Download presentation
Presentation is loading. Please wait.

1
Obesity in Children and Adolescents
A Pediatrician’s Role in Shaping the Future

2
Disclosures We have no financial relations to disclose.

3
Objectives Discuss current epidemiology Review normal growth
Define obesity in childhood Discuss causes Discuss complications What can we do as physicians?

4
According to the CDC in 2015, the percentage of children classified as overweight and obese in the United states is ______. 13% 21% 32% 40% 47%

5
What is the recommended amount of physical activity for children by the American Heart Association?
60 minutes per day, 7 days per week 60 minutes per day, 5 days per week 45 minutes per day, 7 days per week 45 minutes per day, 5 days per week 30 minutes per day, 5 days per week

6
What is the percentage of type 2 diabetes in all new onset diabetes in children?
15% 25% 35% 45% 50%

7
Fasting glucose and lipid panel
Kyle is a 13 year old male presenting to your office for a well child check. His height is at the 85th percentile, his weight is at the 98th percentile, and his BMI is at the 96th percentile. What screening labs should be performed at this visit? Fasting glucose and lipid panel Fasting glucose, lipid panel, AST, and ALT Fasting glucose, lipid panel, AST, ALT, TSH, and Free T4 Fasting glucose, lipid panel, TSH, and Free T4

8
Worldwide Statistics Childhood obesity is one of the most important global health problems of the 21st century. Prevalence increasing at an alarming rate. In 2010, WHO estimated 43 million children < 5 years of age are overweight. It is estimated that by 2020, >60% of global disease burden while be due to obesity related diseases . Primary prevention of pediatric obesity is essential.

9
United States Statistics
Overweight or Obesity BMI-for-age >/= 85th percentile Obesity BMI-for-age >/= 95th percentile All 31.8% 16.9% 2-5 year olds 22.8% 8.4% 6-11 year olds 34.2% 17.7% 12-19 year olds 34.5% 20.5% All Females 2-19 years old 31.6% 17.2% White (non-Hispanic) 29.2% 15.6% Black (non-Hispanic) 36.1% Hispanic 37.0% 20.6% All Males 2-19 years old 32.0% 16.7% 27.8% 12.6% 34.4% 19.9% 40.7% 24.1%
 29.2% 15.6% Black (non-Hispanic) 36.1% Hispanic. 37.0% 20.6% All Males 2-19 years old. 32.0% 16.7% 27.8% 12.6% 34.4% 19.9% 40.7% 24.1%")
10
South Carolina Statistics
17% of adolescents were overweight 14% of adolescents were obese 46% of students grades 9-12 ate fruit or drank 100% fruit juice < 1 time daily 46% of students grades 9-12 consumed vegetables < 1 time daily 78% of adolescents drank a can, bottle, or glass of regular soda during the 7 days prior to the survey 20% of adolescents received < 1 day of 60 minutes of physical activity 33% of adolescents watched 3 or more hours of TV on an average school day

11
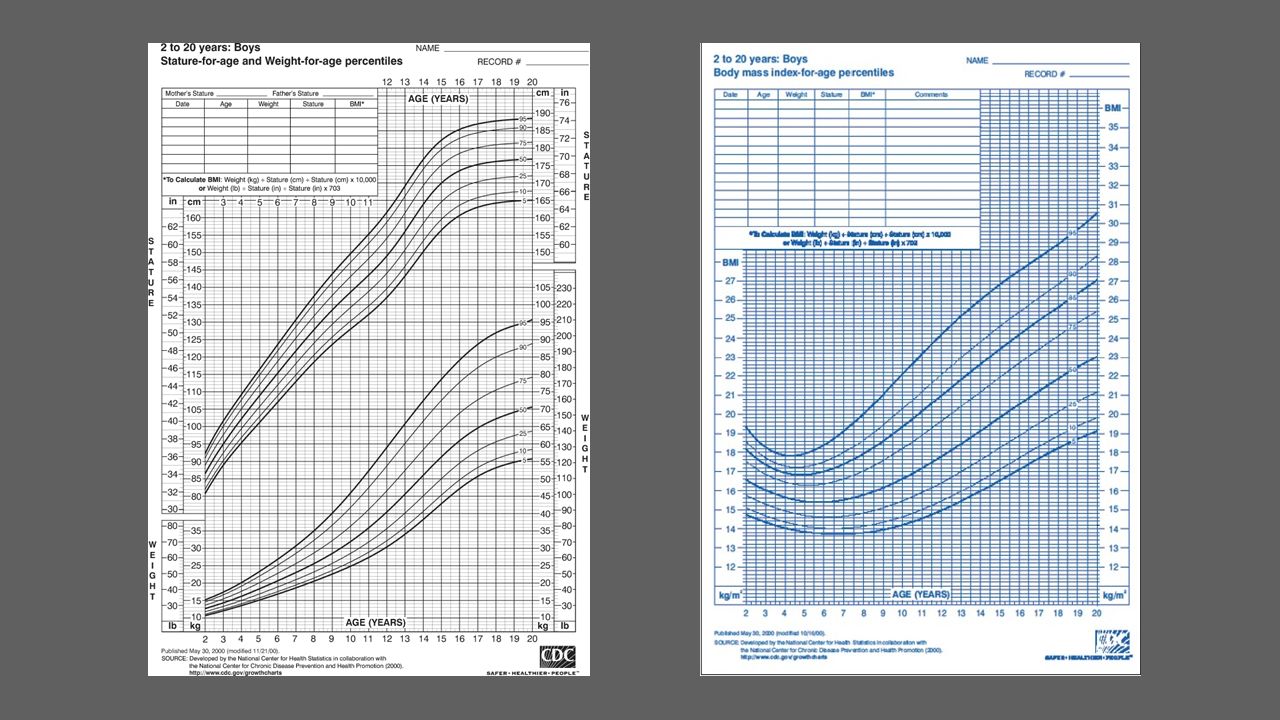
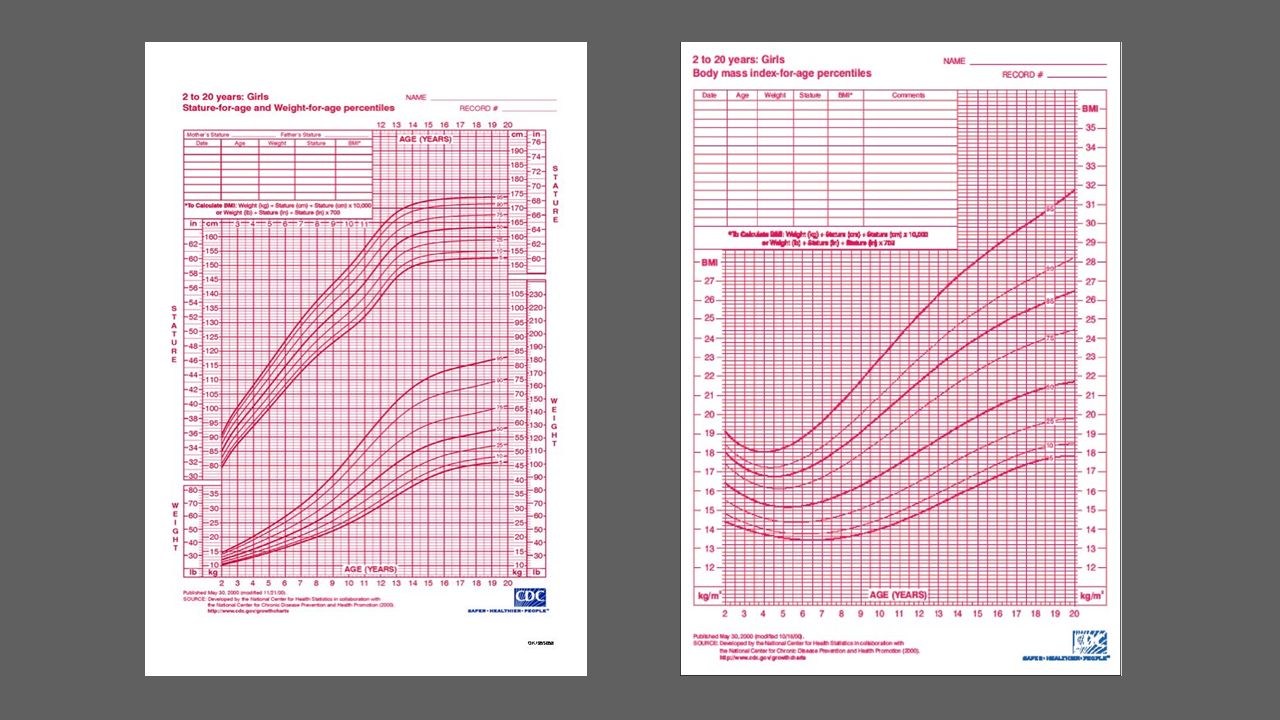
Defining Obesity Excess of body fat CDC 2000 growth charts
Body Mass Index [weight (kg)/ height (m)] 2-18 years of age Obese: BMI at or greater than the 95th percentile of BMI for age Overweight: BMI at the 85th but less than the 95th percentile of BMI for age Less than 2 years of age Overweight: at or greater than the 95th percentile of weight-for-length
/ height (m)] 2-18 years of age. Obese: BMI at or greater than the 95th percentile of BMI for age. Overweight: BMI at the 85th but less than the 95th percentile of BMI for age. Less than 2 years of age. Overweight: at or greater than the 95th percentile of weight-for-length.")
12
Normal Growth Infants typically loss 5-8% of their birth weight in the days following birth Back at birth weight by 2 weeks of age Double birth weight by 6 months Triple birth weight by 12 months Quadruple birth weight by 2 years of age Average weight gain of 2kg/year between 2year of age and puberty

13
Body Fat Proportion of body fat increases rapidly from birth to 12mos
Slow fall occurs until preadolescence Slow rise again until puberty After puberty, percentage stabilizes

14
BMI changes from 2-18 BMI decreases from age 2 years of age to 5-6 years of age and then increase thereafter. V-Shaped Pattern in early childhood has been termed “adiposity rebound”

17
The Cause of Obesity is Multifactorial

18
The Genetic Role Obesity tends to run in families
Risk is 2-8 times greater with a family history of obesity Little is known regarding the specific genes that contribute to obesity What is clear: Genetic factors identified thus far account for only a small portion of obesity risk. Specific Genetic Conditions linked to obesity Bardet-Biedl and Cohen Syndromes Prader Willi

19
>1/3 of kids eat fast food on any given day
FAST Food Consumption >1/3 of kids eat fast food on any given day

20
Soft drink consumption accounts for 1/3 of added sugar in the US diet.
Sugary Beverages Soft drink consumption accounts for 1/3 of added sugar in the US diet.

21
Portion Sizes

22
Activity Level Only 22% of American children meet basic activity level requirements. PE programs in schools are reduced or eliminated Safe places to play outside are limited in some areas Increased screen time

23
Complications

24
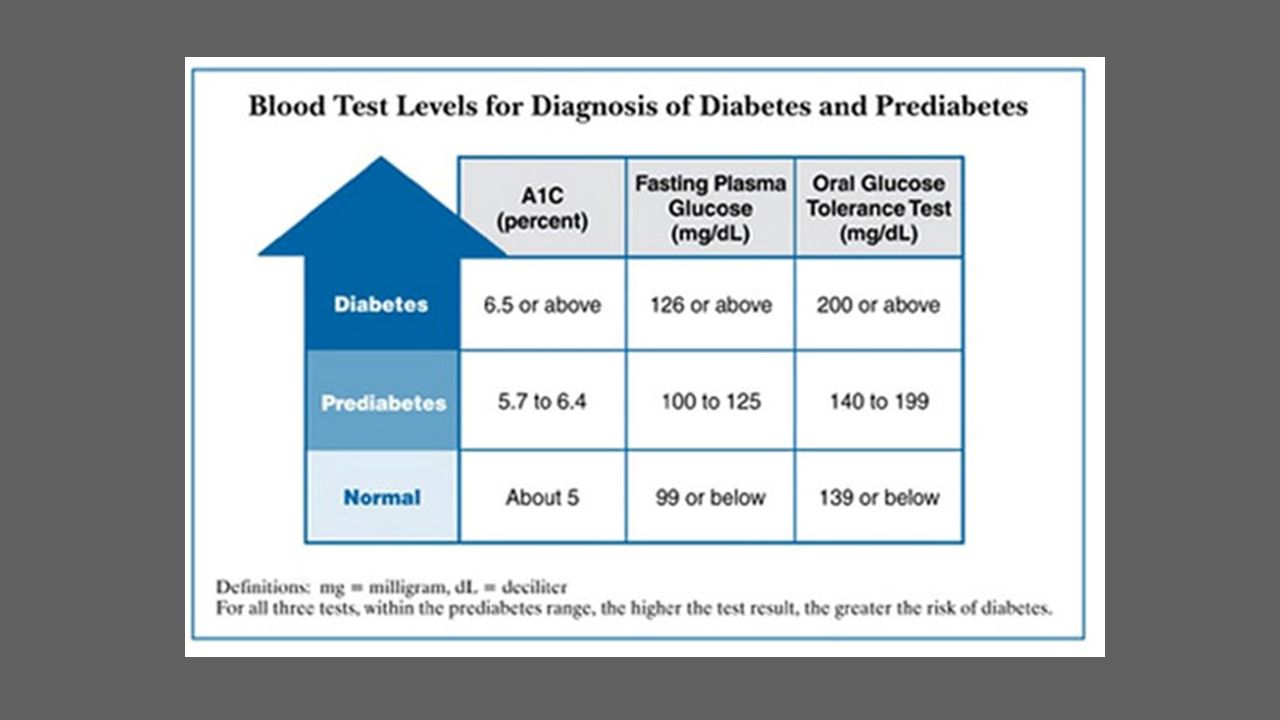
Endocrine Impaired Glucose Tolerance (Pre-Diabetes)
10-30% of children and adolescents have IGT Insulin resistance- increased lipid accumulation and reduced sensitivity of the Beta-cell Majority of this population have normal fasting glucose levels Type 2 Diabetes 45% of all new onset diabetes in adolescents Often occurs in the 2nd decade of life Positive family history in 1st or 2nd degree relative in >75% Biggest risk factor is overweight or obesity

25
Endocrine Hyperandrogenemia Polycystic Ovarian Syndrome
Early puberty in girls

26
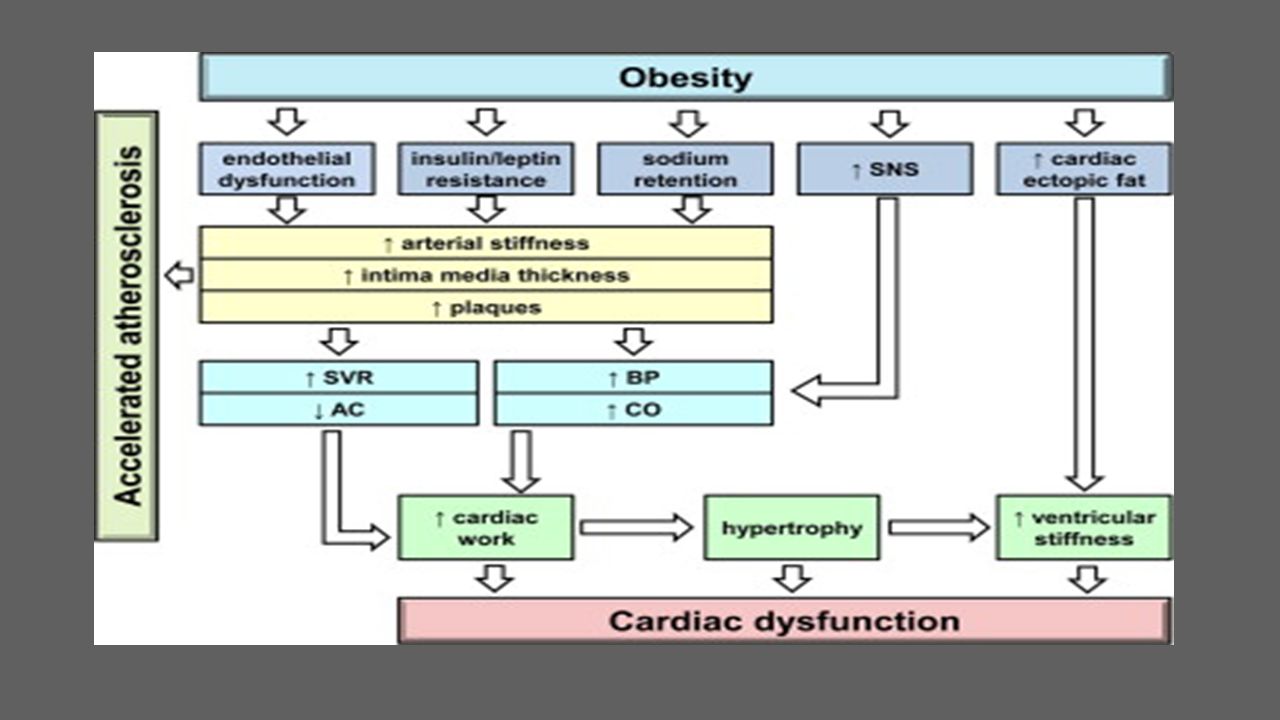
Cardiovascular Hypertension
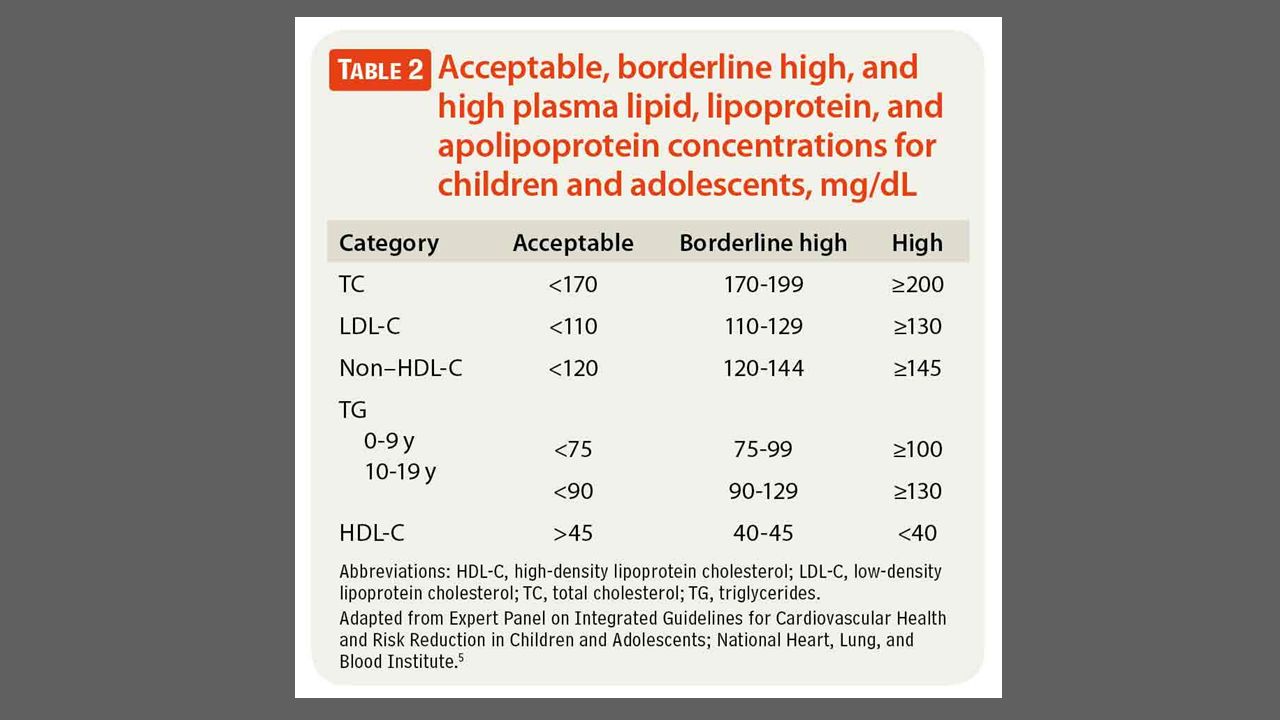
37% of hypertensive children are overweight or obese Dyslipidemia High LDL and Triglycerides, Low HDL Early Development of Atherosclerosis

28
Metabolic Syndrome Type 2 diabetes, hypertension, dyslipidemia, and a prothrombotic inflammatory vascular environment Incidence of 30% in overweight adolescents Increases risk for cardiovascular disease

29
Gastrointestinal NAFLD Most common liver disease in the US
Affects 10% of all children and 38% of obese children Obesity alone and obesity related diseases increase risk Can progress to fibrosis leading to cirrhosis Cholelithiasis

30
Pulmonary Obstructive Sleep Apnea
Occurs in up to 60% of obese children Increases risk of cardiovascular and metabolic syndrome Obesity Hypoventilation Syndrome Asthma

31
Musculoskeletal Higher risk for fractures Early Arthritis
Slipped Capital Femoral Epiphysis Blount’s Disease Pes Planus

32
Other Systems Neuro: Pseudotumor Cerebri
Integumentary: Chronic irritation and infection of skin folds

33
Psychosocial Stress triggering “emotional” eating
Neglect or Maltreatment Living situation lacking consistency, limit-setting, and supervision Food as a reward Food as a part of socializing

34
What can we do as Physicians?

35
Expert Committee Recommendations
Expert committee is comprised of representatives from 15 different professionals organizations First meeting in 1997 Initial recommendations published in 1998 Second meeting in 2007 and revision to initial recommendations published. Serves as a guide for physicians in managing childhood obesity

36
Medical Assessment Identify any underlying syndromes or secondary complications History and Physical

38
History Dietary Assessment Physical Activity Assessment Family History

39
Symptom Possible Causes Anxiety, school avoidance, social isolation Depression Severe recurrent headaches Pseudotumor cerebri Shortness of breath, exercise intolerance Asthma, lack of physical conditioning Snoring, apnea, daytime sleepiness Obstructive sleep apnea, obesity hypoventilation syndrome Sleepiness or wakefulness Abdominal pain Gastroesophageal reflux disease, constipation, gallbladder disease, NAFLDa Hip pain, knee pain, walking pain Slipped capital femoral epiphysis, musculoskeletal stress from weight (may be barrier to physical activity) Foot pain Musculoskeletal stress from weight (may be barrier to physical activity) Irregular menses (<9 cycles per y) Polycystic ovary syndrome; may be normal if recent menarche Primary amenorrhea Polycystic ovary syndrome, Prader-Willi syndrome Polyuria, polydipsia Type 2 diabetes mellitusa Unexpected weight loss Nocturnal enuresis Obstructive sleep apnea Tobacco use Increased cardiovascular risk; may be used as form of weight control
 Foot pain. Musculoskeletal stress from weight (may be barrier to physical activity) Irregular menses (<9 cycles per y) Polycystic ovary syndrome; may be normal if recent menarche. Primary amenorrhea. Polycystic ovary syndrome, Prader-Willi syndrome. Polyuria, polydipsia. Type 2 diabetes mellitusa. Unexpected weight loss. Nocturnal enuresis. Obstructive sleep apnea. Tobacco use. Increased cardiovascular risk; may be used as form of weight control.")
40
Physical Exam Vitals: BP, Weight, Height, BMI General: Body Habitus
Neck: Acanthosis Nigricans, Thyromegaly, Buffalo Hump HEENT: Moon facies, Tonsillar Hypertrophy CV: Murmur Abdomen: Hepatomegaly, RUQ tenderness GU: Early puberty MSK: Bowing of legs, Limited ROM of Hip, Limp Skin: Hirsutism, Excessive Acne, Violaceous Striae I

41
Screening for Obesity Related Conditions
Overweight individuals (BMI of 85th-94th percentile) at age 10 or onset of puberty should have a lipid panel performed and, if risk factors are present, a fasting glucose, AST, and ALT should be performed. Obese individuals (BMI at the 95th percentile or greater at age 10 or onset of puberty should have a lipid panel, fasting glucose, AST, and ALT performed regardless of risk factors The Endocrine Society recommends obese children have a 25-OH vitamin D performed Repeat every 2 years
 at age 10 or onset of puberty should have a lipid panel performed and, if risk factors are present, a fasting glucose, AST, and ALT should be performed. Obese individuals (BMI at the 95th percentile or greater at age 10 or onset of puberty should have a lipid panel, fasting glucose, AST, and ALT performed regardless of risk factors. The Endocrine Society recommends obese children have a 25-OH vitamin D performed. Repeat every 2 years.")
44
Individual based Testing
Tonsillar hypertrophy + snoring, daytime sleepiness Sleep Study OSA? RUQ pain after eating + RUQ tenderness RUQ Abdominal US Cholelithiasis? Knee pain or limp + limited ROM of hip AP and Frog Leg Xrays SCFE?

45
Treatment of Childhood Obesity
Behavior Changes!

46
Counseling Use sensitivity and compassion
Obesity is an important medical condition that can be treated Ask questions in an objective, non-accusatory fashion Try to avoid words that may have a negative connotation

47
Motivational Interviewing
Patient-centered method for enhancing intrinsic motivation to change health behavior by exploring and resolving ambivalence. Elicit-Provide-Elicit Importance and Confidence Scale Positive results in health behavior and weight loss Reduces physician stress and frustration in obesity counseling Increases odds of success!

48
Ineffective Communication
Doctor: We need to talk about John’s weight and diet. His BMI percentile classifies him as obese. You state that he eats little to no vegetables or fruit and that his diet consists of mainly hot dogs, chicken nuggets, fries, and juice. You should increase the vegetables and fruit that John eats and reduce the high calorie, processed foods in his diet. John should also only drink 4-6oz of juice per day. Mother: Well I am a single mother that works a full time job. Fresh fruits and vegetables are more expensive and take more time to prepare. For our lifestyle, his current diet is more feasible.

49
Effective Communication
Doctor: Would it be okay if we discussed John’s diet and weight today? Mother: I guess so. Doctor: The diet of many young kids today consists of a large amount of processed foods such as hot dogs, chicken nuggets, and fries. These foods are high in calories and low in nutritional value which can cause children to be overweight and deficient in vitamins and minerals. They also contain a large amount of salt that isn’t good for the heart. Most children drink more juice than recommended. We recommend no more than 4-6oz of juice per day because it contains a large amount of sugar and calories. How do feel about the information I’ve provided? Mother: Well after hearing all of that information and when I look closer at John’s diet, maybe we do need to make some changes.

50
Doctor: On a scale of 1-10, with 10 being the highest, how important is making a change in John’s diet to you? Mother: I guess I’d say an 8. Doctor: Using this same scale, how confident are you that you can make these changes? Mother: I think an 8. Doctor: Great! Well let’s talk about the changes you would like to make and the strategies you can use to achieve those changes.

51
4 stages of Treatment Stage 1: Prevention Plus
Stage 2: Structured Weight Management Stage 3: Comprehensive Multidisciplinary Intervention Stage 4: Tertiary Care Intervention

52
Additional Tips for Counseling
Make 1 change at a time. Encourage parents not to expect children to make healthy choices on their own. Food should not be used as a reward. Encourage positive behavior changes for the entire family. Emphasize health not weight.

53
Summary Childhood obesity can be a difficult and frustrating disease to treat. Every child should be screened for obesity and risk factors for obesity and obesity-related disorders. Counsel on preventive measures at every visit. Primary prevention is key!

54
According to the CDC in 2015, the percentage of children classified as overweight and obese in the United states is ______. 13% 21% 32% 40% 47%

55
What is the recommended amount of physical activity for children by the American Heart Association?
60 minutes per day, 7 days per week 60 minutes per day, 5 days per week 45 minutes per day, 7 days per week 45 minutes per day, 5 days per week 30 minutes per day, 5 days per week

56
What is the percentage of type 2 diabetes in all new onset diabetes in children?
15% 25% 35% 45% 50%

57
Fasting glucose and lipid panel
Kyle is a 13 year old male presenting to your office for a well child check. His height is at the 85th percentile, his weight is at the 98th percentile, and his BMI is at the 96th percentile. What screening labs should be performed at this visit? Fasting glucose and lipid panel Fasting glucose, lipid panel, AST, and ALT Fasting glucose, lipid panel, AST, ALT, TSH, and Free T4 Fasting glucose, lipid panel, TSH, and Free T4

58
Resources Herouvi, Despina, Evangelos Karanasios, Christina Karayianni, and Kyriaki Karavanaki. "Cardiovascular disease in childhood: the role of obesity." European Journal Pediatrics 172 (2013): PubMed. Web. 3 Jan. 2016 McCrindle, Brian W. "Cardiovascular Complications of Childhood Obesity." Canadian Cardiovascular Society 31.2 (2014): PubMed. Web. 3 Jan Indra Narang and Jospeh L. Mathew, “Childhood Obesity and Obstructive Sleep Apnea,” Journal of Nutrition and Metabolism, vol. 2012, Article ID , 8 pages, doi: /2012/134202 Andrew J. Walley, Alexandra I.F. Blakemore, and Philippe Froguel. Genetics of obesity and the prediction of risk for health. Hum. Mol. Genet. (2006) 15 (suppl 2): R124-R130 doi: /hmg/ddl21 Burt Solorzano, Christine M., and Christopher R. McCartney. “Obesity and the Pubertal Transition in Girls and Boys.” Reproduction (Cambridge, England)140.3 (2010): 399–410. PMC. Web. 6 Jan Schuman, Andrew J. "Making a Difference: Point of care screening for hyperlipidemia." Contemporary Pediatrics (2013). Web. 9 Jan. 2016 Kelishadi, Roya, and Fatemeh Azizi-Soleiman. "Controlling Childhood Obesity: A Systematic Review on Strategies and Challenges." Journal of Research in Medical Sciences (2014): PubMed. Web. 14 Jan. 2016 Krebs, Nancy F., and John H. Himes. "Assessment of Child and Adolescent Overweight and Obesity." Journal of Research in Medical Sciences (2007): PubMed. Web. 14 Jan Vikraman, Sundeep, and Cheryl Fryar. "Caloric Intake From Fast Food Among Children and Adolescents in the United States, " CDC. N.p., Sept Web. 14 Jan Golden, Neville H., and Steven A. Abrams. "Optimizing Bone Health in Children and Adolescents." Pediatrics 134.4 (2014). Web. 14 Jan
: PubMed. Web. 3 Jan McCrindle, Brian W. Cardiovascular Complications of Childhood Obesity. Canadian Cardiovascular Society 31.2 (2014): PubMed. Web. 3 Jan Indra Narang and Jospeh L. Mathew, Childhood Obesity and Obstructive Sleep Apnea, Journal of Nutrition and Metabolism, vol. 2012, Article ID , 8 pages, doi: /2012/ Andrew J. Walley, Alexandra I.F. Blakemore, and Philippe Froguel. Genetics of obesity and the prediction of risk for health. Hum. Mol. Genet. (2006) 15 (suppl 2): R124-R130 doi: /hmg/ddl21. Burt Solorzano, Christine M., and Christopher R. McCartney. Obesity and the Pubertal Transition in Girls and Boys. Reproduction (Cambridge, England)140.3 (2010): 399–410. PMC. Web. 6 Jan Schuman, Andrew J. Making a Difference: Point of care screening for hyperlipidemia. Contemporary Pediatrics (2013). Web. 9 Jan Kelishadi, Roya, and Fatemeh Azizi-Soleiman. Controlling Childhood Obesity: A Systematic Review on Strategies and Challenges. Journal of Research in Medical Sciences (2014): PubMed. Web. 14 Jan Krebs, Nancy F., and John H. Himes. Assessment of Child and Adolescent Overweight and Obesity. Journal of Research in Medical Sciences (2007): PubMed. Web. 14 Jan Vikraman, Sundeep, and Cheryl Fryar. Caloric Intake From Fast Food Among Children and Adolescents in the United States, CDC. N.p., Sept Web. 14 Jan Golden, Neville H., and Steven A. Abrams. Optimizing Bone Health in Children and Adolescents. Pediatrics (2014). Web. 14 Jan")
59
Resources Barlow, Sarah E. "Expert Committee Recommendations Regarding Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report." Pediatrics 120 (2015): Web. 14 Jan. 2016 Barlow, Sarah E., and William H. Dietz. "Obesity Evaluation and Treatment: Expert Committee Recommendations." Pediatrics102 (1998). Web. 14 Jan file:///C:/Users/Rebecca/Downloads/ObesityMgmt-PocketGuide%20(1).pdf
: Web. 14 Jan Barlow, Sarah E., and William H. Dietz. Obesity Evaluation and Treatment: Expert Committee Recommendations. Pediatrics102 (1998). Web. 14 Jan topic=A file:///C:/Users/Rebecca/Downloads/ObesityMgmt-PocketGuide%20(1).pdf.")
60
Thank You!

Similar presentations













 is a measure used to determine childhood overweight.>")






