Download presentation
Presentation is loading. Please wait.

1
Anatomy & Physiology I Chapter 11
The Senses Anatomy & Physiology I Chapter 11

2
The Senses Protect a person by detecting changes in the environment
Stimulus – an environmental change that initiates or stimulate a nerve impulse Sensation – when a specialized area of the cerebral cortex interprets the nerve impulse and the stimulus then becomes something we experience Environmental change >> stimulus >> threshold stimulus >> sensory receptors >> sensory neuron>> CNS >> interpretation>> sensation (what we experience or sense) Threshold stimulus - minimum amount of stimulus required to generate a nerve impulse
 Threshold stimulus - minimum amount of stimulus required to generate a nerve impulse.")
3
Sensory Receptors – Types based on Structure
Free dendrite of a sensory neuron; Example, pain, temperature End-organ - the modified dendrite ending of a sensory neuron enclosed in a capsule -Pacinian & Meissner corpuscles for pressure & touch receptors Specialized cell associated with an afferent neuron (afferent/ascending/to the CNS); rods & cones in the eye
; rods & cones in the eye.")
4
Sensory Receptors

5
Sensory Receptors – Types based on Stimulus
Chemoreceptors – detect chemicals in solution; taste & smell Photoreceptors – respond to light; eye retina Thermoreceptors – detect temperature change; skin Mechanoreceptors – respond to movement, vibration, pressure, stretch; located in skin, joints (monitor body position), hearing & equilibrium in ear
, hearing & equilibrium in ear.")
6
Types of senses based on the distribution of their receptors
Special senses; sensory receptors localized in a special sense organ Vision Hearing Equilibrium Taste Smell General senses; sensory receptors widely distributed throughout the body Pressure Temperature Pain Touch Position

7
The Eye - Protective Structures
Skull bones form walls of eye orbit; over half of posterior eye Upper & lower eyelids; anterior eye Eyelashes & eyebrows; anterior eye Conjunctiva; lines inner surface of eyelids & covers the visible portion of the white of the eye (sclera); produces mucus & is highly vascular Lacrimal glands; produce tears which lubricate & produce enzyme that protects against infection Flow from superior lateral eye into inferior medial nasolacrimal duct
; produces mucus & is highly vascular. Lacrimal glands; produce tears which lubricate & produce enzyme that protects against infection. Flow from superior lateral eye into inferior medial nasolacrimal duct.")
8
Lacrimal Gland & Conjunctiva

9
Coats of the Eyeball 3 tunics (coats)
Sclera – outermost tunic made of tough connective tissue; white of the eye because made of collagen & no blood vessels Choroid – coat made of delicate connective tissue; extensive blood supply which are visualized during eye exam; prevents light from scattering throughout eye Retina – actual receptor layer; contains rods & cones which generate visual nerve impulses

11
What are some structures that protect the eye?
What are the names of the tunics of the eyeball?

12
Pathway of Light Rays & Refraction
Refraction – bending of light rays as they pass from one substance to another substance of a different density Allows light from a very large area to be focused on a very small area of the retina Cornea Aqueous humor Lens Vitreous body

13
Light Refraction in the Eye
Cornea – transparent, colorless continuation of sclera that covers the pupil; the window of the eye Aqueous humor – watery fluid that fills the eye anterior to the lens; aids in refraction & maintains eye shape Lens – clear circular structure with biconcave surface made of firm, elastic material; can change in thickness & focus near or far Vitreous body – soft gel that fills entire space posterior to the lens; aids in refraction & maintains eye shape

14
Layers of the Retina Pigmented layer – deepest layer just anterior to choroid Rods & cones – receptors of the eye Connecting neurons that carry impulses toward the optic nerve

15
Rods Rods – highly sensitive to light
function in dim light but do not provide sharp image Dark adaptation; the time it takes for rods to begin working in a darkened area 120 million each retina Distributed towards the periphery of the retina See shades of gray; no colors Rhodopsin – visual purple pigment that is sensitive to light; requires vitamin A; lack of this pigment leads to night blindness

16
Cones Cones – sensitive to color Function only in bright light
6 million per retina Localized in center of retina fovea centralis, pit near the optic nerve; area of greatest visual acuity surrounded by the macula lutea Optic disk; point where the optic nerve arises in the retina; no rods or cones in this area; blind spot on the retina Sees sharp images Pigments sensitive to red, green, blue Hereditary lack of pigment can lead to colorblindness in males

17
Macula lutea (yellowish)
Fovea & Macula lutea Fovea (dark pink) & Macula lutea (yellowish)
 & Macula lutea (yellowish)")
18
Visual Impulses Light stimulates rods & cones which stimulate neurons that eventually merge to form the optic nerve (CN II) Some optic nerve fibers crosses at optic chiasma Visual center in the occipital cortex of the cerebrum interprets

19
Eye Muscles – Extrinsic & Intrinsic Groups
6 voluntary on outer surface of eye Controlled by CN III, IV, VI (oculomotor, trochlear, abucens) Convergence – pulling the eyeballs in a coordinated fashion so there is one visual field
 Convergence – pulling the eyeballs in a coordinated fashion so there is one visual field.")
20
Eye Muscles – Extrinsic & Intrinsic Groups
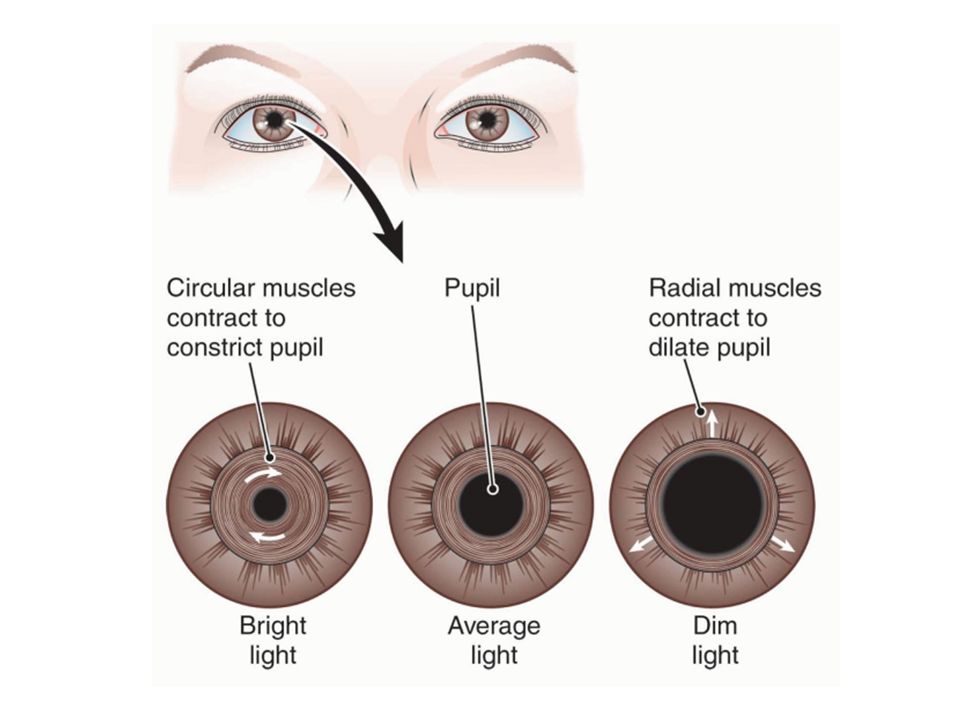
Involuntary muscles within the eyeball Controlled by CN III (oculomotor) Iris; pigmented part of the eye composed of 2 sets of muscles that control pupil size Circular muscle constricts in bright light Radial muscle constricts in dim light Ciliary muscle; holds the lens of the eye in place by suspensory ligaments Accomodation – ciliary muscle constriction changes the shape of the lens to allow for near & far vision
 Iris; pigmented part of the eye composed of 2 sets of muscles that control pupil size. Circular muscle constricts in bright light. Radial muscle constricts in dim light. Ciliary muscle; holds the lens of the eye in place by suspensory ligaments. Accomodation – ciliary muscle constriction changes the shape of the lens to allow for near & far vision.")
22
Intrinsic Eye Muscle Actions

23
The light rays from a close object diverge (separate) more than do the light rays from a distant object >>the lens must become more rounded to bend the light rays more When the ciliary muscle is relaxed, tension on the suspensory ligaments keeps the lens in a more flattened shape. For close vision, the ciliary muscle contracts For close vision, the ciliary muscle contracts, which draws the ciliary ring forward and relaxes tension on the suspensory ligaments. The elastic lens then recoils and becomes thicker

24
Nerve Supply to Eye Two sensory nerves supply the eye:
CNII – optic nerve; carries visual impulses from retinal rods & cones to the thalamus (diencephalon) to the visual center in occipital lobe of cerebrum CNV – trigeminal nerve, opthalmic branch; carries pain, touch & temperature impulses from the eye to the brain There are no retinal rods and cones in the area of the optic nerve. Consequently, no image can form on the retina at this point, which is known as the blind spot or optic disk
 to the visual center in occipital lobe of cerebrum. CNV – trigeminal nerve, opthalmic branch; carries pain, touch & temperature impulses from the eye to the brain. There are no retinal rods and cones in the area of the optic nerve. Consequently, no image can form on the retina at this point, which is known as the blind spot or optic disk.")
25
Nerve Supply to the Eye Three nerves carry motor impulses to the eyeball muscles: CNIII – oculomotor; largest motor nerve to the eyeball; supplies voluntary & involuntary muscles to all but two eye muscles CNIV – trochlear; supplies superior extrinsic eye muscle CNVI – abducens; supplies lateral extrinsic eye muscles

26
Steps in Vision Light refracts (bends)
Muscles of the iris adjust the pupil Ciliary muscle adjusts the lens (accomodation) Extrinsic eye muscles produce convergence (coordinate to allow one visual field) Light stimulates rods & cones Optic nerve transmits impulses to thalamus Thalamus transmits impulses to occipital lobe Occipital lobe cortex interprets impulses
 Extrinsic eye muscles produce convergence (coordinate to allow one visual field) Light stimulates rods & cones. Optic nerve transmits impulses to thalamus. Thalamus transmits impulses to occipital lobe. Occipital lobe cortex interprets impulses.")
27
Errors of Refraction Hyperopia – farsightedness
Usually due to abnormally short eyeball (flat cornea) Light focuses behind retina The lens can thicken only to a given limit to accommodate for near vision move an object away from the eye to see it clearly Glasses with convex lenses that increase light refraction Myopia – nearsightedness Usually due to abnormally long eyeball Light focuses in front of retina Distant objects appear blurred and may appear clear only if brought near the eye A concave lens corrects for myopia Astigmatism – blurred vision Cornea or lens curves irregularly, bending light incorrectly
 Light focuses behind retina. The lens can thicken only to a given limit to accommodate for near vision. move an object away from the eye to see it clearly. Glasses with convex lenses that increase light refraction. Myopia – nearsightedness. Usually due to abnormally long eyeball. Light focuses in front of retina. Distant objects appear blurred and may appear clear only if brought near the eye. A concave lens corrects for myopia. Astigmatism – blurred vision. Cornea or lens curves irregularly, bending light incorrectly.")
28
A. Normal B. Myopia C. Hyperopia D. Astigmatism

29
Eye Disorders Strabismus – deviation of the eye due to lack of coordination of eye muscles In convergent strabismus, the eye deviates toward the nasal side In divergent strabismus, the affected eye deviates laterally. if not corrected brain will not develop to see properly Amblyopia – loss of vision in a healthy eye because it cannot work properly with the other eye

30
Eye Disorders Conjuntivitis – inflammation of conjunctiva
Pinkeye – conjunctivitis caused by infection; is usually caused by cocci or bacilli Inclusion conjunctivitis is an acute eye infection caused by Chlamydia (AKA Trachoma) Corneal laceration – most common eye injury & if untreated can result in blindness Cornea is avascular so it is possible to receive transplant without rejection Enucleation – removes the eye due to traumatic injury Cataract – opacity of the lens which can lead to blindness Glaucoma – excess pressure in the eyeball due to aqueous humor not being reabsorbed into blood
 Corneal laceration – most common eye injury & if untreated can result in blindness. Cornea is avascular so it is possible to receive transplant without rejection. Enucleation – removes the eye due to traumatic injury. Cataract – opacity of the lens which can lead to blindness. Glaucoma – excess pressure in the eyeball due to aqueous humor not being reabsorbed into blood.")
31
Conjunctivitis & Cataract

32
Glaucoma

33
Disorders related to retina
Diabetic retinopathy – retina damaged by vascular hemorrhages & overgrowth Retinal detachment – retina separates from underlying layer as the result of trauma or fluid accumulation between tunics of eye Macular degeneration – macula lutea deteriorates & distorts visual field

34
Diabetic Retinopathy

35
Detached Retina

36
Macular Degeneration

37
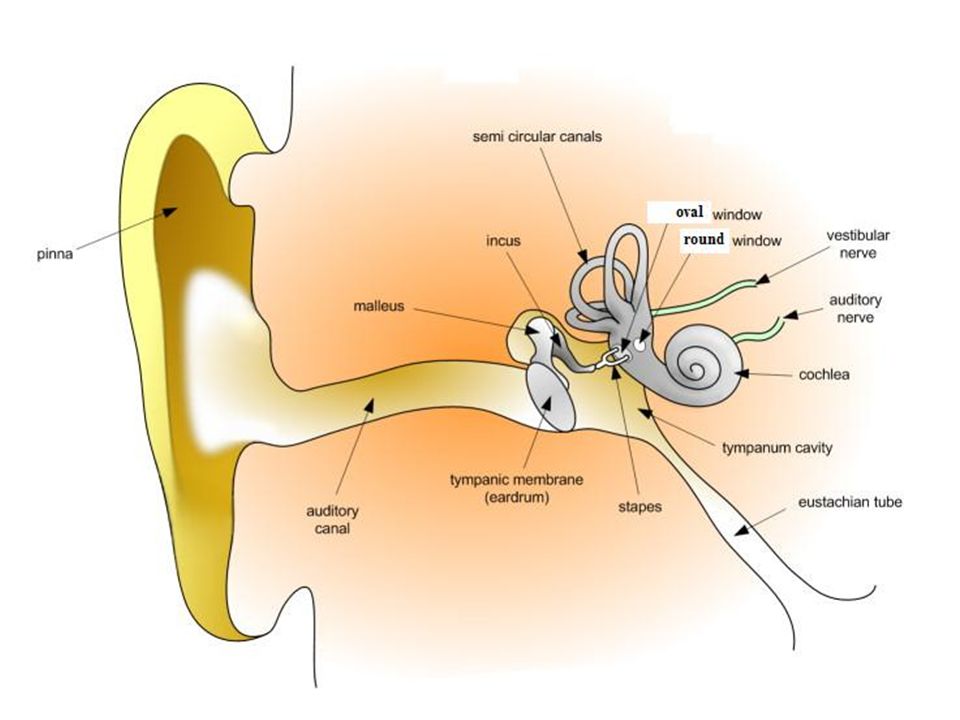
The Ear - Structure Outer ear – external ear to the tympanic membrane
Middle ear – contains 3 bones (ossicles) of ear & eustachian tube Inner ear – contains sensory receptors for hearing & equilibrium
 of ear & eustachian tube. Inner ear – contains sensory receptors for hearing & equilibrium.")
38
Outer Ear Pinna – aka auricle; the external ear
External auditory canal – aka external auditory meatus Contains ceruminous glands Tympanic membrane – aka eardrum Vibrates as sound waves enter the ear

39
Middle Ear - Ossicles Small cavity containing 3 ossicles (bones) that amplify sound waves received by tympanic membrane Malleus (hammer) – attached to tympanic membrane by handle & head attaches to incus Incus (anvil) – connects to malleus & stapes Stapes (stirrup) – connects to oval window, the membrane of inner ear
 – attached to tympanic membrane by handle & head attaches to incus. Incus (anvil) – connects to malleus & stapes. Stapes (stirrup) – connects to oval window, the membrane of inner ear.")
40
The middle ear- ossicles

41
Middle Ear – Eustachian Tube
Eustachian tube – connects middle ear to pharynx Allows pressure to equalize on the 2 sides of tympanic membrane

42
Inner Ear aka Bony Labyrinth
3 separate divisions of sensory receptors Vestibule, semicircular canals & cochlea Perilymph – fluid of inner ear Membranous labyrinth – within bony labyrinth & filled with endolymph

43
Inner Ear aka Bony Labyrinth
Vestibule – 2 bony chambers that contain equilibrium receptors Semicircular canals – 2 bony tubes that contain equilibrium receptors

44
Inner Ear aka Bony Labyrinth
Cochlea – bony coil that contains hearing receptors Round window – membrane through which sound waves leave the inner ear

46
Hearing Organ of Corti – sensory organ of hearing
Consists of ciliated receptor cells Located inside membranous cochlea aka cochlear duct Wave against the roof of the cochlear duct (tectorial membrane) Stimulates cochlear nerve (auditory branch of vestibulocochlear nerve CN VIII) Sound waves leave inner ear through round window
 Stimulates cochlear nerve (auditory branch of vestibulocochlear nerve CN VIII) Sound waves leave inner ear through round window.")
47
Steps of Hearing Sound waves vibrate tympanic membrane
Amplified by ossicles in middle ear Reach the oval window & create waves in the inner ear fluids Vibrating the chochlear duct Causing cilia or organ of Corti to wave against the tectorial membrane Cochlear nerve stimulated (branch of CNVIII) The temporal lobe of cerebrum interprets stimuli
 The temporal lobe of cerebrum interprets stimuli.")
48
Hearing Organ of Corti differentiates both pitch (tone) & intensity (loudness) Higher pitched tones near the base Lower pitched tones near the top Loud sounds stimulate more cells & produce more vibrations, sending more impulses to the brain

49
Equilibrium - Balance Sensory receptors are ciliated cells located in vestibule & semicircular canals Shifting in position of cilia within the thick fluid that surrounds them generates a nerve impulse Send impulses to vestibular branch of CN VIII (vestibulocochlear)
")
50
Equilibrium - Balance Static equilibrium- Sensing the position of head or body when moving in a straight line Due to vestibule receptors known as macula Fluid surrounding maculae contains crystals called otoliths which drag the fluid & increase pull of gravity Detail of Macula

51
Equilibrium Dynamic equilibrium – function during spinning or moving in different directions Semicircular canal receptors known as cristae

52
Ear Disorders Otitis media – inflammation of the middle ear
Children susceptible because short eustachian tube Otitis externia – inflammation of external auditory canal - aka swimmer’s ear

53
Hearing Loss Conductive hearing loss – interference with sound waves passing through ear Foreign body obstruction Tympanic membrane damage Otosclerosis – hereditary malfunction of stapes Sensorineural hearing loss – cochlea, CNVIII or temporal lobe of brain improperly transmit or interpret neural stimuli Prolonged exposure to loud noises Certain drugs or toxins Cochlear implant can stimulate cochlear nerve directly, bypassing receptor cells Presbycusis – age related hearing loss due to atrophy of sensory receptors an CNVIII fibers

54
Loud Noise Damage to Ear

55
Taste - Gustation Tongue receptors aka taste buds
Taste buds are stimulated only if the substance to be tasted is in solution or dissolves in the fluids of the mouth Sweet – tip of the tongue Salty – middle of tongue Sour – middle sides of tongue Bitter – posterior tongue Transmitted along CN VII & IX (facial & glossopharyngeal) to frontal cortex; no special center in cortex Other tastes include water, alkaline, metallic Tastes can be combined with smells
 to frontal cortex; no special center in cortex. Other tastes include water, alkaline, metallic. Tastes can be combined with smells.")
56
Smell - Olfaction Important for protection, taste, triggering memory, sexual behavior Receptors located in superior nasal cavity Conduct impulses along olfactory nerve (CNI) to olfactory center in temporal lobe of cerebral cortex
 to olfactory center in temporal lobe of cerebral cortex.")
57
General Senses Located throughout body Touch Pressure Temperature
Position Pain

58
General Senses Touch – The touch receptors, tactile (TAK-til) corpuscles, are found mostly in the dermis of the skin and around hair follicles Meissner corpuscles in skin, also near hair follicles; # of corpuscles determines sensitivity to touch Lips, tip of tongue, fingertips very sensitive Back, back of hand less sensitive Pressure – Pacinian corpuscles in skin, also near joints sensory end-organs Can respond even when a person is under anesthesia

59
General Senses Temperature – free nerve endings; dendrite branches
Widely distributed in skin Separate branches for heat & cold Stimulus travels to hypothalamus (diencephalon) Position – proprioceptors - receptors located in joints, muscles, tendons Kinesthesia – sense of body movement – where the body is in time & space Inform brain about muscle contraction/tendon tension Muscle tone, posture, coordination, complicated skills Stimulus travels to cerebellum
 Position – proprioceptors - receptors located in joints, muscles, tendons. Kinesthesia – sense of body movement – where the body is in time & space. Inform brain about muscle contraction/tendon tension. Muscle tone, posture, coordination, complicated skills. Stimulus travels to cerebellum.")
61
Temperature & Proprioceptors

62
General Senses Pain – free nerve endings; widely distributed in skin, muscles, joints, and scattered sparsely in viscera & blood vessels Nocioceptors – nerve endings that transmit pain signals Sharp – acute, fast Adelta fibers Dull – slow, chronic C fibers

63
Pain The 5th vital sign An unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Pain is always subjective Pain is whatever the experiencing person says it is, existing whenever he or she says it does

64
Neuroanatomy of Pain Nocioception – how noxious stimuli are perceived as pain 3 phases of nocioception Transduction – a noxious stimulus occurs peripherally and travels to the spinal cord Transmission – pain impulse moves from the level of the spinal cord to the brain Perception – conscious awareness of a painful sensation Modulation – pain is inhibited The brain sends signals to slow down or impede the pain impulse

65
Sources of Pain Visceral pain – from organs
Deep somatic pain – from structures like vessels, bones, muscles, joints Cutaneous pain – from skin Referred pain – pain felt at a particular site but originates at a different location innervated by the same spinal nerve Neuropathic pain – an abnormal neurological processing of pain signals the most difficult to assess & treat Pain often perceived long after the site of injury heals

66
Referred Pain

67
Different Pain Scales

68
Neonatal Pain Scoring

69
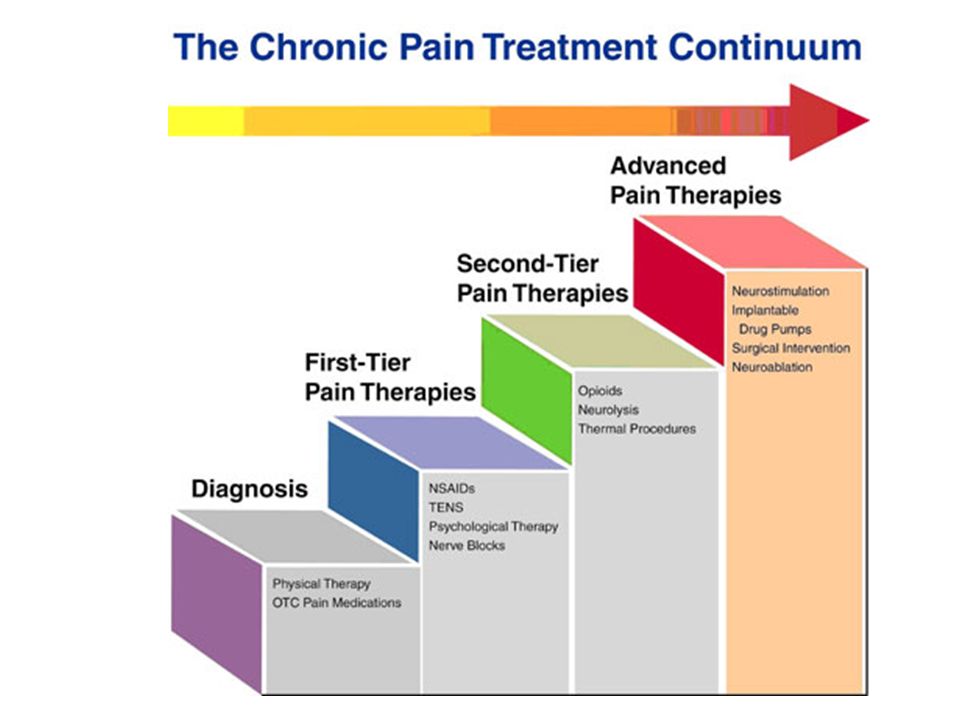
Pain Relief Analgesics – drugs that relieve pain
Nonnarcotic analgesics – act locally to reduce inflammation i.e. NSAIDs Narcotics – act on CNS to alter the perception of pain Anesthetics – drugs that block pain Endorphins – chemicals released from the brain to modulate pain; massage can activate endorphins Heat – reduces chronic pain as long as there is no inflammation Cold – acts as an anesthetic; reduces inflammation; when in doubt, ice Relaxation or distraction techniques

71
Sensory Adaptation Sensory receptors exposed to continuous stimulus adjust so sensation becomes less acute; warmth, cold & light pressure adapt rapidly Pain receptors do not adapt; C fiber (slow pain) receptors become more sensitive if exposed to continuous stimulation
 receptors become more sensitive if exposed to continuous stimulation.")
72
Chronic Pain

73
Chronic Pain

Similar presentations




















 detects a physical or chemical change. 2. The physical or chemical change causes action potentials.>")
