphysema

42
Endoscopic findings: hyperemia, edema of bronchial mucosa, hypersecretion

43
Allergic tests allow to determine allergens

44
Positive reaction

47
Usage of inhaler

48
Solotvino (salt caves)
")
49
Solotvino (salt caves)
")
50
Solotvino (salt caves)
")
52
Physiotherapy

53
Climatotherapy

54
Elimination of risk-factors

56
Bronchoscopy is used if it is necessary

57
Chronic obstructive pulmonary disease (COPD)
The common combination of chronic bronchitis and emphysema has also been termed chronic obstructive airways disease (COAD) or chronic obstructive pulmonary disease (COPD). This is a morbid condition characterized by non-reverseble bronchial obstruction caused by deformation and sclerosis of bronchial tree due to persistent inflammation. Up to 20% of adults worldwide have the disease, and this proportion is higher in heavily industrialized countries. Chronic bronchitis occurs in the majority of heavy smokers, but significant airway obstruction or emphysema, or both occurs in only a minority. It is the third most common cause of death in men over 65 years (60 per ), and is more common in men (8%) than women (3%). COPD develops in at least 80% of smokers.
 or chronic obstructive pulmonary disease (COPD). This is a morbid condition characterized by non-reverseble bronchial obstruction caused by deformation and sclerosis of bronchial tree due to persistent inflammation. Up to 20% of adults worldwide have the disease, and this proportion is higher in heavily industrialized countries. Chronic bronchitis occurs in the majority of heavy smokers, but significant airway obstruction or emphysema, or both occurs in only a minority. It is the third most common cause of death in men over 65 years (60 per ), and is more common in men (8%) than women (3%). COPD develops in at least 80% of smokers.")
58
Causes of COPD I. Localized A. Congenital
B. Compensatory due to lung collapse, scarring or resection C. Partial bronchial obstruction Neoplasm Foreign body D. MacLeod'syndrome II. Generalized A. Idiopathic B. Senile C. Familial (alpha-1-anti-trypsin deficiency) D. Associated with chronic bronchitis, asthma or pneumoconiosis.
 D. Associated with chronic bronchitis, asthma or pneumoconiosis.")
66
Treatment The most important step in management is to persuade the patient to stop smoking. Bronchodilators may achieve some reversal of airways obstruction Corticosteroids have a role in some patients. Surgical removal of large bullae is occasionally helpful. Oxygen is usually given via nasal cannulae. Occasionally transtracheal oxygen therapy (TTOT) via a small polyethylene catheter introduced directly into the trachea. Long-term oxygen therapy from cylinders or an oxygen concentrator may be of value in patients with chronic stable respiratory failure. The flow rate and concentration are adjusted to relieve arterial hypoxaemia while avoiding carbon dioxide narcosis. Infections are frequent, and it is important to educate patients in the early recognition of symptoms and signs, for example change of sputum colour and quality, fever or increasing wheeze. Many patients should be given a supply of antibiotics to keep at home for self-medication.
 via a small polyethylene catheter introduced directly into the trachea. Long-term oxygen therapy from cylinders or an oxygen concentrator may be of value in patients with chronic stable respiratory failure. The flow rate and concentration are adjusted to relieve arterial hypoxaemia while avoiding carbon dioxide narcosis. Infections are frequent, and it is important to educate patients in the early recognition of symptoms and signs, for example change of sputum colour and quality, fever or increasing wheeze. Many patients should be given a supply of antibiotics to keep at home for self-medication.")
67
Thank you for your attention!

Similar presentations





















 into the atmosphere Filter, moisten,>")
 Dr. Walaa Nasr Lecturer of Adult Nursing Second year.>")






 is one of the most common lung disease Makes it difficult to breathe There are two main forms of COPD.>")
 Asthma.>")








