Download presentation
Presentation is loading. Please wait.

1
NUTRITION AND CANCER: BEFORE, DURING AND AFTER Andrew D. Nish MD

2
NUTRITION AND CANCER: BEFORE, DURING AND AFTER A simple question: IS CANCER A PREVENTABLE DISEASE?

3
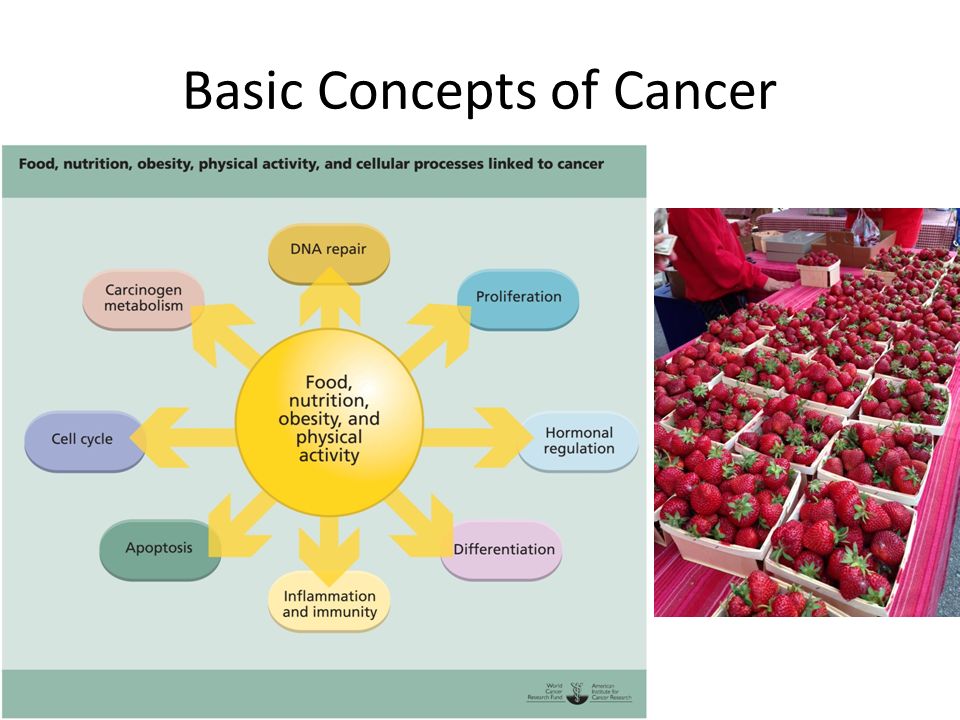
Basic Concepts of Cancer 5-10% of cancers result directly from inheriting genes associated with cancer The majority of cancers involve alterations or damage accumulated over time to the genetic material within cells The causes of damage are both endogenous (internal) and exogenous (environmental) FOOD, NUTRITION AND PHYSICAL ACTIVITY ARE IMPORTANT ENVIRONMENTAL FACTORS IN THE DEVELOPMENT OF CANCER The hallmark of cancer is unregulated cell growth and/or cell death
 and exogenous (environmental) FOOD, NUTRITION AND PHYSICAL ACTIVITY ARE IMPORTANT ENVIRONMENTAL FACTORS IN THE DEVELOPMENT OF CANCER The hallmark of cancer is unregulated cell growth and/or cell death")
4
Basic Concepts of Cancer

6
Concepts of Cell Function and Obesity The normal functioning of all biological processes depends on the availability of substrates and nutrients. Good nutrition – appropriate provision of food and nutrients from the level of the whole organism to the cellular and intracellular level- is needed for normal structure and function. When a person is not suitably nourished, either through under- or overnutrition, this impacts the tissue microenvironment, compromising both structure and function. Overall dietary patterns can indirectly influence cell growth by way of changes in general metabolic, regulatory and endocrine effects.

7
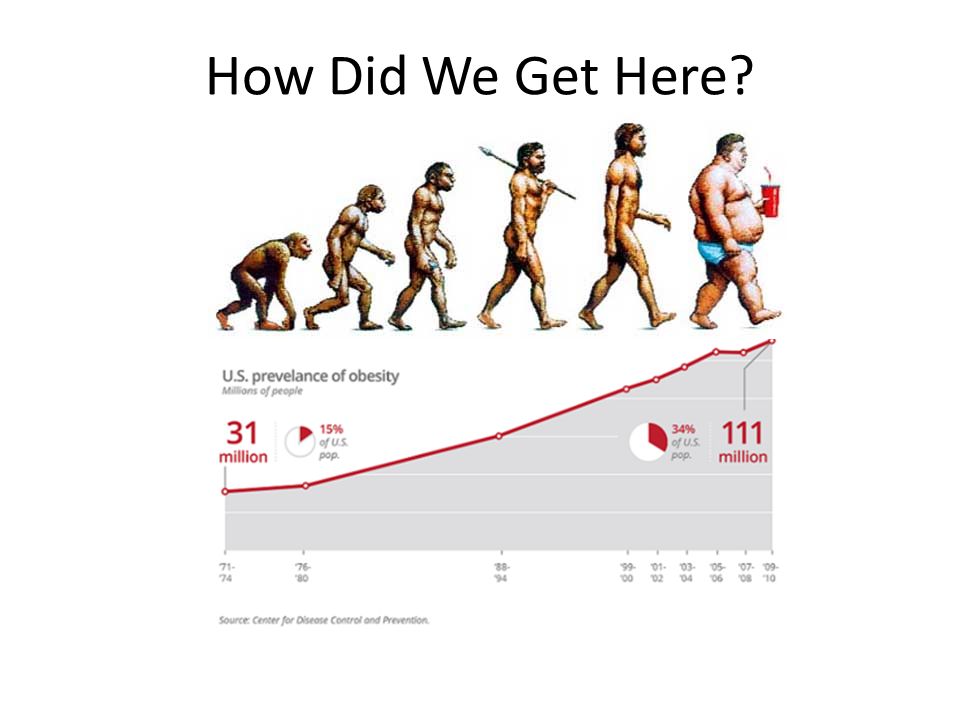
Concepts of Cell Function and Obesity The prevalence of obesity has doubled globally over the past 30 years. Today 65% of the population lives in countries where obesity kills far more people than underweight ( WHO fact sheet 311. Obesity and Overweight;2011 ) The prevalence of adult obesity in the US 2011-2012 – 34.9% and youth 17% ( JAMA.2014;311(8) 806-814 ) CDC estimates that 75 million Americans have metabolic syndrome – this is truly astounding!!!
 The prevalence of adult obesity in the US – 34.9% and youth 17% ( JAMA.2014;311(8) ) CDC estimates that 75 million Americans have metabolic syndrome – this is truly astounding!!!.")
8
Concepts of Cell Function and Obesity

9
So what? Why are we talking about metabolic syndrome? I thought we are suppose to be talking about cancer Well, metabolic syndrome increases cancer risk through metabolic disturbances that promote genetic instability (increased risk in 75 million people) The inflammatory state associated with obesity and metabolic syndrome is one mechanism that promotes cancer
 The inflammatory state associated with obesity and metabolic syndrome is one mechanism that promotes cancer.")
10
Energy Excess and Cancer When energy intake exceeds energy expenditure, the resulting state of nutrient excess can trigger responses in many cell types – endothelial cells, hepatocytes, myocytes, adipocytes and macrophages Nutrient excess can lead to the production of reactive oxidative species (molecules generated during fuel production by the mitochondria) Excessive production of these molecules creates “oxidative stress” which can damage cellular structures and trigger an inflammatory response
 Excessive production of these molecules creates oxidative stress which can damage cellular structures and trigger an inflammatory response")
11
Energy Excess and Cancer Nutrient excess can also impair functioning of the endoplasmic reticulum giving rise to unfolded proteins which can itself induce inflammation A third response to nutrient excess is the accumulation of long-chain fatty acyl coenzyme A molecules (driven mainly by fructose) further increasing inflammation
 further increasing inflammation")
12
Energy Excess and Cancer Inflammation can limit further exposure to nutrients by blocking the action of insulin The binding of insulin or IGF-1 to cell surface receptors activates the PL3K/Akt pathway leading to downstream activation of the mTOR complex, a central regulator of cell growth and mitogenesis. Data strongly suggests that endogenous hyperinsulinemia may be one obesity-related factor enhancing cancer growth and metastases In women with breast cancers a worse prognosis has been noted in those with higher circulating levels of insulin.

13
Energy Excess and Cancer

14
Factors associated with cell growth, carcinogenesis and tumor promotion: Hormones and growth factors – insulin, insulin derived growth factor1 (IGF1), vascular endothelial growth factor (VGEF) estrogen Immune cells and inflammatory factors - Macrophage infiltration, cytokines
, vascular endothelial growth factor (VGEF) estrogen Immune cells and inflammatory factors - Macrophage infiltration, cytokines")
15
Energy Excess and Cancer Clinical and epidemiologic evidence suggests that elevated levels of circulating insulin or C-peptide (cleavage product of proinsulin) are associated with increased risk and/or poor prognosis of endometrial, pancreatic, renal, prostate, colon and pre and postmenopausal breast cancer Data strongly suggests that endogenous hyperinsulinemia may be one obesity-related factor enhancing cancer growth and metastases ( Hursting et al Cancer Prevention Research 2012;5:1260- 1272 )
 are associated with increased risk and/or poor prognosis of endometrial, pancreatic, renal, prostate, colon and pre and postmenopausal breast cancer Data strongly suggests that endogenous hyperinsulinemia may be one obesity-related factor enhancing cancer growth and metastases ( Hursting et al Cancer Prevention Research 2012;5: )")
16
Energy Excess and Cancer High circulating levels of insulin also upregulate the hepatic synthesis of insulin derived growth factor-1 (IGF-1) which is a major endocrine and paracrine regulator of tissue growth and metabolism as it both suppresses apoptosis and initiates cell cycle progression from G1 to S phase. Epidemiologic evidence supports the hypothesis that increased circulating IGF-1 is associated with increased risk and/or worse prognosis for several types of human cancers ( Hursting et al Cancer Prevention Research 2012;5:1260-1272 )
.")
17
Energy Excess and Cancer Vascular Endothelial Growth Factor (VGEF) production is induced by insulin and IGF-1 and mediates cancer cell proliferation and tumor growth by inducing angiogenesis Produced by both adipocytes and tumor cells higher levels of VEGF are seen in obese animals and humans and decrease with weight loss A growing body of evidence in humans suggests strong associations between VGEF levels and aggressive cancers ( Hursting et al Cancer Prevention Research 2012;5:1260-1272)
 production is induced by insulin and IGF-1 and mediates cancer cell proliferation and tumor growth by inducing angiogenesis Produced by both adipocytes and tumor cells higher levels of VEGF are seen in obese animals and humans and decrease with weight loss A growing body of evidence in humans suggests strong associations between VGEF levels and aggressive cancers ( Hursting et al Cancer Prevention Research 2012;5: )")
18
Energy Excess and Cancer Estrogens stimulate cell proliferation and inhibit apoptosis and can also induce VEGF and angiogenesis Estrogens can also be metabolized into DNA-reactive metabolites that potentially induce mutagenesis In postmenopausal women a major contributor to estrogen production is adipose tissue, where the enzyme aromatase converts adrenal androgens into estrogen Tamoxifen, a selective estrogen receptor inhibitor, has been shown to significantly reduce the development of postmenopausal breast cancer ( Hursting et al Cancer Prevention Research 2012;5:1260-1272 )
")
19
Energy Excess and Cancer Leptin: an adipocytokine secreted by adipose tissue. As body fat stores increase, circulating levels of leptin increase. In vitro studies have shown that leptin can stimulate cell proliferation and survival in colon, breast, endometrial and prostate cancer cells. Leptin can modulate tumor growth by increasing the expression of VEGF Adiponectin: an adipocytokine secreted by adipose tissue. As fat stores increase levels of adiponectin decrease. In vitro studies have shown that adiponectin induces apoptosis and inhibits cell growth and proliferation in breast, colon, endometrial and prostate cancer cells. It has also been shown to inhibit angiogenesis by inducing apoptosis of endothelial cells. Higher adiponectin concentrations have been associated with a lower risk of post-menopausal breast cancer and endometrial cancer

20
Energy Excess and Cancer Chronic inflammation has long been associated with cancer development and progression and increases the risk of multiple tumor types Obesity leads to subclinical inflammation in visceral and subcutaneous white fat and is characterized by macrophages surrounding necrotic adipocytes

21
Energy Excess and Cancer Increasing obesity has been positively associated with inflammation Increased adipose tissue produces inflammatory cytokines including tumor necrosis factor (TNF), monocyte chemoattractant protein (MCP1) and C-reactive protein (CRP), all of which enhance local macrophage infiltration Through intracellular signaling pathways inflammatory molecules induce gene expression associated with cell proliferation, apoptosis and angiogenesis, leading to increased proliferation and differentiation, inhibition of apoptosis and induction of angiogenesis. ( Hursting et al Cancer Prevention Research 2012;5:1260- 1272 )
.")
22
Energy Excess and Cancer In mice, tumor cells transplanted into underfed mice did not grow as rapidly as in those fed more abundantly An excess in nutrients causes an imbalance in energy leading to oxidative stress and abnormalities of fatty acid metabolism that foster inflammation and insulin resistance. This results in a number of processes that underlie cancer initiation and promotion including DNA damage, cell division, delayed cell death, an increase in blood vessel formation and cell migration ( An Integrated View of Obesity. Science 318: 928-929 )
.")
23
Energy Excess and Cancer

24
Energy Balance, Obesity and Cancer How many of us are obese? 34.9% of adults over 20 are obese-- defined as a BMI greater than 30 (JAMA. 2014;311(8):806-814) Another third of people are overweight – BMI 25-29.9 That means that fully 2/3rds of the US population is overweight or obese and carries an increased risk of cancer!!
: ) Another third of people are overweight – BMI That means that fully 2/3rds of the US population is overweight or obese and carries an increased risk of cancer!!.")
25
Energy Balance, Obesity and Cancer Is this the new normal?

26
Energy Balance, Obesity and Cancer Is there evidence between obesity and increased risk of cancer?

27
Energy Balance, Obesity and Cancer There is a convincing link of obesity to the following cancers: Endometrial Colorectal Esophageal Kidney Pancreas Post-menopausal breast Gallbladder Liver Thyroid Ovarian Early and aggressive prostate

28
Energy Balance, Obesity and Cancer Lancet 2014;384:755-765

29
Energy Balance, Obesity and Cancer How bad is the problem? It has been estimated that up to 1/3 of cancers are related to overweight or obesity, physical inactivity and/or poor nutrition (AICR/WRCF, Policy and Action for Cancer Prevention 2009)
.")
30
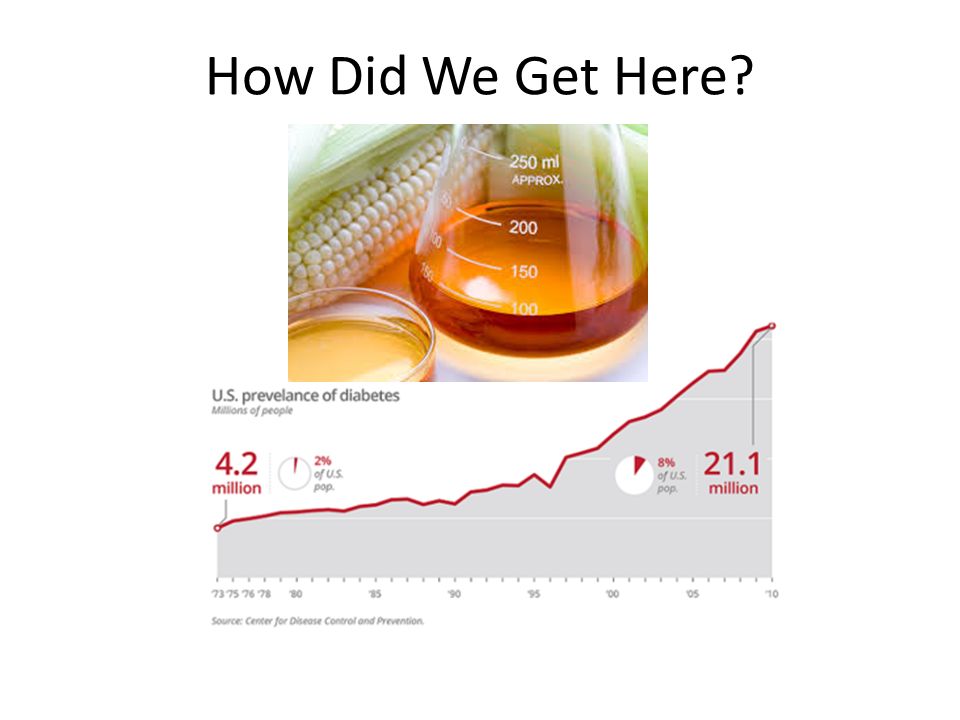
How Did We Get Here? By substituting natural protein, fat and carbohydrate sources for high caloric, poorly nutritious manufactured food, fast food and sugary beverages – THE WESTERN DIET The largest medical disaster of the past 100 years has been the recommendation of the low fat/high carbohydrate diet – a public health experiment which has been an utter and complete failure!!!

31
How Did We Get Here? What happened?? In the 1950’s and 60’s there was an all out war on heart disease and the lipid heart hypothesis was born – the thought that saturated fat and cholesterol were the cause of heart disease. This led to National guidelines (USDA, AHA, NHLBI, NIH) in the 1970’s promoting a low fat/high carbohydrate diet. Let’s see how that worked out…..
 in the 1970’s promoting a low fat/high carbohydrate diet. Let’s see how that worked out…...")
32
How Did We Get Here? Here is what we are eating. Convenient - yes, nutritious – NO!!

33
How Did We Get Here?

37
So the question becomes is the increase in obesity due to increased caloric intake and decreased physical activity (calories in vs calories out) or is it because of the composition of the food we are eating and the biochemical and hormonal response to this food (response to simple carbohydrates and sugar)?? I want you to think about the following statement before you contemplate your answer. We have an epidemic of obese 6 month olds

38
How Did We Get Here? So what happened?? We replaced highly nutritious fats and plant based carbohydrates with sugar and highly refined, nutrient poor processed carbohydrates. Our consumption of protein has stayed about the same. At the same time our caloric consumption increased. Adult males are eating 187 calories more per day and adult females are eating 335 calories more per day than they were 20 years ago. ALL THE EXTRA CALORIES ARE IN THE FORM OF SUGARY BEVERAGES AND PROCESSD CARBOHYDRATES, NOT FAT (in fact fat consumption has decreased).
..")
39
FOODS, TOXINS AND CANCER: IS THERE A LINK? Arsenic: inorganic arsenic is a human carcinogen found in drinking water and there is convincing evidence linking arsenic contamination to an increased risk of lung cancer and possibly skin and esophagus cancer. Coffee: there is no convincing evidence that it increases the risk of pancreas or kidney cancer.

40
FOODS, TOXINS AND CANCER: IS THERE A LINK? Supplements: there is convincing evidence that high dose beta carotene supplements in tobacco smokers increases the risk of lung cancer. No specific vitamin or mineral supplementation is recommended for cancer prevention

41
FOODS, TOXINS AND CANCER: IS THERE A LINK? Processed meat and domesticated red meat: there is convincing evidence for an increased risk of colorectal cancer. Alcohol: there is convincing evidence for an increased risk of mouth, pharynx, larynx, esophageal, colorectal in men and breast cancer in women and liver cancer related to cirrhosis without distinction as to the type of alcoholic beverage consumed.

42
RECOMMENDATIONS FOR CANCER RISK REDUCTION So what do we do? It is really quite simple – we need to eat fewer and more nutritionally dense calories. In many cases we have replaced 30-40% of potentially nutritious foods with SUGAR – a substance with absolutely NO nutritional value. In fact, sugar is a chronic toxin!! RESTRICTION OF ENERGY INTAKE FROM FOOD IS THE MOST EFFECTIVE SINGLE INTERVENTION FOR PREVENTING CANCER IN EXPERIMENTAL ANIMALS!!

43
RECOMMENDATIONS FOR CANCER RISK REDUCTION Limit consumption of energy dense foods and eliminate ALL sugar sweetened and diet beverages as well as all fast food: Energy dense foods are those containing 225-275 kcal per 100g. This includes most processed and fast food. Energy dense processed food and sugary beverages promote weight gain and obesity = =

44
RECOMMENDATIONS FOR CANCER RISK REDUCTION Limit intake of red meat and processed meats: Limit the consumption of domesticated red meat to 18oz per week and try to eliminate all processed meats. Limit consumption of alcohol: No more than 2 drinks per day for men and 1 drink per day for women

45
RECOMMENDATIONS FOR CANCER RISK REDUCTION Non-starchy fruits and vegetables: there is probable evidence that these protect against cancers of the mouth, pharynx, esophagus and stomach with limited evidence for protection against lung, colon, endometrial and ovarian cancers. That being said these foods are high in fiber and nutrients and low in energy density thus being the foundation of any diet.

46
RECOMMENDATIONS FOR CANCER RISK REDUCTION Eat mostly plant based foods: Consume 5 servings of non-starchy vegetables (14 oz) daily as well as 2 servings of fruit, preferably those lower in sugar – berries If eating grains consume unprocessed grains Nuts and seeds: Good source of fiber, essential fatty acids and vitamins and minerals
 daily as well as 2 servings of fruit, preferably those lower in sugar – berries If eating grains consume unprocessed grains Nuts and seeds: Good source of fiber, essential fatty acids and vitamins and minerals")
47
RECOMMENDATIONS FOR CANCER RISK REDUCTION Physical activity: there is convincing evidence physical activity protects against colon cancer and probable evidence that it protects against post-menopausal breast cancer and endometrial cancer.

48
RECOMMENDATIONS FOR CANCER RISK REDUCTION Maintain a lean body mass - BMI between 19 and 25 from childhood through adulthood Be physically active – perform some sort of physical activity equivalent to 30 minutes of brisk walking daily. Avoid sedentary activities such as television watching.

49
RECOMMENDATIONS FOR CANCER SURVIVORS Cancer survivors should follow the recommendations for healthy weight, diet and physical activity as recommended for cancer prevention. Current evidence suggests that there are health benefits from physical activity during cancer survivorship with breast cancer survivorship having been the most studied

50
Energy Balance, Obesity and Cancer In animal models a 20-40% reduction in total energy intake relative to an unrestricted comparison group is one of the most potent and broadly acting dietary interventions for preventing or reversing weight gain and inhibiting cancer in experimental tumor models Hurstig et al; Cancer and Metabolism 2013, 1:10

51
Energy Balance, Obesity and Cancer How does this translate into humans?? CALERIE trial – Comprehensive Assessment of Long Term Effects of Reducing Intake of Energy – preliminary reports indicate that many of the same metabolic and endocrine changes observed in rodents and monkeys are also occurring in humans in response to calorie restriction.

52
Energy Balance, Obesity and Cancer Woman at high risk for breast cancer showed reduction in inflammatory and growth factor signaling pathways with either total caloric restriction or carbohydrate calorie restriction for 2 days/week. Imayama et al; Cancer Research 2012, 72:2314-2326 Each increase in energy intake of 238kcal/day during childhood was associated with a 20% increase in adult cancers unrelated to smoking Frankel et al: BMJ 1998, 316:499

53
Energy Balance, Obesity and Cancer What is the bottom line ?? We are too fat We consume the wrong calories – sugar and refined carbohydrates We consume too many calories – increased caloric consumption mainly as refined carbohydrates and sugar We consume a diet rich in calories but extraordinarily poor in nutrients We are too sedentary We want a pill to make it go away

54
Energy Balance, Obesity and Cancer Is Cancer a Preventable Disease?? The resounding answer is YES. With appropriate dietary intervention, increased exercise, smoking cessation and appropriate vaccinations it has been estimated that up to 60% of cancers could be prevented!!!

55
Energy Balance, Obesity and Cancer ARE WE NEXT ?

56
NUTRITION AND CANCER: BEFORE, DURING AND AFTER In addition to the references quoted in this power point there is a terrific reference on the link between food, nutrition, physical activity and the prevention of cancer: Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective: World Cancer Research Fund and American Institute for Cancer Research 2007 This is the most comprehensive publication on the subject to date – 537 pages worth!

Similar presentations






 75% of your cholesterol is.>")













