Download presentation
Presentation is loading. Please wait.

1
1 Respiratory system Lecture 1 Faisal I. Mohammed, MD, PhD Yanal A. Shafagoj MD, PhD University of Jordan

2
In general the 5 lectures will cover the following Respiratory Physiology Topics: 1. Overview, potential causes of hypoxia, analyzing different compartments in term of gas compositions 2. Mechanics of Breathing (Lung Ventilation(, Pulmonary Function Test and Airway Resistance 3. Lung Compliance and IRDS 4. Gas Exchange and Transport 5. Regulation of Lung Ventilation, high altitude, exercise etc

3
Exchange of gases Directionality depends on gradients “Pressure difference “! Atmosphere to blood- Blood to tissues Excretion of some volatile waste products e.g. acetone and alcohol. Helps blood and lymph flow (venous return)…important Regulation of body temperature by evaporation of water from the respiratory passages to help heat loss from the body Regulation of pH…Acid-base balance which dependents on rate of CO2 retension BP regulation by converting AI to AII Protection…..Vocalization etc Plus other things you learn them from your lecture… if we have enough time
…important Regulation of body temperature by evaporation of water from the respiratory passages to help heat loss from the body Regulation of pH…Acid-base balance which dependents on rate of CO2 retension BP regulation by converting AI to AII Protection…..Vocalization etc Plus other things you learn them from your lecture… if we have enough time.")
4
What are the Potential Causes of Hypoxia – inadequate oxygenation of lungs Atmosphere…high altitude every 5.5 km above sea level, Patm decreases by 50% – Increase R – Non-inflatable balloon – Cardiovascular level anemia, abnormal hemoglobin blood flow and heart problem – Histotoxic….. Cyanide poisoning - The controller system…muscles and nerves University of Jordan 4

5
Introduction Respiration is the process by which the body takes in and utilizes oxygen and gets rid of CO 2. Three determinants of respiration Respiration depends on three things: the lungs, the blood, and the tissues.

6
The lungs: The lungs must be adequately ventilated and be capable of adequate gas exchange. Ventilation: is determined by the activity of the control system (respiratory system), the adequacy of the feedback control systems (neural and hormonal), and the efficiency of the effector system (muscles of respiration). Gas exchange: depends on the patency of the airways, the pressure gradient across the alveolar- capillary membrane, the diffusability of individual gases and the area and thickness of the exchange membrane.
, the adequacy of the feedback control systems (neural and hormonal), and the efficiency of the effector system (muscles of respiration). Gas exchange: depends on the patency of the airways, the pressure gradient across the alveolar- capillary membrane, the diffusability of individual gases and the area and thickness of the exchange membrane..")
7
The Blood: The blood must pick up, carry and deliver O 2 and CO 2 in amounts that are appropriate to the body’s need. It depends in the presence of adequate amount of the correct type of Hb, the cardiac output, and local perfusion.

8
The Tissues: Individual cells must be capable of taking up and utilizing O 2 properly. Hypoxia can therefore result from a fault at any point along this lungs-blood- tissue chain.

9
Respiratory component element Respiration is the exchange of gas between the body and the environment. External respiration : the exchange of gases between pulmonary blood and the external environment, which involves not only diffusion across the lung capillaries ( pulmonary gas exchange, but also the bulk movement of gases in and out of the lungs (pulmonary ventilation). Internal respiration : the exchange of gases between the tissue cells and the systemic capillaries. The diffusion of gases between the interstitial fluid and the cytoplasm. Gas transport in the blood : physical solvation and chemical constitution.
. Internal respiration : the exchange of gases between the tissue cells and the systemic capillaries. The diffusion of gases between the interstitial fluid and the cytoplasm. Gas transport in the blood : physical solvation and chemical constitution..")
10
10 Structures of the Respiratory System University of Jordan

11
11 University of Jordan

12
Respiratory Zone Region of gas exchange between air and blood. Includes respiratory bronchioles and alveolar sacs. Must contain alveoli.

13
Basics of the Respiratory System Functional Anatomy….Functions of the anatomic dead space All the structures air passes through before reaching the respiratory zone. Warms and humidifies inspired air. Filters and cleans: Mucus secreted to trap particles in the inspired air. Mucus moved by cilia to be expectorated. All divided into Upper respiratory tract Entrance to larynx Lower respiratory tract Larynx to alveoli (trachea to lungs)
.")
14
The Bronchial Tree Cartilage and protection The first 10 generations have cartilage and thus have support and therefore are somehow non-collapsible structures 12 th to 16 th are called bronchioles (diameter < 1 mm) lack cartilage….and thus collapsible From 0-16 is the conductive zone From 17-23 is the respiratory zone
 lack cartilage….and thus collapsible From 0-16 is the conductive zone From is the respiratory zone")
15
15 Microscopic Anatomy of Lobule of Lungs University of Jordan

16
16 Alveoli Cup-shaped outpouching Alveolar sac – 2 or more alveoli sharing a common opening 2 types of alveolar epithelial cells Type I alveolar cells – form nearly continuous lining, more numerous than type II, main site of gas exchange Type II alveolar cells (septal cells) – free surfaces contain microvilli, secrete alveolar fluid (surfactant reduces tendency to collapse) University of Jordan
 – free surfaces contain microvilli, secrete alveolar fluid (surfactant reduces tendency to collapse) University of Jordan")
17
17 Components of Alveolus University of Jordan

18
Pneumocytes I and pneumocytes II

19
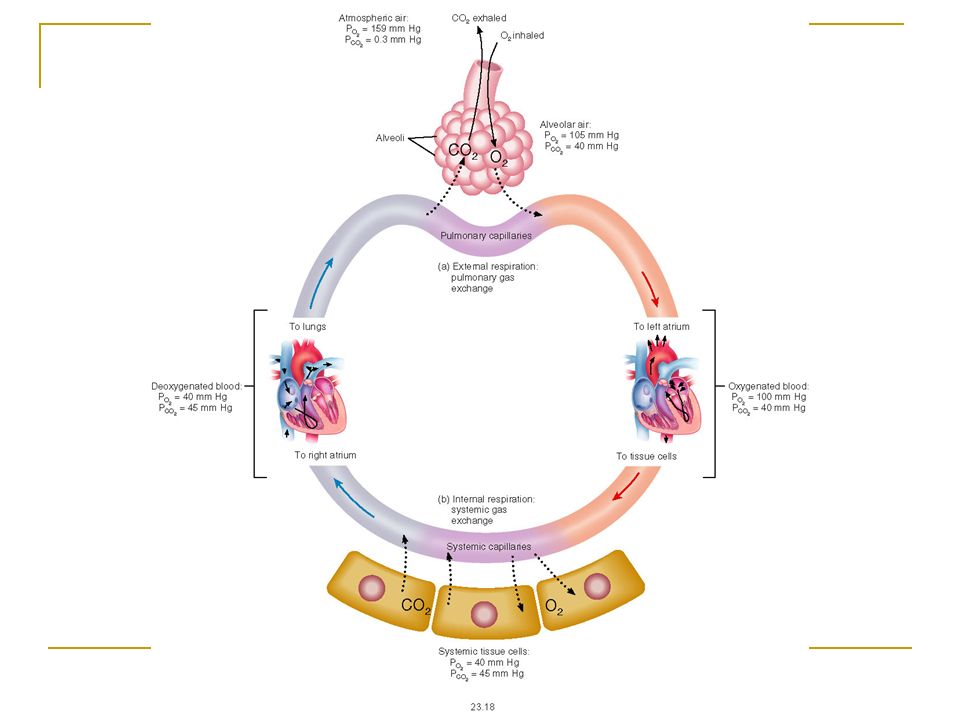
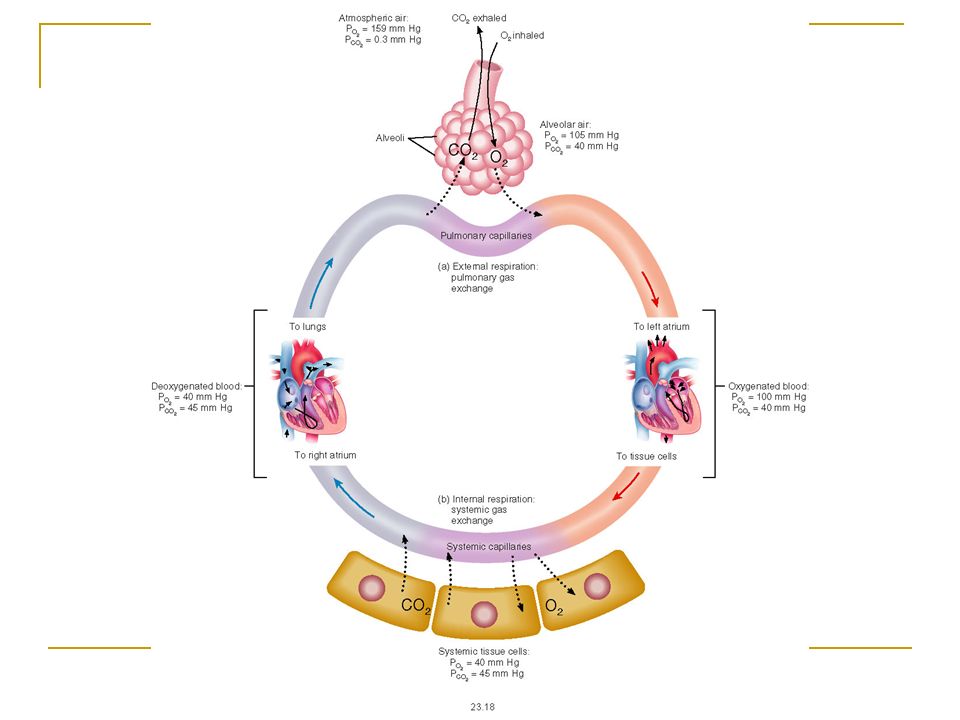
External Respiration Internal Respiration Schematic View of Respiration

20
Partial Pressures of Gases in Inspired Air and Alveolar Air Insert fig. 16.20

21
PO 2 and PCO 2 in different compartments. Atmospheric ADS AavE PO 2 160 15010210240120 PCO 2 ------40404627 PH 2 O---4747474747 PN 2 600563 571571571566 Total P760760760760704760

22
22 Exchange of Oxygen and Carbon Dioxide Dalton’s Law Each gas in a mixture of gases exerts its own pressure as if no other gases were present Pressure of a specific gas is partial pressure P x Total pressure is the sum of all the partial pressures Atmospheric pressure (760 mmHg) = P N2 + P O2 + P H2O + P CO2 + P other gases Each gas diffuses across a permeable membrane from the are where its partial pressure is greater to the area where its partial pressure is less The greater the difference, the faster the rate of diffusion University of Jordan
 = P N2 + P O2 + P H2O + P CO2 + P other gases Each gas diffuses across a permeable membrane from the are where its partial pressure is greater to the area where its partial pressure is less The greater the difference, the faster the rate of diffusion University of Jordan")
23
- is determined by its concentration in the mixture and by the overall pressure of the gas mixture P atm O 2 = P atm * FO 2 P atm O 2 = 760 mm Hg * 0.21 - in the liquid - partial pressure of the gas component, which is balanced with the liquid Partial pressure of the gas

24
24 Partial Pressures of Gases in Inhaled Air P N2 =0.786x 760mm Hg= 597.4 mmHg P O2 =0.209x 760mm Hg= 158.8 mmHg P H2O =0.004x 760mm Hg= 3.0 mmHg P CO2 =0.0004x 760mm Hg= 0.3 mmHg P other gases =0.0006x 760mm Hg= 0.5 mmHg TOTAL= 760.0 mmHg University of Jordan

26
26 External Respiration in Lungs Oxygen Oxygen diffuses from alveolar air (P O2 100 mmHg) into blood of pulmonary capillaries (P O2 40 mmHg) Diffusion continues until P O2 of pulmonary capillary blood matches P O2 of alveolar air Small amount of mixing with blood from conducting portion of respiratory system drops P O2 of blood in pulmonary veins to 100 mmHg Carbon dioxide Carbon dioxide diffuses from deoxygenated blood in pulmonary capillaries (P CO2 45 mmHg) into alveolar air (P CO2 40 mmHg) Continues until of P CO2 blood reaches 40 mmHg University of Jordan
 into blood of pulmonary capillaries (P O2 40 mmHg) Diffusion continues until P O2 of pulmonary capillary blood matches P O2 of alveolar air Small amount of mixing with blood from conducting portion of respiratory system drops P O2 of blood in pulmonary veins to 100 mmHg Carbon dioxide Carbon dioxide diffuses from deoxygenated blood in pulmonary capillaries (P CO2 45 mmHg) into alveolar air (P CO2 40 mmHg) Continues until of P CO2 blood reaches 40 mmHg University of Jordan")
27
Ventilation Mechanical process that moves air in and out of the lungs. [O 2 ] of air is higher in the lungs than in the blood, O 2 diffuses from air to the blood. C0 2 moves from the blood to the air by diffusing down its concentration gradient. Gas exchange occurs entirely by diffusion: Diffusion is rapid because of the large surface area and the small diffusion distance. Insert 16.1

28
Surface Tension (continued) Law of Laplace: Pressure in alveoli is directly proportional to surface tension; and inversely proportional to radius of alveoli. Pressure in smaller alveolus would be greater than in larger alveolus, if surface tension were the same in both. Insert fig. 16.11

29
Surfactant Phospholipid produced by alveolar type II cells. Lowers surface tension. Reduces attractive forces of hydrogen bonding by becoming interspersed between H 2 0 molecules. Surface tension in alveoli is reduced. As alveoli radius decreases, surfactant’s ability to lower surface tension increases. Disorders: RDS. ARDS. Insert fig. 16.12

30
30 Internal Respiration Internal respiration – in tissues throughout body Oxygen Oxygen diffuses from systemic capillary blood (P O2 100 mmHg) into tissue cells (P O2 40 mmHg) – cells constantly use oxygen to make ATP Blood O 2 drops to 40 mmHg by the time blood exits the systemic capillaries Carbon dioxide Carbon dioxide diffuses from tissue cells (P CO2 45 mmHg) into systemic capillaries (P CO2 40 mmHg) – cells constantly make carbon dioxide P CO2 blood reaches 45 mmHg At rest, only about 25% of the available oxygen is used Deoxygenated blood would retain 75% of its oxygen capacity University of Jordan
 into tissue cells (P O2 40 mmHg) – cells constantly use oxygen to make ATP Blood O 2 drops to 40 mmHg by the time blood exits the systemic capillaries Carbon dioxide Carbon dioxide diffuses from tissue cells (P CO2 45 mmHg) into systemic capillaries (P CO2 40 mmHg) – cells constantly make carbon dioxide P CO2 blood reaches 45 mmHg At rest, only about 25% of the available oxygen is used Deoxygenated blood would retain 75% of its oxygen capacity University of Jordan")
32
32 Rate of Pulmonary and Systemic Gas Exchange Depends on (D p*S *A / M.Wt ) Partial pressures of gases Alveolar P O2 must be higher than blood P O2 for diffusion to occur – problem with increasing altitude Surface area available for gas exchange Diffusion distance Molecular weight and solubility of gases O 2 has a lower molecular weight and should diffuse faster than CO 2 except for its low solubility - when diffusion is slow, hypoxia occurs before hypercapnia University of Jordan
 Partial pressures of gases Alveolar P O2 must be higher than blood P O2 for diffusion to occur – problem with increasing altitude Surface area available for gas exchange Diffusion distance Molecular weight and solubility of gases O 2 has a lower molecular weight and should diffuse faster than CO 2 except for its low solubility - when diffusion is slow, hypoxia occurs before hypercapnia University of Jordan")
33
33 Henry’s law Quantity of a gas that will dissolve in a liquid is proportional to the partial pressures of the gas and its solubility Higher partial pressure of a gas over a liquid and higher solubility, more of the gas will stay in solution Much more CO 2 is dissolved in blood than O 2 because CO 2 is 24 times more soluble Even though the air we breathe is mostly N 2, very little dissolves in blood due to low solubility Decompression sickness (bends) University of Jordan
 University of Jordan")
34
Factors affecting the internal respiration: 1.Partial pressure of gases (diffusion) 2.Distance between the cells and the capillary 3.Rate of metabolic rate: cellular oxidation that leads to formation of CO 2 4.Speed of the blood flow in capillary Internal Respiration
 2.Distance between the cells and the capillary 3.Rate of metabolic rate: cellular oxidation that leads to formation of CO 2 4.Speed of the blood flow in capillary Internal Respiration")
35
Oxygen Diffusion from the Alveoli to the Pulmonary circulation O 2 diffuses into the pulmonary capillaries because the Po 2 in the alveoli is high. Po 2 in the pulmonary capillaries increased very fast (1/3 distance).
..")
36
Transport in arterial blood & Pulmonary shunt flow Due to the bronchial circulation the arterial Po 2 fall to 95 mm Hg

37
Po 2 in systemic circulation (Diffusion from peripheral capillaries) Oxygen is always being used by the cells. Therefore, the intracellular Po 2 in the peripheral tissue cells remains lower than the Po 2 in the peripheral capillaries.

38
Diffusion of CO 2 from the Tissue Cells into the Capillaries

39
Diffusion of CO 2 from the Pulmonary Capillaries into the Alveoli

40
40 Thank You University of Jordan

Similar presentations