Download presentation
Presentation is loading. Please wait.

1
Using Positive Deviance to Improve Patient Experience Aligning Forces for Quality April 12, 2012

2
AF4Q Patient Experience Affinity Group Deborah Roseman AF4Q National Program Office Dale Shaller & Michelle Ferrari Shaller Consulting

3
Jon C. Lloyd, MD, FACS Senior Associate, Positive Deviance Initiative Mike Wenzel Performance Improvement Manager, Allina Hospitals & Clinics

4
Jon C. Lloyd, MD, FACS Senior Associate, Positive Deviance Initiative

5
Enables communities to find and spread their own hidden solutions

6
Solutions to seemingly intractable problems already exist in your hospital/community The people (front line staff) are the gurus- no one else knows what they know about their work. They frequently don’t know what they know or realize the importance of what they do. You can’t “empower” them. You can unleash their power. There’s an approach that enables them to discover and spread what they know & do.

7
Road Map The opportunity The “what” - Evidence based precautions The “how” - PD Primer PD in healthcare So what? Results Then what? Sustainability and spread

9
MRSA HAI Still a National Epidemic HHS 2009 Quality Report Shows Increase In Hospital- Acquired Infections 15 Apr 2010

10
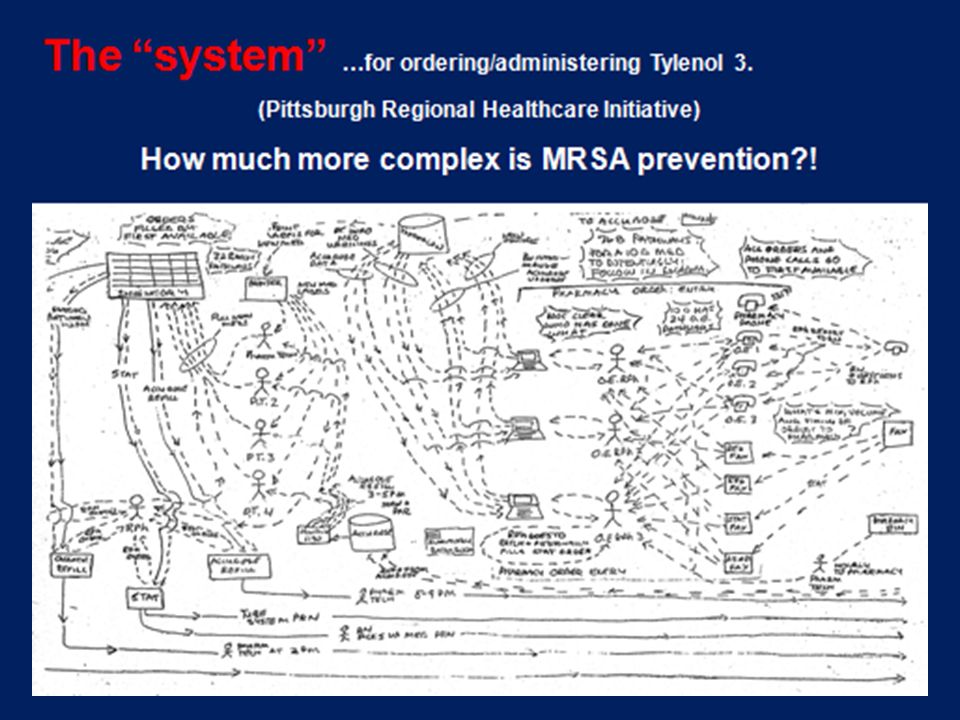
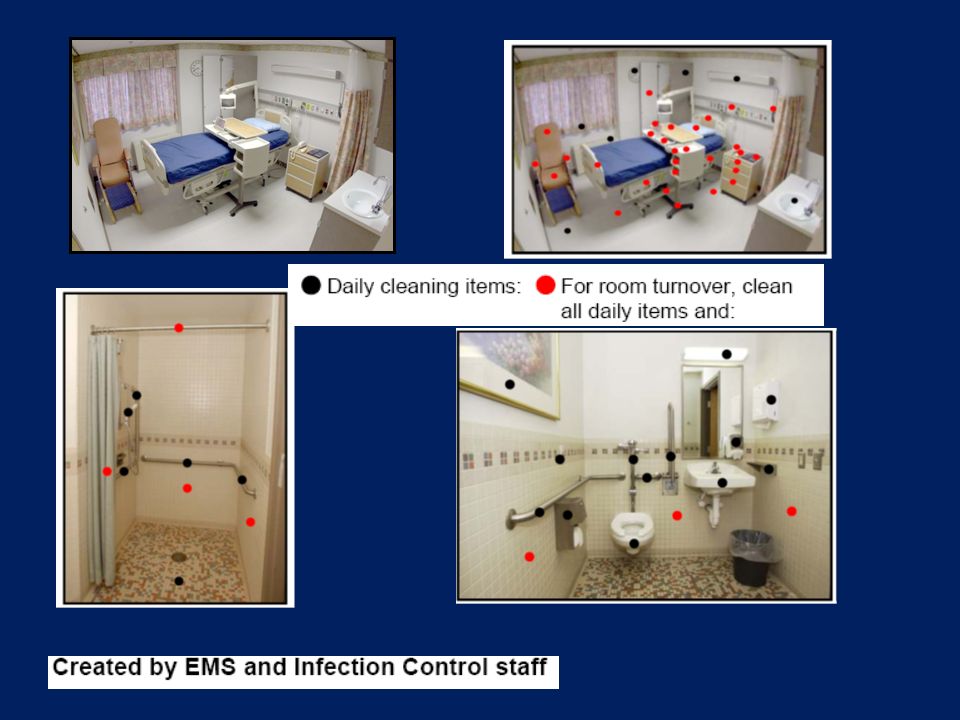
10 “ WHAT” we ALL need to DO (Evidence-based precautions) Identify the reservoir of infected and colonized patients Wash hands before and after every interaction with a patient and before and after putting on gloves Protect clothing from becoming a transmission source by wearing gloves and gown when interacting with an infected or colonized patient Keep equipment from becoming a transmission source by using designated equipment or cleaning Effectively clean the patient care environment How?! HOW?!

12
12 HAI’s: a complex problem requiring behavior and social change Not primarily a knowledge problem. We already know what to do – Hand hygiene and barrier precautions were introduced 160 ago. Resistant pathogens and active surveillance emerged 50 years ago Traditional best practice, industrial approaches, P4P and regulation & enforcement alone either fail outright or tend to achieve modest & frequently transient improvement without spreading within or between healthcare institutions and beyond. Time is ripe for a solution that matches the complexity and nature of the challenge.

13
The P o w e r of Positive Deviance Solutions before our very eyes The Premise: In every community there are certain individuals whose uncommon practices/behaviors enable them to find better solutions to problems than their neighbors who have access to the same resources. (www.positivedeviance.org)

14
Sternins Introduce PD, Vietnam 1991 Childhood Malnutrition 14 www.positivedeviance.org

15
The Positive Deviance Process These are the steps the community follows in the Positive Deviance Process: 1. Define 2. Determine 3. Discover 4. Design 5. Discern (Monitor and Evaluate) 6. Disseminate
 6. Disseminate.")
17
The “Touchers” The people who have direct patient contact and touch them with hands, clothing and equipment are clearly in the best position to know how, when and where (MRSA) transmissions occur in their work area and how to prevent them. *Unlikely suspects found in places rarely visited

18
18 Define Day 1—Kick-Off (2-3 hours) Senior Leader Introduction MRSA overview- Infection rates Personal Stories- Reflection The Vietnam Story- Reflection Opt-in (out) Invitation to Volunteer Meeting
 Senior Leader Introduction MRSA overview- Infection rates Personal Stories- Reflection The Vietnam Story- Reflection Opt-in (out) Invitation to Volunteer Meeting")
19
Determine 19 Day 2—Volunteers Meet The community… Organizes for action Forms Core Group Trains local facilitators Asks, Listens & Invites Acts Measures Feeds back & celebrates

20
20 Discovery & Action Dialogue Ask, then actively listen. The answer is in the room. The people are the gurus.

22
How do you know which patients have MRSA? What do you do to prevent patients in your care from getting MRSA? What are the barriers that keep you from doing it 100 percent of the time? Do you know of anyone who has figured out strategies to overcome these challenges? If so, how? Do you have any ideas about new strategies? What would it take to implement them in this unit? Who is willing to take the next steps?

24
24 Design & Do Front line staff acts on and owns their solutions

25
Heinz leads the way Heinz is the first long term care facility in the nation to focus on the eradication of MRSA. The Veterans, the Healthcare workers and the Center for Disease Control and Prevention –CDC- have joined together to discover the ways that MRSA is acquired and how it can be eliminated permanently from all hospitals nationwide. Darryl Taylor, William Baker, (not pictured) Dwight Morris, Robert Carlyle Prepared by veterans at the VA Heinz hospital in Pittsburgh A Guide to MRSA Keeping America’s Veterans Healthy A Guide to MRSA A simple way to shorten your hospital stay
 Dwight Morris, Robert Carlyle Prepared by veterans at the VA Heinz hospital in Pittsburgh A Guide to MRSA Keeping America’s Veterans Healthy A Guide to MRSA A simple way to shorten your hospital stay.")
26
Somersaulting beyond perceptions Until the Positive Deviance effort was undertaken, the patients playing cards in the Recreation Room did not realize the soap dispenser on the wall was not only for the staff, but for them also. The veterans became aware that playing cards and bingo could be infectious. The rest is history.

27
27 “We dance around in a ring and suppose, while the secret sits in the middle and knows.” Robert Frost

28
28 RO

30
Unit Briefings Staff owned and operated All healthcare specialties and vocations Leaders listen and support Staff reviews their performance data Problems discussed and solved Success celebrated …and all in fifteen minutes

31
31

32
MRSA-HAI Rates- 153 VA Hospitals NEJM 364;15, April 14, 2011 NEJM; April 14, 2011; 364: 1419-1430

33
33 PD/MRSA Prevention Partnership 2012 2006: 6 hospitals funded by RWJF partnered with PDI, Plexus Institute and CDC to prevent MRSA infections 2007: 17 hospitals in Maryland, 6 VA hospitals and 2 health systems in Colombia became partners 2008: 153 VA hospitals joined the partnership 2009: 7 hospitals funded by AHRQ integrate PD & Lean 2010: 12 hospitals in Canada and 1 hospital in Brazil join

34
“We dance around in a ring and suppose, while the secret sits in the middle and knows.” Robert Frost 34

35
35 Acknowledgments Jerry and Monique Sternin, Positive Deviance Initiative Rajiv Jain, MD, VA Pittsburgh Healthcare System (VAPHS) Frontline staff and patients- VAPHS Bob Muder, MD, MS, VAPHS Cheryl Squier, RN, ICP, VAPHS Candace Cunningham, RN VAPHS Cheryl Creen, RN, MSN, VAPHS John A. Jernigan, MD, MS, CDC Curt Lindberg, Plexus Institute Margaret Toth, MD, CQO, Delmarva Foundation Robert Wood Johnson Foundation Beta Site Coordinators and Staff

36
Contacts & Resources Website: www.positivedeviance.org E-mail: contact@positivedeviance.org www.facebook.com/PositiveDeviance Twitter: PDInitiative The Power of Positive Deviance, Pascale, Sternin and Sternin, Harvard Business Press, 2010.

37
Questions?

Similar presentations









 Gloves Gown* Mask* Individuals in Contact Precautions do not require PPE when leaving their.>")












