Download presentation
Presentation is loading. Please wait.

1
ImmunoPathogenesis of HIV Disease Overview of HIV Epidemic Basic biology of HIV-1 Stages of HIV Disease Viral and Cellular Dynamics after HAART HIV Therapy and Future Directions in Pathogenesis Research

2
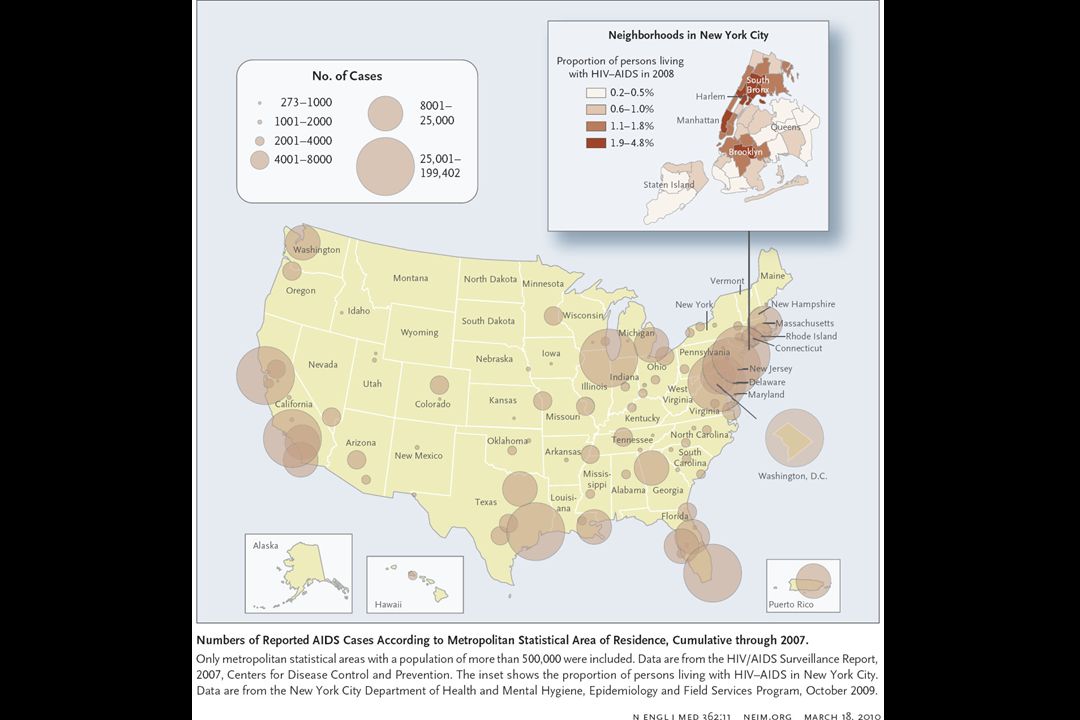
Overview of HIV Epidemic Origin of virus Scope of worldwide Epidemic Brief History of Epidemic –Immunodeficiency syndrome identified (GRID) in late 1970’s –Identification of virus and development of serological test - 1984 –Introduction of first antiretroviral drug (AZT) – 1987 –Identification of three stages of disease – early 1990’s –Competitive RT-PCR to measure viral RNA in plasma – 1993 –combination antiretroviral drugs (protease inhibitors & RTI) – 1995 –Introduction of ART to Africa – 2001 –Epidemic still expanding – 2006
 in late 1970’s –Identification of virus and development of serological test –Introduction of first antiretroviral drug (AZT) – 1987 –Identification of three stages of disease – early 1990’s –Competitive RT-PCR to measure viral RNA in plasma – 1993 –combination antiretroviral drugs (protease inhibitors & RTI) – 1995 –Introduction of ART to Africa – 2001 –Epidemic still expanding – 2006")
3
Death rates in persons aged 25-44 years in the United States

5
A global view of HIV infection 38.6 million people [33.4 ‒ 46.0 million] living with HIV, 2005
![A global view of HIV infection 38.6 million people [33.4 ‒ 46.0 million] living with HIV, 2005](http://images.slideplayer.com/27/8999706/slides/slide_5.jpg "A global view of HIV infection 38.6 million people [33.4 ‒ 46.0 million] living with HIV, 2005")
8
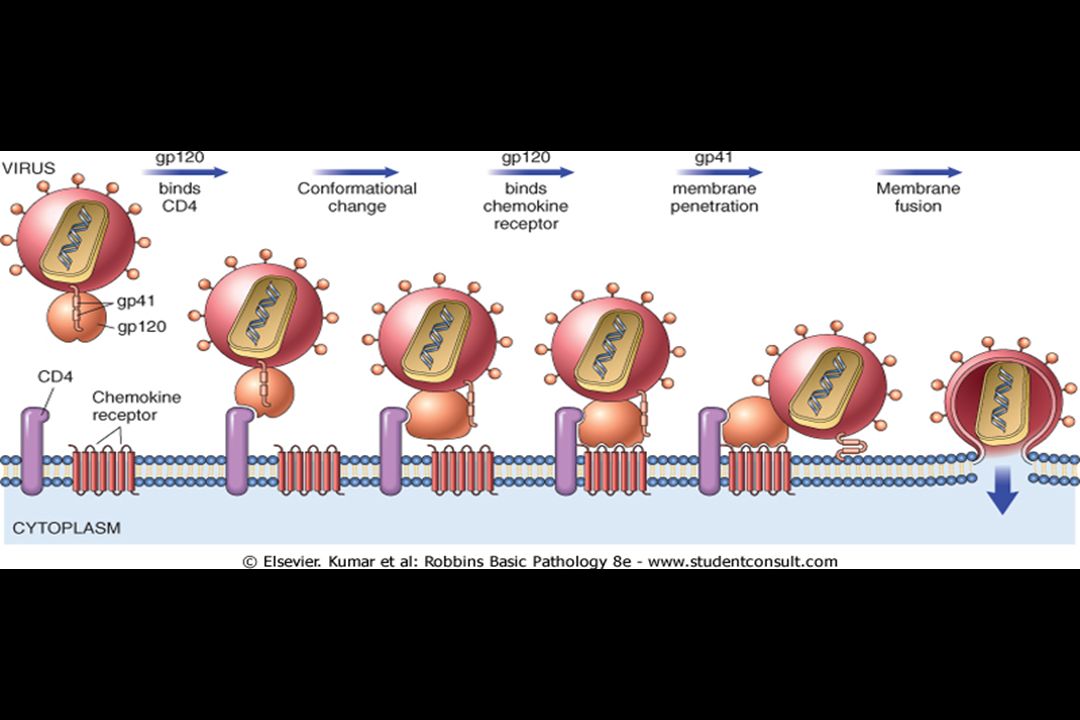
Life cycle of HIV Viral Entry - CD4 and co-receptors Reverse Transcription Integration into host chromatin Transcriptional activation of integrated provirus Production of viral proteins, particle assembly and maturation

11
Chemokine Co-receptors for HIV Two co-receptors - CXCR4 and CCR5 with distinct viral isolates CXCR4 - T tropic - syncytium inducing - present in late stage disease CCR5 - M tropic - non- syncytium inducing - dominant in early infection Natural ligands - SDF-1/CXCR4 & MIP-1 , MIP-1 , & RANTES/CCR5 Protection from infection in CCR5 32 homozygotes

12
HIV Latent Infection Pre-integration latency –After reverse transcription, before integration –Due to lability of unintegrated DNA, this pool is dependent on continual de novo infection Integrated latency –Integrated provirus with low or absent transcription of viral genes (no expression no clearance) –Likely the major reason for eradication failure –Controversy about origin, role of defective viral genomes, chromatin integration sites, and clearance rate
 –Likely the major reason for eradication failure –Controversy about origin, role of defective viral genomes, chromatin integration sites, and clearance rate")
13
High viral mutation rate Reverse Transcriptase is fairly sloppy and cellular RNA polymerases are not high fidelity enzymes Estimated to be around 1000 different sequence variants in a single individual at one time Rapid evolution of drug resistance, if there is continued de novo infection In general, inverse relationship of “viral fitness” in vivo growth rate and drug resistant phenotype. Wild type virus grows out when drugs withdrawn. Partial drug mediated inhibition of growth is recipe for resistance

14
Diagnosis of HIV Infection Signs & Symptoms of Primary Infection HIV Ab measurement (EIA Western Blot) HIV viral RNA in plasma Response to suspected exposure (needle stick) Post-exposure prophylactic ART
 HIV viral RNA in plasma Response to suspected exposure (needle stick) Post-exposure prophylactic ART")
15
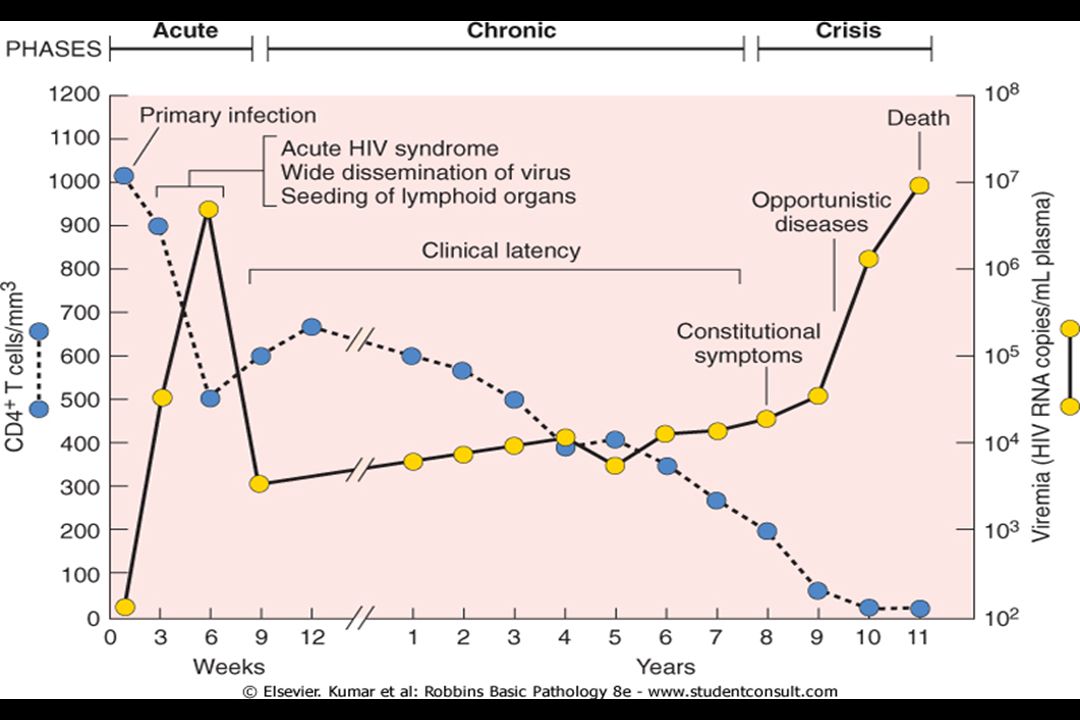
Laboratory Testing for AIDS Antibody testing —to diagnose HIV infection. p24 protein testing —may be used to detect early HIV infection, to monitor HIV therapy and HIV progression, and to screen blood for HIV. Viral load testing —to decide when to start therapy and to monitor therapy and HIV progression. –In chronic phase, the extent of viremia (as measured by HIV-1 RNA) can predict disease progression CD4 testing —to decide when to start therapy and to monitor therapy, HIV progression, and the status of the immune system. –>500 asymptomatic –200-499 early symptoms –<200 severe immunosuppression Genotypic resistance testing —to determine if a particular strain of HIV is resistant to the therapy you are on and if the therapy should be switched.
 can predict disease progression CD4 testing —to decide when to start therapy and to monitor therapy, HIV progression, and the status of the immune system. –>500 asymptomatic – early symptoms –<200 severe immunosuppression Genotypic resistance testing —to determine if a particular strain of HIV is resistant to the therapy you are on and if the therapy should be switched..")
16
Occupational Exposure to HIV Concept of Universal precautions –Any human bodily fluids could be contaminated with infectious agents transmitted by parenteral exposure. In case of possible exposure, immedately report to HIV response team (at UAB 4-3675) or ER. Early Treatment with antiretroviral drugs have very substantial benefit –Time after infection is critical. –Excellent results if ART started within several days.
 or ER. Early Treatment with antiretroviral drugs have very substantial benefit –Time after infection is critical. –Excellent results if ART started within several days..")
17
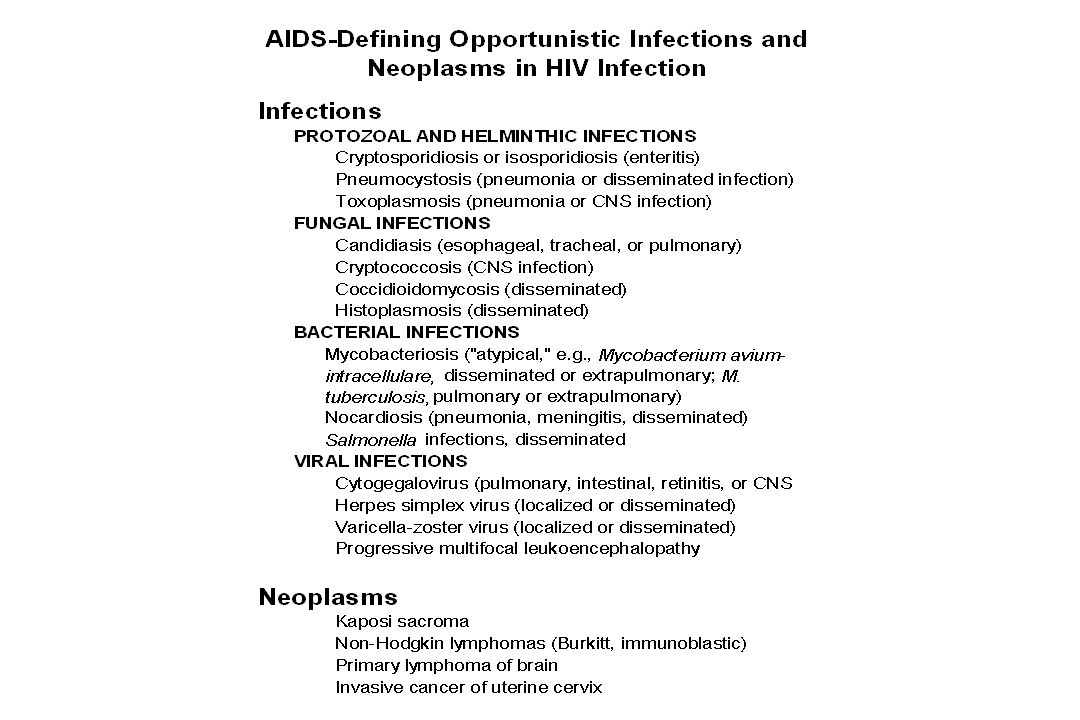
Three Phases of HIV Disease Acute Infection Syndrome –“flu-like” clinical illness –high viral load that resolves coincident with development of effective CD8 T cell response Clinical “Latent” Disease –Widely variable viral load correlated with rate of disease progression (loss of CD4 T cells) –Lymphadenopathy and constitutional symptoms End Stage Disease (AIDS) –CD4 T cells < 200; often increase in viral load –development of opportunistic infections
 –Lymphadenopathy and constitutional symptoms End Stage Disease (AIDS) –CD4 T cells < 200; often increase in viral load –development of opportunistic infections")
21
Initial Rate Independent of Absolute vRNA t ½ 1 day HAART Viral Dynamics after HAART

22
Dynamics of HAART Induction Rapid fall in viral RNA in plasma –First phase is very rapid (t ½ = 1-1.5 days) and fairly consistent among individuals, second phase slower. Rapid Increase in CD4 T cells in Blood –Redistribution of lymphocytes from inflammed tissue is primary mechanism - previously thought to be change in CD4 T cell growth Significant Immune Reconstitution –Decreased incidence of OIs and death

23
Despite initial optimism, infection not eradicated Concept of Reservoir - residual viable virus during HAART –Latently infected CD4 T cells –Sequestered Anatomic site - CNS, ?others –Persistent rounds of de novo infection –Intermittent Non-adherence Slow evolution of viral quasispecies sequences Status of HIV Dynamics on HAART Both Latent infection and persistent vRNA+ cells - Tissue and Blood

24
Goals in Medical Management of HIV Disease Pharmacological suppression of viral Replication –Multiple drugs available – low replication low mutations –Monitoring status – viral load and CD4 count Eradication - complete elimination of viable virus –Problems - HAART alone does not result in Eradication. Regimen is difficult - Intermittent regimen Non-Adherence Development of Drug Resistance Persistent population of latently infected CD4 T cells Induction of Immune Control –Increase efficiency of immune response to viral antigen to maintain control of replication at very low viral load –Low viral load = Lack of disease progression –Normal “successful” outcome of chronic viral infection

Similar presentations













 is the virus that causes Acquired Immunodeficiency Syndrome (AIDS).>")







 AIDS was first reported in the US in 1981 –Origin in Africa in 1950s.>")

