Download presentation
Presentation is loading. Please wait.

1
Presented by: Courtney Bennett, DNP, PMHNP-BC Brenda Phillips, DNP, PMHNP-BC

2
Demonstrate understanding of neurocognitive disorders. Identify neurocognitive subtypes and specific syndromes. Recognize risk factors and treatment for Delirium. Recognize treatment for Dementia.

3
The content of material presented in this CE activity will not include discussion of unapproved or investigational uses of products or devices.

4
Attention Memory Language Orientation Praxis Problem solving

5
Delirium Mild and Major Neurocognitive Disorder (NCDs)
")
6
KEY POINTS 1. Delirium is a disorder of attention and cognition. 2. It has an abrupt onset and a variable course. 3. It has an identifiable precipitant. 4. 1-year mortality rate is greater than 40%. Read more: Delirium -Psychiatric Disorders- Cognitive Disorders- http://www.health.am/psy/more/delirium/#ixzz2PLzIvyYtDelirium -Psychiatric Disorders- Cognitive Disorders- http://www.health.am/psy/more/delirium/#ixzz2PLzIvyYt

7
The essential feature of Delirium is a disturbance of attention or awareness that is accompanied by a change in baseline cognition that cannot be better explained by a preexisting or evolving neurocognitive disorder (NCD) (DSM-5, p.599)
 (DSM-5, p.599)")
8
May involve up to 50% of hospitalized elderly patients. They become acutely confused, agitated and have an inability to sustain attention. In elderly patients behavior changes are often a first indicator of delirium even in those diagnosed with Dementia.

10
Perceptual disturbances Abnormal psychomotor activity Sleep cycle impairment Emotional instability Prevalence at hospital admission between 14 and 24 % ( source Kaplan and Sadock )
")
11
Fluid and electrolyte disturbances (dehydration, hyponatremia, hypernatremia). Infections (urinary tract, respiratory tract, Drug toxicity or withdrawal Hypoglycemia, hypercalcemia, uremia, liver failure, thyrotoxicosis Low perfusion states (shock, heart failure) Postoperative states, especially in the elderly Medications (Anticholinergic)
 Postoperative states, especially in the elderly Medications (Anticholinergic).")
12
Acetylcholine..deficiency Dopamine.. excess Glutamate excitatory..excess Gaba inhibitory.. excess Serotonin..excess Ammonia secondary to hepatic encephalopathy

13
CABG up to 35% Hip replacement up to 60%

14
According to the DSM-5, to diagnosis delirium the individual should not be in a coma and there should be a level of arousal sufficient for response to verbal stimulation (p. 600).
..")
15
Serum electrolytes (Creatinine, glucose, calcium, CBC, BMP or CMP) Drug Levels (Digoxin, lithium, or quinidine) Urinalysis and urine culture Blood gas Chest x-ray if indicated
 Drug Levels (Digoxin, lithium, or quinidine) Urinalysis and urine culture Blood gas Chest x-ray if indicated")
16
Substance withdrawal delirium Medication-inducted delirium Delirium due to another medical condition Delirium due to multiple etiologies Other specified delirium Unspecified delirium

17
When the underlying cause of delirium is identified, specific treatment is directed towards the medical condition. Last about 7 days Milieu therapy Antipsychotics and benzodiazepines

18
Agitation will usually resolve once underlying illness responsible for Delirium identified and treated. Nonpharmacolgic interventions: Frequent assurance and verbal orientation. Physical restraints: Only use as a last resort

19
Neuroleptic medications Haloperidol (Haldol) (0.5 to 1.0 mg)- Used to control agitation or psychotic symptoms. 30 minute onset of action. Can be administered orally, intramuscularly or intravenously. Monitor for extrapyramidal side effects (EPS) (>4.5mg per day) and QT prolongation with intravenous administration.
 (>4.5mg per day) and QT prolongation with intravenous administration..")
20
Risperidone (Risperdal) (0.5mg every 12 hours) can also be used to treat severe agitation. Atypical antipsychotics have fewer side effects and similar efficacy to haloperidol (Seroquel, Geodon, Risperidone, and Zyprexa).
..")
21
Benzodiazepines It is recommended Benzodiazepines only be used when neuroleptic drugs are contraindicated. Primarily indicated for alcohol and sedative drug withdrawal. Lorazepam (Ativan) (0.5 to 1.0mg)-can be given PO (less restrictive) or IM and has a rapid onset of action (5minutes).
 (0.5 to 1.0mg)-can be given PO (less restrictive) or IM and has a rapid onset of action (5minutes)..")
22
Always monitor for EPS when prescribing any neuroleptic (antipsychotic) medication.
 medication.")
23
65 year old Caucasian male with a diagnosis of Schizophrenia presents with complaints of weird thoughts, hallucinations, and urinary retention when he receives his Duoneb Treatments. He has been stable on his psychotropic medications for some time now. 1.What is the possible cause of his onset of Delirium and why? 2.What type of Delirium would this be?

24
69 year old African American male presents with increased confusion. Family reports episodes of irritability, mood swings, hallucinations and the patient reports feeling depressed. The family reports no sudden life changing events that could have caused the increased confusion. Laboratory results including urinalysis are all within normal limits. The family suspects Alzheimer’s Disease but after screening the patient and interviewing the family the patient does not fit the criteria for Alzheimer’s Disease. Upon completing the assessment, the patient reports he is not sleeping at night due to the neighbors making a lot of noise. One of the family members laughingly states “The way he snores I’m surprised he even hears the neighbors”.

25
73 year old Caucasian male presents with increased delusions, auditory hallucinations, and paranoia. He believes that people are out to kill him and people have been standing outside of his door watching him. The nursing staff reports his psychosis started all of a sudden, fluctuates during the day, and he has become very withdrawn. Upon assessment, you also notice he is now receiving oxygen therapy for low oxygen saturation and skin is grayish in color.

26
77 year old Caucasian male presents with his wife who reports auditory hallucinations, paranoia, and beliefs that people are trying to harm him. She explains that he was in an inpatient psychiatric facility for 28 days for psychosis and was released two weeks ago on antipsychotic meds and his symptoms have not improved. She also reports unexplained weight loss, memory loss, fatigue, progressive loss of hair, and withdrawal that has occurred over the last three months. A review of some of his lab results reveals the following: WBC (4), RBC (3.9), Platelet (375), SGOT (35), SGPT (65), TSH (0.125).
, RBC (3.9), Platelet (375), SGOT (35), SGPT (65), TSH (0.125)..")
27
83 year old African American female presents with a sudden change in mental status and mood. Nursing staff reports she is confused, irritable, refusing care hitting the staff, and believes the nurses are trying to kill her. This is a change from her baseline in which she is usually pleasant and cooperative with staff. A review of some of her labs reveals the following: WBC (9), RBC (3.9), H&H (12 & 38), TSH (0.45), BUN(15), Crea (0.7) Urinalysis: Cloudy urine appearance, WBC urine >6, Leukocytes (+), Squam Epith >10.
, RBC (3.9), H&H (12 & 38), TSH (0.45), BUN(15), Crea (0.7) Urinalysis: Cloudy urine appearance, WBC urine >6, Leukocytes (+), Squam Epith >10..")
28
KEY POINTS 1. Dementia is a disorder of memory impairment coupled with other cognitive defects. 2. It has a gradual onset and progressive course. 3. It may be caused by a variety of illnesses. 4. Dementia predisposes to delirium. Read more: Dementia -Psychiatric Disorders- Cognitive Disorders- http://www.health.am/psy/more/dementia/#ixzz2PLzi0GeaDementia -Psychiatric Disorders- Cognitive Disorders- http://www.health.am/psy/more/dementia/#ixzz2PLzi0Gea

29
In the DSM-5 the term Dementia (newly named entity Major Neurocognitive Disorders; NCD) Slowly evolving cognitive dysfunction. Decline in thinking skills Usually involves memory, personality, information processing

30
Gradual loss of memory Problems reasoning Judgment Disorientation Difficult in learning Loss of language skills Decline in the ability to perform routine tasks Can have changes in personalities and behavior: hallucinations, delusions, agitation, and anxiety.

32
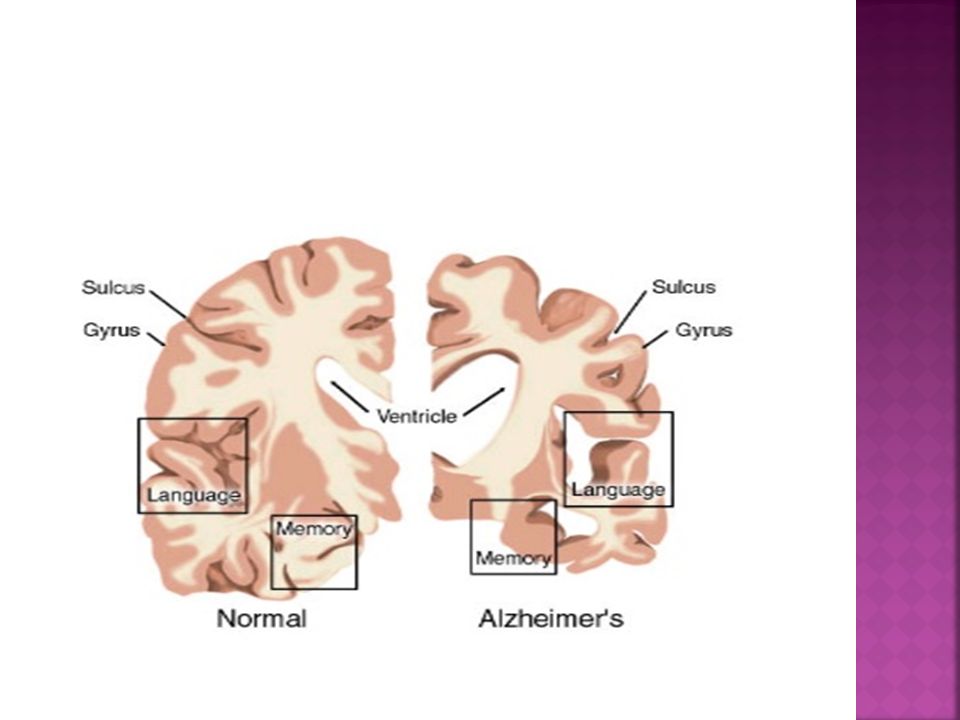
Healthy Brain – NormalOlder Brain – Memory Loss

33
Age is leading risk factor( except for nun study) About 20%of 75 year olds About 50% of those over 85 Duration in years Few effective treatments except cognitive enhancers Behavioral management can use antipsychotics but there is a black box warning
 About 20%of 75 year olds About 50% of those over 85 Duration in years Few effective treatments except cognitive enhancers Behavioral management can use antipsychotics but there is a black box warning")
34
The prevalence of Neurocognitive Disorders varies widely by age and by etiological subtypes. Major NCD-Overall prevalence estimates for dementia (which is largely congruent with major NCD) are approximately 1%-2% at age 65 and as high as 30% by age 85 years. Mild NCD-ranging from 2%-10% at age 65 and 5%-25% by age 85
 are approximately 1%-2% at age 65 and as high as 30% by age 85 years. Mild NCD-ranging from 2%-10% at age 65 and 5%-25% by age 85.")
35
Alzheimers Vascular Dementia with lewy bodies ‘’visual hallucinations Frontotemporal personality and behavior (Pick’s disease ) sexually inappropriate, aggressive Creutzheldt-Jakob disease (CJD)- “mad cow disease”
 sexually inappropriate, aggressive Creutzheldt-Jakob disease (CJD)- mad cow disease")
36
Dementia attributable to Alzheimer’s disease ranges from 60% to over 90% Vascular dementia estimates from 0.2% (65- 70 years age to 16% (80years and older) 20%- 30% are diagnosed with dementia within 3 months of stroke. Lewy bodies range from 0.1%-5% of general elderly population and 1.7% to 30.5% of all dementia cases Frontotemporal-20%-25% occur in older than 65

39
The first problem noticeable is forgetfulness severe enough to affect their work, lifelong hobbies or social life. Confusion Trouble with organizing and expressing thoughts Misplacing things Getting lost in familiar places Changes in personality and behavior

40
Alzheimer’s disease advances at different rates. The symptoms result from damage to the brain’s nerve cells. Gradually gets worse as cells are damaged and destroyed Total Care No one knows exactly what causes Alzheimer’s disease

41
Early Stage- by the time it is obvious someone has AD, it is too late to stop process Unable to recall major events and aspects of their life Recognizable sign- someone gets lost while driving to familiar place like grocery store Preparing a meal become difficulty Trouble concentrating Takes longer doing routine task dressing

42
Middle Stage- ability to perform basic activities of daily living Develops deficits in daily hygiene (brushing teeth, bathing, and eating independently) Forget own name or names of spouse, children and others May not recognize themselves, family, friends, or places Concentration, planning, and understanding more difficult- make bad decisions Mood changes and behavior problems
 Forget own name or names of spouse, children and others May not recognize themselves, family, friends, or places Concentration, planning, and understanding more difficult- make bad decisions Mood changes and behavior problems")
43
Keep a routine One-step directions Limit noise and activity that can be distracting Speak in gentle, low, slow voice Allow them to do what they can as long as they can do it.

44
Late Stage- lose their ability to walk independently Physical rigidity Physical deformities or contractures Death is inevitable until a cure is found

45
Repeat often Allows lots of time to respond Touch in a kind way Use touch with words to communicate Plenty of fluids Read or play music

46
Occurs when clots block blood flow to parts of the brain, depriving nerve cells of food and oxygen Sometimes called “post-stroke dementia” Forgetfulness may or may not be a prominent symptom, depends on whether memory area are affected Difficulty focusing attention and confusion

47
Lewy bodies have been found in several brain disorders, including dementia Symptoms: Memory problems Movement symptoms- stiffness, shuffling walk, lack of facial expression, problems with balance Excessive daytime drowsiness Life threatening to Antipsychotic medication

48
Disease involving Lewy Bodies Damaged and destroyed cells in brain area. Important in controlling movement Usually develop dementia in later stages of the disease

49
Rare disorder chiefly affecting the front and sides of the brain. Progresses more quickly than Alzheimer’s disease and tends to occur at a younger age Changes in personality Judgment Planning and Social skills Show feelings disconnected from the situation

50
Rare, rapidly fatal disease affecting about 1 millions people per year worldwide Usually affects individuals older than 60 Symptoms Impairment in memory, thinking, and reasoning Changes in personality and behavior Depression or agitation tend to occur early Problems with movement may present from the beginning or appear shortly after other symptoms

51
Psychotic features are common in many areas of psychotic symptoms and depression; particularly due to NCDs d/t Alzheimers disease, Lewy body disease, and frontotemporal lobar degeneration Mood disturbances, depression, anxiety and elation may occur Agitation is common in a wide variety of NCDs Apathy is common in mild and major NCD

52
Statistically the older the patient is, the more likely they will develop a cognitive disorder. Most people will be aware of Alzheimer’s disease, as it affects around 4 million people in the USA alone. Alzheimer’s dementia is a cognitive disorder.

53
Organ failure, infection, tumor, kidneys and nerves disorder, side effects of medication and drugs etc. which are some cause of cognitive disorder.

54
Awareness, problem in perception, reasoning, memory and judgment, schizophrenia and delusional disorder these are symptoms of this disorder.

55
Risk factor of this disorder such as advanced cancer or other serious illness, having more than one disease, dementia, and low levels of albumin protein in the blood, infection, taking medications that affect the mind or behavior.

56
Some tips for treating this disorder for example putting the patient in a quiet, well- lit room with familiar objects, placing a clock or calendar where the patient can see it, reducing noise.

57
Donepezil (Aricept) Galantamine (Reminyl) Rivastigmine (Exelon) Memantine (Namenda)
 Galantamine (Reminyl) Rivastigmine (Exelon) Memantine (Namenda)")
58
May slow the progression of mild cognitive impairment to Alzheimer Disease May take up to 6 weeks before any improvement in baseline memory or behavior is evident May slow progression of disease, but does not reverse the degenerative process

59
Aricept (Donepezil)- start 5mg/day; may increase to 10 mg/day after 4-6 weeks Elderly may tolerate lower doses Monitor for bradycardia May lose effectiveness in slowing course of AD after 6 months Once a day dosing Target symptoms- memory loss in AD and other dementias, behavioral symptoms, One of only two drugs indicated for moderate to severe AD
- start 5mg/day; may increase to 10 mg/day after 4-6 weeks Elderly may tolerate lower doses Monitor for bradycardia May lose effectiveness in slowing course of AD after 6 months Once a day dosing Target symptoms- memory loss in AD and other dementias, behavioral symptoms, One of only two drugs indicated for moderate to severe AD")
60
Galantamine (Razadyne)- Initial 4 mg twice daily; after 4 weeks may increase dose to 8 mg twice daily then 12mg after 4 more weeks Syncopal episodes associated with use of medication May slow the progression of mild cognitive impairment to AD Useful for DLB, Vascular Dementia
- Initial 4 mg twice daily; after 4 weeks may increase dose to 8 mg twice daily then 12mg after 4 more weeks Syncopal episodes associated with use of medication May slow the progression of mild cognitive impairment to AD Useful for DLB, Vascular Dementia")
61
Exelon –(Rivastigimine)- Initial 1.5 mg twice daily; increase by 3 mg every 2 weeks titrate to tolerability; maximum dose to 6 mg daily transdermal – Initial 4.6 mg/24hours; after 4 weeks increase to 9.5/24hours; max 13.3/24 Caution with renal, hepatic, and cardiac impairment May interact with anticholinergic agents Treats behavioral and physichological symptoms
- Initial 1.5 mg twice daily; increase by 3 mg every 2 weeks titrate to tolerability; maximum dose to 6 mg daily transdermal – Initial 4.6 mg/24hours; after 4 weeks increase to 9.5/24hours; max 13.3/24 Caution with renal, hepatic, and cardiac impairment May interact with anticholinergic agents Treats behavioral and physichological symptoms")
62
Namenda (Memantine)- NMDA- may takes months before stabilization Initial- 5mg/day; may increase by 5 mg each week; max 10mg twice/day; over 5 mg should be divided. Long half-life Unproven to be effective in mild to moderate AD

63
?????????????????

64
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (5 th ed). Arlington, VA: American Psychiatric Association. Godara, H., Hirbe, A., Nassif, M., Otepka, H. & Rosenstock, A.(2014). The Washington Manual of Medical Therapeutics. St. Louis, MI: Lippincott Williams & Wilkins. Stahl, S. M. (2014). Essential Psychopharmacology Prescriber’s Guide (5 th ed). New York, NY: Cambridge University Press. Townsend (2015). Psychiatric Mental Health Nursing: Concepts of Care in Evidence-Based Practice (8 th ed). Philadelphia, PA: F.A. Davis Company.
. Arlington, VA: American Psychiatric Association. Godara, H., Hirbe, A., Nassif, M., Otepka, H. & Rosenstock, A.(2014). The Washington Manual of Medical Therapeutics. St. Louis, MI: Lippincott Williams & Wilkins. Stahl, S. M. (2014). Essential Psychopharmacology Prescriber’s Guide (5 th ed). New York, NY: Cambridge University Press. Townsend (2015). Psychiatric Mental Health Nursing: Concepts of Care in Evidence-Based Practice (8 th ed). Philadelphia, PA: F.A. Davis Company..")
Similar presentations