Download presentation
Presentation is loading. Please wait.

1
Renal Megan McClintock, RN, MS 10/27/11 “TO PEE IS TO LIVE”

2
"Bones can break, muscles can atrophy, glands can loaf, even the brain can go to sleep without immediate danger to survival. But should the kidneys fail … neither bone, muscle, gland, nor brain could carry on.” Smith HW: Fish to philosopher, Boston, 1953, Little, Brown.

3
KIDNEY DISEASE Acute kidney injury (AKI)Chronic kidney disease (CKD) Sudden onset Acute decrease in urine output and/or increase in creatinine Potentially reversible Mortality 60% Usually die from infection Gradual onset GFR 3 months Progressive and irreversible Mortality 19-24% (need dialysis to survive) Usually die from CV disease
Chronic kidney disease (CKD) Sudden onset Acute decrease in urine output and/or increase in creatinine Potentially reversible Mortality 60% Usually die from infection Gradual onset GFR 3 months Progressive and irreversible Mortality 19-24% (need dialysis to survive) Usually die from CV disease")
4
ACUTE KIDNEY INJURY Prerenal causes – external to the kidney, sudden reduction in blood flow to the kidneys Usually resolve quickly with correction of cause Intrarenal causes – infections, toxins, drugs, or direct trauma, ATN Postrenal causes –urinary tract obstructions Usually resolve quickly with correction of cause

5
ACUTE KIDNEY INJURY CLINICAL COURSE Oliguric Phase (10-14 days) –Urine output less than 400 mL/day –UA w/ casts, RBCs, WBCs, SG fixed at 1.010, urine osmo of 300 mOsm/kg (may have proteinuria) –Volume depletion but oftentimes fluid retention –Metabolic acidosis –Sodium imbalance –Potassium increase –Hematologic disorders –Waste product accumulation –Neuro disorders
 –Urine output less than 400 mL/day –UA w/ casts, RBCs, WBCs, SG fixed at 1.010, urine osmo of 300 mOsm/kg (may have proteinuria) –Volume depletion but oftentimes fluid retention –Metabolic acidosis –Sodium imbalance –Potassium increase –Hematologic disorders –Waste product accumulation –Neuro disorders")
6
ACUTE KIDNEY INJURY CLINICAL COURSE Diuretic Phase (1-3 weeks) –Begins with a gradual increase in daily urine output to 1-3 L –Nephrons still not fully functional –Kidneys can excrete waste, but still can’t concentrate the urine –Hypovolemia –Hypotension –Hyponatremia, hypokalemia
 –Begins with a gradual increase in daily urine output to 1-3 L –Nephrons still not fully functional –Kidneys can excrete waste, but still can’t concentrate the urine –Hypovolemia –Hypotension –Hyponatremia, hypokalemia")
7
ACUTE KIDNEY INJURY CLINICAL COURSE Recovery Phase (12 months) –Begins when the GFR increases –BUN and creatinine plateau, then decrease
 –Begins when the GFR increases –BUN and creatinine plateau, then decrease")
8
ACUTE KIDNEY INJURY TREATMENT Eliminate the cause, manage signs & symptoms, prevent complications –#1 goal is to ensure adequate cardiac output and intravascular volume –Careful monitoring of I/Os –Prevent hyperkalemia –Use RRT (renal replacement therapy) only if needed –Nutritional management
 only if needed –Nutritional management")
9
ACUTE KIDNEY INJURY TREATMENT Avoid exposure to contrast media Watch for nephrotoxic drugs ACE inhibitors Meticulous aseptic technique Meticulous skin care Meticulous mouth care

10
ACUTE KIDNEY INJURY NURSING DIAGNOSES Decreased cardiac output Excess fluid volume Risk for infection Imbalanced nutrition: less than body requirements Fatigue Anxiety Dysrhythmias Sensory/perceptual alterations

11
CHRONIC KIDNEY DISEASE

12
Frequently asymptomatic Early on have no change in urine output, may even have polyuria Uremia develops when GFR is <10 mL/min Persistent proteinuria Tend to die of CV disease before needing dialysis

13
Fig 45-3 clinical manisfestations of chronic uremia

14
CHRONIC KIDNEY DISEASE TREATMENT Treat high potassium Control HTN Treat anemia (EPO) Treat hyperlipidemia Restrict proteins Restrict fluids Restrict sodium, potassium, phosphates Lots of teaching and reteaching
 Treat hyperlipidemia Restrict proteins Restrict fluids Restrict sodium, potassium, phosphates Lots of teaching and reteaching")
15
TREATING HYPERKALEMIA Insulin Sodium Bicarbonate Calcium Gluconate IV Dialysis Sodium Polystyrene Sulfonate (kayexalate) Dietary Restriction
 Dietary Restriction")
16
Dialysis Peritoneal Dialysis (PD)Hemodialysis (HD)
Hemodialysis (HD)")
22
PERITONEAL DIALYSIS Three phases of PD Manual vs Continuous Complications

25
Fig 45-12 Temporary catheters Fig 45-13 placement of jugular vein temporary dialysis catheter

26
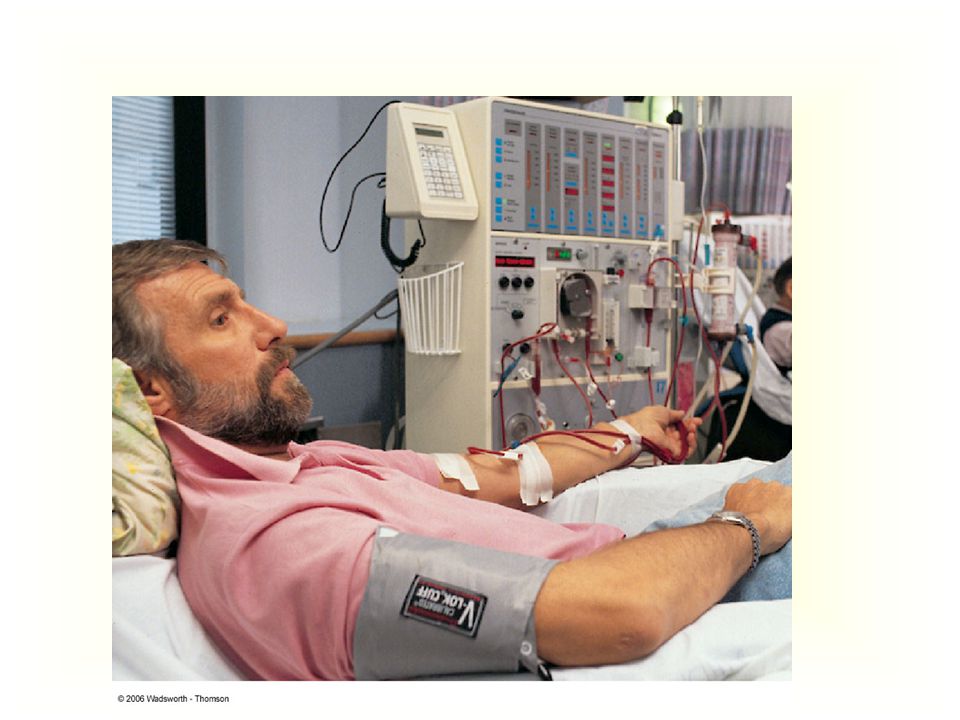
Fig 45-14 components of hemodialysis system

28
HEMODIALYSIS Pre & Post Dialysis Interventions Complications –Hypotension –Muscle cramps –Blood loss –Hepatitis

29
PYELONEPHRITIS Cause – Bacteria (most common) S/S – abrupt onset of chills, fever, vomiting, malaise, CVA pain, dysuria, urinary urgency and frequency Labs – UA w/ pyuria, bacteriuria, hematuria, WBC casts; CBC w/ left shift (increase in bands) Cx – Urosepsis leading to septic shock and death, chronic pyelonephritis
 S/S – abrupt onset of chills, fever, vomiting, malaise, CVA pain, dysuria, urinary urgency and frequency Labs – UA w/ pyuria, bacteriuria, hematuria, WBC casts; CBC w/ left shift (increase in bands) Cx – Urosepsis leading to septic shock and death, chronic pyelonephritis")
30
Pyelonephritis: glomerular hemorrhage

31
Pyelonephritis - papillary necrosis

32
PYELONEPHRITIS INTERVENTIONS Early tx for cystitis Take antibiotics as prescribed Follow-up urine culture Drink at least 8 glasses of fluid daily Rest

33
GLOMERULONEPHRITIS Cause – Antibody-induced injury (exposure to drugs, immunizations, microbial/viral infxn) S/S – generalized edema, HTN, oliguria, hematuria, proteinuria, abd/flank pain Labs – UA w/ proteinuria, hematuria, WBC casts; increased BUN and creatinine, ASO titer Cx – Renal insufficiency, destruction of renal tissue
 S/S – generalized edema, HTN, oliguria, hematuria, proteinuria, abd/flank pain Labs – UA w/ proteinuria, hematuria, WBC casts; increased BUN and creatinine, ASO titer Cx – Renal insufficiency, destruction of renal tissue")
34
GLOMERULONEPHRITIS INTERVENTIONS REST Diuretics, restricted sodium and fluids Restrict dietary protein if in BUN. Treat severe HTN with anti-hypertensives No abx unless infection still present Prevention - Take the FULL course of antibiotics (treat strep)
.")
35
NEPHROTIC SYNDROME Cause – systemic disease, allergens, drugs, infxn, glomerulonephritis S/S – edema, massive proteinuria, HTN, hypoalbuminemia, hyperlipidemia Labs – low albumin, low protein, high cholesterol Cx – Infection, thromboembolism, skin breakdown, malnourishment, body image problems

38
NEPHROTIC SYNDROME INTERVENTIONS ACE inhibitors, corticosteroids, diuretics, lipid- lowering agents Low sodium, low-moderate protein diet (focus on preventing malnutrition) Strict I/Os, daily weights Protect skin Prevention of infection
 Strict I/Os, daily weights Protect skin Prevention of infection")
39
Minute paper On the provided 3x5 card answer the following: 1)What was the most important thing you learned today. 2)What important point remains unclear to you?
What important point remains unclear to you .")
Similar presentations










activate vitamin D (renal 1-alpha hydroxylase) produces erythropoietin.>")






 Dr. Belal Hijji, RN, PhD April 18 & 23, 2012.>")











 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")