Download presentation
Presentation is loading. Please wait.

1
Russell E. Berger, MD Co-Director of Medical Toxicology Emergency Physician Cambridge Health Alliance Instructor in Medicine Harvard Medical School

2
Brief Outline -Toxidromes -The “Tox” EKG -Guidance on some of the most common ingestions -Agents of Concern -Agents of little or no concern -Q &A

3
Toxidromes A way that we can group symptoms together which helps us formulate a treatment plan. Vital Signs Mental Status Pupils Skin Findings Neurologic Exam

4
Opiate Toxidrome Vitals signs: Down - low heart rate, low blood pressure Mental Status: Down (asleep) Pupils: Down(small) Skin Finding: - Needle tracks, usually cool and dry
 Pupils: Down(small) Skin Finding: - Needle tracks, usually cool and dry")
5
Sympathomimetic Vital signs: up: -high heart rate, hypertensive Mental Status: up -agitated-VIOLENT Pupils(up) Skin findings(sweaty)
 Skin findings(sweaty)")
6
Anticholinergic Vital Signs: Up Mental Status: -Agitated, DELIRIOUS Pupils: Up Skin: DRY

7
Serotonergic AMS Hyper-reflexia (clonus is most important feature. Dysautonomia(Vital sign abnormalities, usually activated)
.")
8
Sympathomimetic versus Anticholinergic Freddy Kruger Versus The Cookie Monster

9
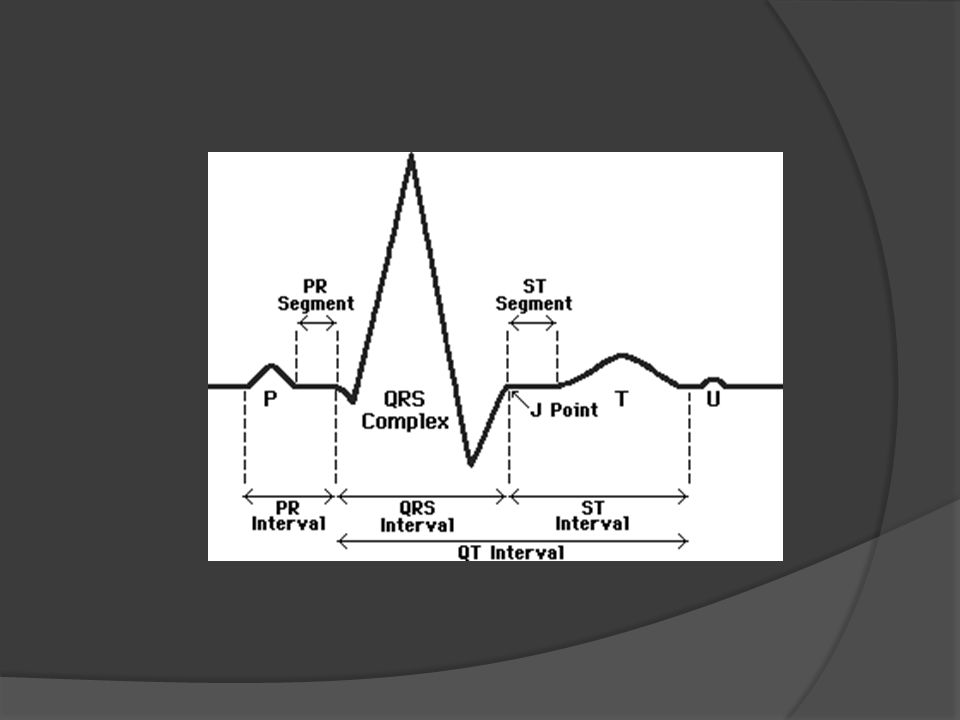
Tox EKG QRS duration QTC duration Terminal R in aVR

11
If you block Sodium channels… You prolong the QRS complex >100ms is significant Just read from the top of the cardiogram

12
If you block Potassium Channels… You prolong the QTC >450ms is significant Just go by what’s reported on the top of the cardiogram

13
Some Na Channel Blockers besides TCA’s Carbamazepine Benadryl Flecainide, Procainamide Chloroquine Propranolol Quinine Bupivicaine

14
Some QTC prolonging Agents Seroquel Zofran Methadone Trazodone Citalopram Erythromycin

15
DRUGS

16
Tylenol It is in everything. It produces early symptoms that are easy to overlook. Have a low threshold to test for it and a low threshold to treat in overdose.

17
Tylenol We have NAC to treat this overdose. The dosing of NAC is very confusing for people so needs to be checked carefully for accuracy. NAC may produce a scary appearing reaction during loading. Still give it!

18
Opiates One of the most worrisome emerging epidemics. RESPIRATORY RATE is the most important reason to give Narcan. Remember Narcan has a short half life compared with the agents it is reversing. Observe, Observe, Admit, Observe.

19
Give Narcan sparingly to avoid precipitating patient distress. Don’t forget to check a tylenol level. Detectable tylenol levels should = NAC treatment and admission (in the setting of combined opiate preps, eg percocet)
.")
20
Aspirin One of the most dangerous agents we see. 30, 60, 90 rule; chronic levels are worse than acute levels so get treated earlier. Single levels are not adequate to medically clear a patient

21
Aspirin Any change in mental status = dialysis Seizures = death If you are at a facility without reliable renal coverage, push to transfer the patient.

22
Carbon Monoxide Exposures Flu like symptoms Is the dog sick or not? Duration of exposure is as important as level While level is cooking, NRB based 100% oxygen.

23
Carbon Monoxide If your patient is pregnant, worry about them. Patients will have a functional anemia. Chest pain SOB Dizziness Headache. If in doubt, talk to a dive chamber for guidance.

24
Lithium Check the level. Is the level post-distribution---was the blood drawn >6 hours after the last dose of medication. If yes, it is reliable. If not, it may not be reliable. Is the patient neurotoxic? Can they walk?

25
Substantial alteration in mental status is always a reason to dialyze (esp with co- ingestants). Early dialysis is associated with better patient outcomes. Level is NOT everything. Give sodium to trick the kidneys into eliminating lithium as early as you can.

26
Benadryl In everything Patient can get SUPER sick Don’t forget your NAC (eg tylenol PM). May act like a TCA overdose

27
Benadryl Patient will be dry, delirious, and tachycardic. They may have prolongation of their QRS complex on EKG. They may seize and develop ventricular dysrhythmias.

28
Sympathomimetic Agents Cocaine LSD Ecstacy Bath Salts PCP Ketamine

29
Crazy and aggressive. Wide eyed and pouring sweat Control with benzodiazepines/Avoid Haldol. Keep the patient cool. Intubate and paralyze PRN.

30
Clonidine Very common in both pediatric and adult populations(ADHD or withdrawal) Sedation Produces hypotension, bradycardia with normal potassium and glucose. Looks like opiate---pinpoint pupils---may respond to narcan

31
Digoxin Hypotension, bradycardia, hyperkalemia. More common in the elderly or in cardiac kids. Can reverse with digibind. Labs for digoxin will be off when you check the level again. Don’t freak out about this-- -go by the clinical picture.

32
Digoxin Consider treating the potassium itself Avoid calcium (for now) Concentration x Wt in Kg/100 gives you reversal dose of digibind (round up) Pt is 80 kg, dig level is 4.0. [80]x[4]/100 = 3.2 Give 4 vials

33
Calcium Channel Blockers Hypotension, bradycardia, HYPERglycermia The worst of the worst ingestions High Dose insulin therapy Intralipid ECMO/Intra-aortic balloon pump.

34
Seroquel “I take seroquel for sleep.” Ataxia Prolongation of the QT. May need to be tubed 2/2 decreased mental status.

35
Sleeping Pills Ambien Lyrica Gabapentin Lunesta A lot of worry Little true concern

36
Agents to not worry about Motrin(unless > 400mg/kg) Most Antibiotics SSRI’s Thyroid Hormone Laxatives Most diuretics Ace inhibitors ARBS Vitamins(except prenatals) Sleep aids Benzodiazepines
 Most Antibiotics SSRI’s Thyroid Hormone Laxatives Most diuretics Ace inhibitors ARBS Vitamins(except prenatals) Sleep aids Benzodiazepines")
37
Household Items(bedroom and bathroom) I don’t care: Makeup Household bleach Dish soap Bath soap Dish detergent (Pods are different) Shampoo Rat poison Raid Vitamins
 I don’t care: Makeup Household bleach Dish soap Bath soap Dish detergent (Pods are different) Shampoo Rat poison Raid Vitamins")
38
Household items(garage) Emergency: -Gasoline/Kerosone -Oil of wintergreen(salicylate) -Antifreeze(EG) -De-icer(Methanol) -Button Batteries -Wheel Cleaners(HF) -Essential Oils(citronella)
 Emergency: -Gasoline/Kerosone -Oil of wintergreen(salicylate) -Antifreeze(EG) -De-icer(Methanol) -Button Batteries -Wheel Cleaners(HF) -Essential Oils(citronella)")
39
Admit these kids Oral sulfonylureas(glipizide, glimeperide, etc) Long acting opiates, suboxone and methadone TCA’s Calcium Channel Blockers Most beta blockers MAOi exposures Wellbutrin
 Long acting opiates, suboxone and methadone TCA’s Calcium Channel Blockers Most beta blockers MAOi exposures Wellbutrin")
40
Specific Agents: Questions Contact: rberger@challiance.org

41
Thank you

Similar presentations







 may be used to terminate status epilepticus?>")











