Download presentation
Presentation is loading. Please wait.

1
GROUP 09 MATERNAL AND CHILD HEALTH PRESENTATION TOPIC: ANTI SHOCK GARMENT JANUARY 2014.

2
Members OYEKANMI oladunjoye Nsc/08/236 WAHAB Gafar Nsc/08/250 AWOTUNDE Seye Nsc/08/147 OPARA Nora Nsc 08/226 ONI Catherine Nsc/08/ KUSE Abigael Nsc/08 AKILO Bolanle Nsc/08/ OWODUNNI Iranlowo Nsc/08/ OLAWOYIN Adenike Nsc/07/

3
Anti-shock Garment is a low- technology first-aid device used to treat hypovolemic shock. It has been shown to be efficient in reducing maternal deaths due to Obstetrical hemorrhage

4
Obstetrical heamorrhage is a condition in which a woman bleeds heavily, most often after giving birth Anti-shock garment works to decrease blood loss, recovers them from shock and keeps them alive until adequate treatment arrives

5
background Current estimate suggests over 300,000 women die every year, 99 percent of which occurs in developing countries due to complication during pregnancy and child birth. Complication at birth can be serious, lifelong ailments which compromise a woman's health, productivity, quality of life, family health and ability to participate in community life. If a mother dies after childbirth, the newborn is ten times more likely to die before the age of two, other children are more likely to suffer from decreased nutrition and decreased schooling.

6
Once Heamorrhage has been identified, many women die before reaching or receiving adequate treatment. The Anti-shock Garment can be used to keep women alive until they can get the treatment they need.

7
In the 1900s an inflatable pressure suit was developed by George Crile. It was used to maintain blood pressure during surgery In the 1940s and 1970s, after several modifications, it was used by the military for resuscitating and stabilizing soldiers with traumatic injuries before and during transportation.

8
In the 1900s an inflatable pressure suit was developed by George Crile. It was used to maintain blood pressure during surgery In the 1940s and 1970s, after several modifications, it was used by the military for resuscitating and stabilizing soldiers with traumatic injuries before and during transportation.

9
The use of anti-shock garment for obstetrical heamorrhage began in 2002 when Dr. Carol Brees and Dr. Paul Hensleigh introduced the garment into a hospital in Pakistan. There are reports of its use in various places An implementation program with the NASG as part of a Continuum of Care for Post-Partum Heamorrhage (CCPPH) has been underway since 2008 in India, Peru and Nigeria.
 has been underway since 2008 in India, Peru and Nigeria..")
10
Types of Anti-Shock Garment. Pneumatic Anti Shock Garment (PASG). Non- Pneumatic Anti Shock Garment (NASG).
..")
11
Pneumatic AntiShock Garment

13
PASG Did not make statistically significant difference in mortality and morbidity for lower body trauma patients. Use of PASG for obstetrical hemorrhage: ONLY 6 cases reported NO comparative trials

14
NON-PNEUMATIC ANTI SHOCK GARMENT. DESCRIPTION: a first aid device. made from neoprene (strechable with recoil property). in form of a trouser. has Velcro fastener. Light weight and reusable.
. in form of a trouser. has Velcro fastener. Light weight and reusable..")
15
Figure 1 Schematic diagram of the non-pneumatic anti-shock garment

16
Figure 2: NASG - Non-pneumatic Anti-shock Garment picture.

17
Clinical signs of Shock. Fast and /or weak pulse >100 beats/minute. Low BP less than 100mmHg systolic. Pallor, sweating, cold skin. Rapid breathing. Anxious and confused. Unconsciousness. Urine output less than 30mls/hour.

18
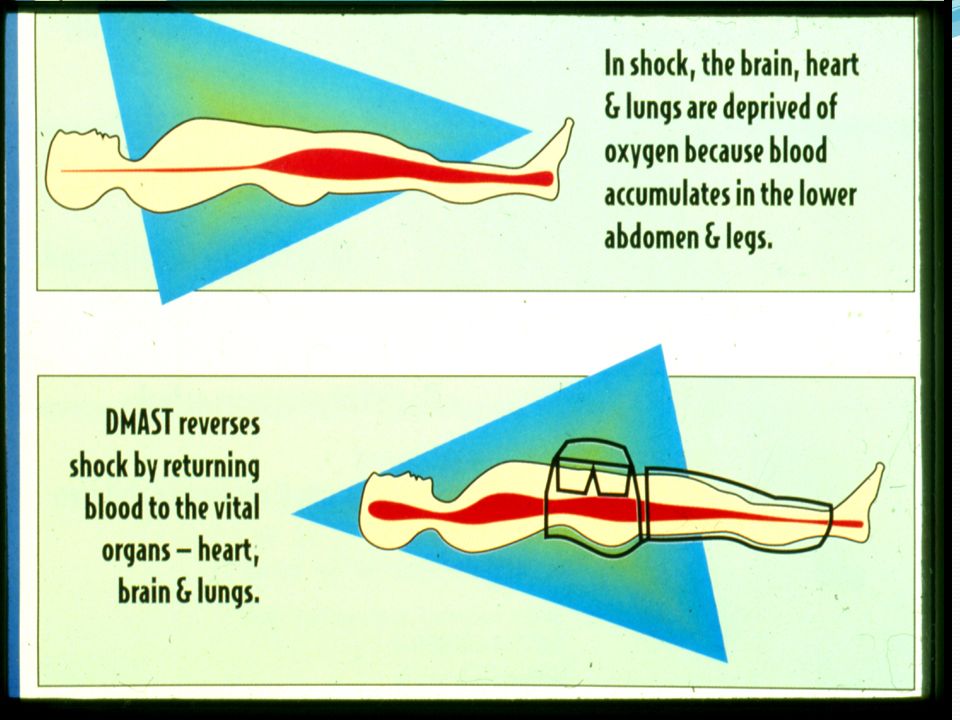
How Anti-Shock Garment Works

19
When in shock, the brain, heart and lungs are deprived of oxygen because blood accumulates in the lower abdomens and legs. The anti-shock garment reverses shock by decreasing blood flow by applying direct counter pressure (30 to 50mmHg) to the lower body parts thus, returning blood to the heart, brain and lungs. Research has shown that the Anti- shock garment serves to significantly increase the resistive index of the internal iliac artery (which supplies blood to uterus via the uterine arteries) and as well decreases blood flow in the distal aorta. It also causes uterus to contract and decreases blood flow.
 to the lower body parts thus, returning blood to the heart, brain and lungs. Research has shown that the Anti- shock garment serves to significantly increase the resistive index of the internal iliac artery (which supplies blood to uterus via the uterine arteries) and as well decreases blood flow in the distal aorta. It also causes uterus to contract and decreases blood flow..")
21
The non-pneumatic anti-shock garment is light, flexible and comfortable to wear. It is designed to allow perineal access so that examinations and vaginal procedures can be performed without it being removed. Upon application, a patient’s vital signs are restored and consciousness regained. It must not be removed before a woman receives IV fluids, blood and before all vital signs are restored.

22
Stabilizes patient while evaluating, transporting, or preparing for definitive surgical treatment. Shunts blood to vital organs. Can be safely and comfortably used up to 48 hours. During delays, provides up to 48 hours stability May arrest bleeding and avoid surgical intervention. May decrease need for number of blood transfusions

23
Permits complete perineal access so that genital lacerations can be repaired. Speculum or bimanual examinations, manual removal of placenta, manual vacuum aspiration or curettage can all be accomplished with the NASG in place.

24
Uses/prospects ctd. May arrest bleeding and avoid surgical intervention. May decrease need for or number of blood transfusions. Reduces further blood loss. Protects haemophiliac children from bleeding into elbow and knee joints by straightening and compressing the joint until medical attention is available. (Coelius et al. 2010).
..")
25
Mechanism of Action. Reduces Haemorrhage. Counteracts shock and decreases blood flow by applying direct counter pressure (30 to 50mmHg) to the lower parts of the body. causes the uterus to contract and decrease blood flow. Decreases arterial pressure to the uterus, comparable to ligation of the internal iliac arteries.
 to the lower parts of the body. causes the uterus to contract and decrease blood flow. Decreases arterial pressure to the uterus, comparable to ligation of the internal iliac arteries..")
26
Mechanism of Action. Resuscitation of central circulation. Result in translocation of up to 30% (1.5 to 2 L) of total blood volume from lower body to the core (vital organs). Reverses shock (anti shock).
 of total blood volume from lower body to the core (vital organs). Reverses shock (anti shock)..")
27
Figure 4: a practical section on NASG application (fully applied).
.")
28
NASG Obstetric Hemorrhage

29
What NASG Does NOT DO Does not avert the necessity for evaluation to identify cause of shock to manage fluid and blood replacement to provide appropriate therapy for coagulopathy

30
INDICATIONS. BEFORE DELIVERY. Ectopic pregnancy. Abruption. Placenta praevia. Ruptured uterus. Hydatidiform mole. Spontaneous abortion.

31
INDICATIONS ctd. AFTER DELIVERY. Atony. Retained products of conception. Obstetrical trauma. NOTE: NASG is not a treatment. It is an obstetric first aid.

32
CONTRADICTIONS. Mitral stenosis. Viable fetus in-utero. Rupture of (or bleeding above) the diaphragm. Pulmonary oedema. Congestive Heart Failure. Open thoracic wounds.
 the diaphragm. Pulmonary oedema. Congestive Heart Failure. Open thoracic wounds..")
33
UNITS WHERE NASG ARE USED. NASG are used where bleeding patients are first seen e.g. Accident and Emergency Unit. Labour Ward. Theatre. Ante natal Clinic.

34
Advantages. It is less expensive. It can be easily and quickly applied. Application requires about 2 minutes. Can be used by persons with minimal training Within 2-5 minutes of application most patients with severe shock regain consciousness and vital signs begin to stabilize The Non Pneumatic Garment is less expensive and simpler than predecessors It also has less danger of excessive pressures due to over- inflation.

35
Advantages ctd. Limits prolonged hospitalization. Prevents/decreases further obstetric complications. Enhances quality care in emergencies. NASG to decreases blood loss, reverses shock, and stabilize women for many hours while awaiting blood transfusions. As such, use of the NASG might contribute to decreased maternal mortality and morbidity. (Coelius et al. 2010).
..")
36
Procedure for application of NASG. For any level of facility or provider: 1. General application. 2. Application for shorter women. 3. Application if the woman is unconscious. SEGMENT 1: Just above the ankle. ‘’ 2: Just below the knee. ‘’ 3: Thigh. ‘’ 4: Pelvis. ‘’ 5 &6: On the abdomen, just below the diaphragm.

38
1. General application. Step 1: Open the NASG after wearing glove. Place it under the woman, the top of the NASG should be at the level of her lowest rib. Start at the ankles, close segment tightly around each ankle. Make sure it is tight enough so that you can snap it and hear a sharp sound.

39
1. General application ctd. Step 2: Close segment 2 tightly as possible. Try to leave the woman’s knee free (in space between segments) so that she can bend her leg. She may be in the NASG for a long time) Step 3: Apply segment 3, the thigh segments in the same way as segments 1 and 2. Remember: close segments tightly enough so that you can snap it and hear a sharp sound.
 so that she can bend her leg. She may be in the NASG for a long time) Step 3: Apply segment 3, the thigh segments in the same way as segments 1 and 2. Remember: close segments tightly enough so that you can snap it and hear a sharp sound..")
40
1. General application ctd. Step 4: Segment 4, the pelvic segment goes all the way around the woman, the lower edge at the level of the pubic bone. Step 5: Place segment 5 with the pressure ball directly over her umbilicus. Close the NASG using segment 6. do not close the segment so tightly that it restricts the woman’s breathing.

41
1. General application ctd. When finished: Make sure the patient can breath normally with the NASG segment 6 in place. If the source of bleeding appears to be uterine atony, administer uterotonic drugs and massage the uterus. The NASG stretches, allowing room for your massaging hand.

42
2. Application for short women. If the small garment is not available. Step 1: Fold segment 1 to the inside of segment 2. Begin segment 2 at her ankles. Apply segment 3 to the thighs as usual. Continue with the rest of the segments as usual.

43
3. Application if the woman is unconscious. You will need 2 people. Step 1: Fold the NASG in half along the dotted line. Then, turn the woman on her side with her back facing you and place the dotted line along the woman’s spine. Push the flat half of the abdominal and pelvic sections under her body. The principle is the same as that of making a patient-occupied bed.

44
3. Application if the woman is unconscious. Step 2: Roll her back towards you, turning her to her other side, spreading the NASG under her. Then, have the second person helping pull the flat half of the abdominal and pelvic sections out from under the woman. Step 3: Finally, close the NASG, starting at her ankles. Continue with the rest of the segments as with all women.

45
NOTE. It should be applied by a single person to prevent too much pressure. With proper monitoring, NASG can be safely and comfortably used for 24 – 48 hours. The use of NASG does not avert the necessity for evaluation to identify cause of shock, management of fluid and blood replacement and appropriate therapy for coagulopathy.

46
Figure 5: NASG being applied.

47
Figure 6: NASG fully applied.

48
Figure 7;NASG fully applied in a non obstetric condition

49
WHEN TO REMOVE THE NASG. When the woman’s condition is stable. Bleeding has stopped < 50mls/ hour. Haemoglobin level is >7 or the heamatocrit 20% The woman is conscious and aware. Use the rule of 100 to start removal. Use the rule of 20 for in between removal.

50
WHEN TO REMOVE THE NASG CTD. RULE OF 100 : Tells when to start removing. Systolic pressure above 100 Pulse rate below 100 RULE OF 20 : For in between removal. If between removal of segment, there is a decrease in BP of 20mmHg OR increase in pulse rate of 20b/m. The patient is not stable, hence, re-apply.

51
REMOVAL PROCEDURE. Use the Rule of 100. Remove segment 1 : wait for 15 minutes & re-check vital signs. If stable (using the rule of 20) Remove segment 2 & wait for 15 minutes. Re-check the vital signs (rule of 20). Remove segment 3 e.t.c.
 Remove segment 2 & wait for 15 minutes. Re-check the vital signs (rule of 20). Remove segment 3 e.t.c..")
52
NOTE. WHY WAITING FOR 15 MINUTES? This is because the time it takes for re-distribution for the equilibrium to take place will take about 15 minutes for stabilization. The largest portion of capacitance vessels are in the abdominal cavity rather than the legs, hence, segments 5 and 6 should never be removed first to prevent rapid redistribution of blood which may return the patient to shock state.

53
CLEANING OF THE NASG. 1 st Bowl - Jik Solution (1:6) : 3 L Jik into 18 L of water. 2 nd Bowl - Detergent. 3 rd Bowl - Clean water.

54
PROCEDURE. Wear elbow lenght glove. If very bloody, take to running water and wash away the blood. soak the garment for 10 minutes in the jik solution to kill the virus. (just 10 minutes so that it does not destroy the garment.

55
PROCEDURE CONT. Remove into the detergent, use brush to remove the blood stain. Rinse in clean water (3 rd Bowl). Dry. Fold back properly.
. Dry. Fold back properly..")
56
PROCEDURE CONT. Store in an agreed designated place, accessible to all. Not locked up, place where bleeding patients are first seen e.g. A & E, Labour ward, Theatre. With careful care of the garment, it can be used for up to 50 to 100 times.

58
Challenges. Institutional capacity (tested in tertiary centers) NASG is first aid - not definitive treatment Facilities must be able to provide Oxygen Normal Saline Blood Uterotonics and other medicines Surgery/anesthesia
 NASG is first aid - not definitive treatment Facilities must be able to provide Oxygen Normal Saline Blood Uterotonics and other medicines Surgery/anesthesia.")
59
Conclusion. Most women die of haemorrhage due to DELAYS in restoring the circulatory volume through timely and adequate blood/fluid replacement. NASG is a DEVICE that can save our women’s lives during these DELAYS by shunting 2-3 units of blood to the vital organs such as heart, kidneys and the brain. (Pathfinder International, 2010) PPH is treatable if the woman has access to trained healthcare workers at a well-equipped health facility.
 PPH is treatable if the woman has access to trained healthcare workers at a well-equipped health facility..")
60
Promote Change!!!

61
References. Adesokan F.O.(2010). Reproductive Health for All Ages, Faxwell Nigeria Ltd. Ado- Ekiti. Anderson JM, Etches D (March 2007). "Prevention and management of postpartum haemorrhage". American Family Physician 75 (6): 875–82. PMID 17390600. Brees C, Hensleigh PA, Miller S, Pelligra R. (2004). A non-inflatable anti shock garment for obstetric hemorrhage. Int J Gynaecol Obstet, 87 (2), 119-124, 2004. Coelius, R, Stenson, A, Morris, J, Cuomu, M, Tudor, C, Miller, S. The Tibetan Uterotonic Zhi Byed 11: Mechanisms of Action, Efficacy, and Historical Use for Post-Partum Hemorrhage. Evid Based Complement Alternat Med, vol 2012 article ID 794164,: 2011, 10.1155/2012/794164
. Prevention and management of postpartum haemorrhage . American Family Physician 75 (6): 875–82. PMID Brees C, Hensleigh PA, Miller S, Pelligra R. (2004). A non-inflatable anti shock garment for obstetric hemorrhage. Int J Gynaecol Obstet, 87 (2), , Coelius, R, Stenson, A, Morris, J, Cuomu, M, Tudor, C, Miller, S. The Tibetan Uterotonic Zhi Byed 11: Mechanisms of Action, Efficacy, and Historical Use for Post-Partum Hemorrhage. Evid Based Complement Alternat Med, vol 2012 article ID ,: 2011, /2012/")
62
References ctd. Diane M.F. % Margaret A.C. (2009). Myles Textbook for Midwives, Fifteen Edition. Churchil Livingstone, Toronto. pg 544-552. Miller, S., Turan, JM, Ojengbede A, Ojengbede, O, Fathalla, M, Morhason-Bello, IO, Mourad, M, Galandanci, H, Hamza, S, Awaal, M, Akinwuntan, A, Mohammed AI, McDonough, L, Dau, K, Butrick, E, and Hensleigh, P. The Pilot Study of the Non- pneumatic Anti-Shock Garment (NASG) in Women with Severe Obstetric Hemorrhage: Combined Results from Egypt and Nigeria. Int J Gynaecol Obstet, 94(S3), ps43-s44. 2006
 in Women with Severe Obstetric Hemorrhage: Combined Results from Egypt and Nigeria. Int J Gynaecol Obstet, 94(S3), ps43-s")
63
References ctd. Miller, S, Hamza, S, Bray E, Gipson R, Nada, K, Fathalla, M, Mourad, M. et al. First Aid for Obstetrical Hemorrhage: The Pilot Study of the Non-pneumatic Anti-Shock Garment (NASG) in Egypt. British Journal of Obstet Gynaecol, 113(4): p. 424-9, 2006. Miller, S., Turan, JM, Ojengbede A, Ojengbede, O, Fathalla, M, Morhason-Bello, IO, Mourad, M, Galandanci, H, Hamza, S, Awaal, M, Akinwuntan, A, Mohammed AI, McDonough, L, Dau, K, Butrick, E, and Hensleigh, P. The Pilot Study of the Non-pneumatic Anti-Shock Garment (NASG) in Women with Severe Obstetric Hemorrhage: Combined Results from Egypt and Nigeria. Int J Gynaecol Obstet, 94(S3), ps43-s44. 2006
 in Egypt. British Journal of Obstet Gynaecol, 113(4): p , Miller, S., Turan, JM, Ojengbede A, Ojengbede, O, Fathalla, M, Morhason-Bello, IO, Mourad, M, Galandanci, H, Hamza, S, Awaal, M, Akinwuntan, A, Mohammed AI, McDonough, L, Dau, K, Butrick, E, and Hensleigh, P. The Pilot Study of the Non-pneumatic Anti-Shock Garment (NASG) in Women with Severe Obstetric Hemorrhage: Combined Results from Egypt and Nigeria. Int J Gynaecol Obstet, 94(S3), ps43-s")
64
References ctd. Miller, S, Ojengbede A, Turan J, Ojengbede O, Butrick E, Hensleigh, P. Anti-Shock Garments for Obstetric Hemorrhage. Current Women’s Health Reviews, 3(1), 3-11, 2006. Miller, S, Turan, JM, Dau, K, Fathalla M, Mourad M, Sutherland, T, Hamza, S. et al. Decreasing Maternal Mortality from Hypovolemic Shock in Low Resource Settings: the Non-pneumatic Anti-Shock Garment (NASG). Global Public Health Journal, 2(2);110-24, 2006.
, 3-11, Miller, S, Turan, JM, Dau, K, Fathalla M, Mourad M, Sutherland, T, Hamza, S. et al. Decreasing Maternal Mortality from Hypovolemic Shock in Low Resource Settings: the Non-pneumatic Anti-Shock Garment (NASG). Global Public Health Journal, 2(2);110-24,")
65
References ctd. Miller, S, Turan, JM, Dau, K, Fathalla M, Mourad M, Sutherland, T, Hamza, S. et al. Decreasing Maternal Mortality from Hypovolemic Shock in Low Resource Settings: the Non-pneumatic Anti Shock Garment (NASG). Global Public Health Journal, 2(2);110-24, 2006. Pathfinder International (2010), A Continum of Care addressing Postpartum Haemorrhage in India and Nigeria Trainer’s guide.
. Global Public Health Journal, 2(2);110-24, Pathfinder International (2010), A Continum of Care addressing Postpartum Haemorrhage in India and Nigeria Trainer’s guide..")
66
THANK YOU.

Similar presentations











 Dr. Abdelhadi Eltahir, MD, MPH, Senior Advisor for Maternal and Newborn Health,>")










