Download presentation
Presentation is loading. Please wait.

1
Introduction to the diagnosis and management of common opportunistic infections (Ols) Module 4 Sub module OIs
 Module 4 Sub module OIs")
2
Opportunistic Infections l Pneumocystis carinii pneumonia (PCP) l Penicilliosis l Recurrent pneumonia l Cryptococcus l Toxoplasmosis l Oesophageal candidasis l Mycobacterium Avium Complex (MAC) l Cytomegalovirus (CMV)
 l Penicilliosis l Recurrent pneumonia l Cryptococcus l Toxoplasmosis l Oesophageal candidasis l Mycobacterium Avium Complex (MAC) l Cytomegalovirus (CMV)")
3
Natural course & common clinical manifestations

4
Common opportunistic infections

5
The most common opportunistic infections Division Epidemiology, Department of Communicable Diseases Control, MOPH, Thailand

6
Pneumocystis Carinii Pneumonia (PCP) l Organism l Pneumocystis Carinii l Very common l CD4 count < 200 cells l Absolute lymphocyte count <1200
 l Organism l Pneumocystis Carinii l Very common l CD4 count < 200 cells l Absolute lymphocyte count <1200")
7
Differentiation of bacterial pneumonia & PCP

8
PCP Bacterial pneumonia

9
Pneumocystis carinii pneumonia

10
PCP l Diagnosis –Frequently clinical –Typical symptoms –Response to treatment –Microscopic demonstration of P. carinii in lung secretions/tissue –Culture unavailable

11
PCP l Diagnosis –special methods to obtain specimens are necessary Induced sputum/B.A.L./Biopsy l DDX: –MTB, bacterial pneumonia, fungal pneumonia, lymphoma, KS

12
PCP l Treatment –Trimethoprim-Sulfamethoxazole –drug of choice (iv 15 mg/kg/day or oral 2 DS tablets tid) –3 weeks recommended –Allergy to TMP-SMX –Corticosteroids if severely hypoxic
 –3 weeks recommended –Allergy to TMP-SMX –Corticosteroids if severely hypoxic")
13
PCP l Alternative treatment for allergic patients l (all for 21 days) pentamidine dapsone + trimethoprim clindamycin + primaquine atovaquone –less effective
 pentamidine dapsone + trimethoprim clindamycin + primaquine atovaquone –less effective")
14
PCP l Prognosis: –100% fatal untreated – Level of hypoxaemia best predicts outcome l Secondary Prophylaxis –co-trimoxazole 1-2 tabs daily –Dapsone 100 mg daily –aerosilized pentamidine 300 mg monthly

15
Penicilliosis l Organism: Penicillium marneffei l Endemic area: –SE Asia (Northern Thailand, Southern China, Vietnam, Indonesia, Hong Kong) –3rd most common OI in Northern Thailand l CD4 count < 100 cells
 –3rd most common OI in Northern Thailand l CD4 count < 100 cells")
16
Penicilliosis l Clinical symptoms: –Fever (99%) –papulo-necrotic skin lesions (71%) –weight loss (76%) –anaemia (77%) –lymphadenopathy (58%) –hepatomegaly (51%) –productive cough –lung disease
 –papulo-necrotic skin lesions (71%) –weight loss (76%) –anaemia (77%) –lymphadenopathy (58%) –hepatomegaly (51%) –productive cough –lung disease")
17
Penicilliosis l Diagnosis –Presumptive:microscopy on smear –Definitive: culture –DDx: other disseminated mycobacterial or fungal disease

18
Penicilliosis

20
l Treatment: –amphotericin B IV for 6-8 weeks –amphotericin IV for 2 weeks + itraconazole 400 mg orally daily for 10 weeks l In mild cases: –Itraconazole 400 mg orally daily for 8 weeks

21
Penicilliosis l Prognosis: –high mortality in patients with delayed diagnosis/treatment. l Secondary prophylaxis –Itraconazole 200 mg orally daily for life –> 50% relapse at 1 year without secondary prophylaxis l Primary prophylaxis - not routinely indicated

22
Recurrent Pneumonia l Definition > 1 episode of pneumonia in 12 months l Epidemiology –common in HIV infected patients –S. pneumoniae and H. influenzae at least 20 times more common in HIV –Pneumococcal bacteraemia rate 100 times higher in AIDS v. non-AIDS l Clinical –clinical presentation same as for non-HIV

23
Recurrent Pneumonia Organism l S. pneumoniae H. influenzae l S. aureus enteric gram neg rods l M.TB l Rhodococcus equi l Nocardia asteroides Stage of HIV Infection l early and late l late l early and late l late

24
Recurrent Pneumonia

25
RUL infiltrate caused by Nocardia

26
RUL infiltrate of TB

27
TB with cavitation

28
Disseminated candidiasis

29
Recurrent Pneumonia l Diagnosis –clinical evaluation, sputum smear/culture, CXR, blood culture l Treatment –as per local guidelines for pneumonia in non HIV l Prevention –Co-trimoxazole prophylaxis protects against recurrent pneumonia –Improve immune function with HAART

30
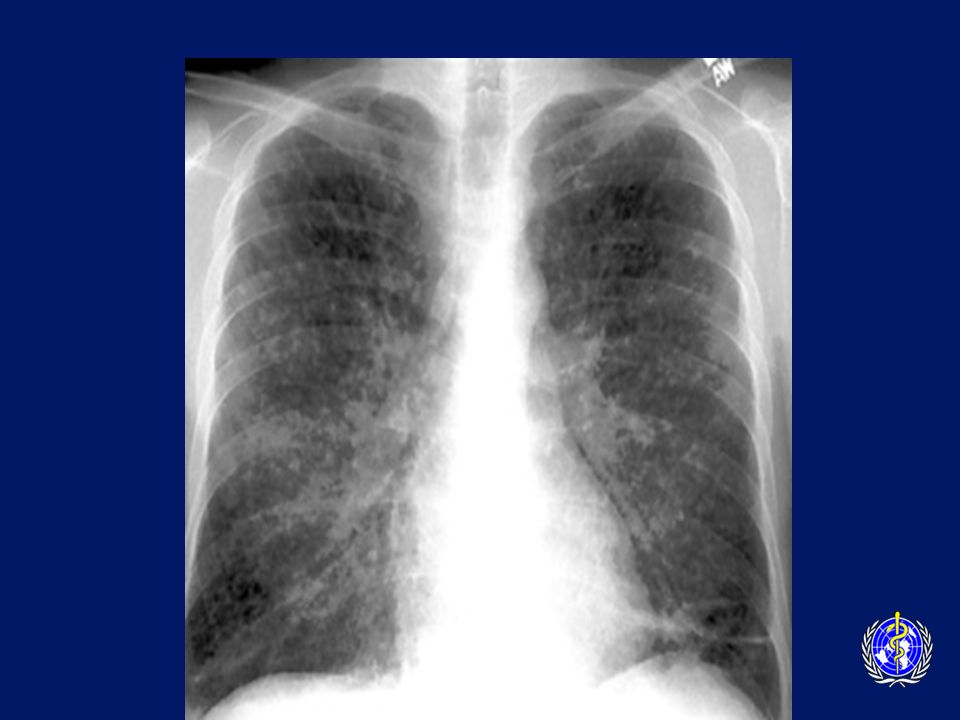
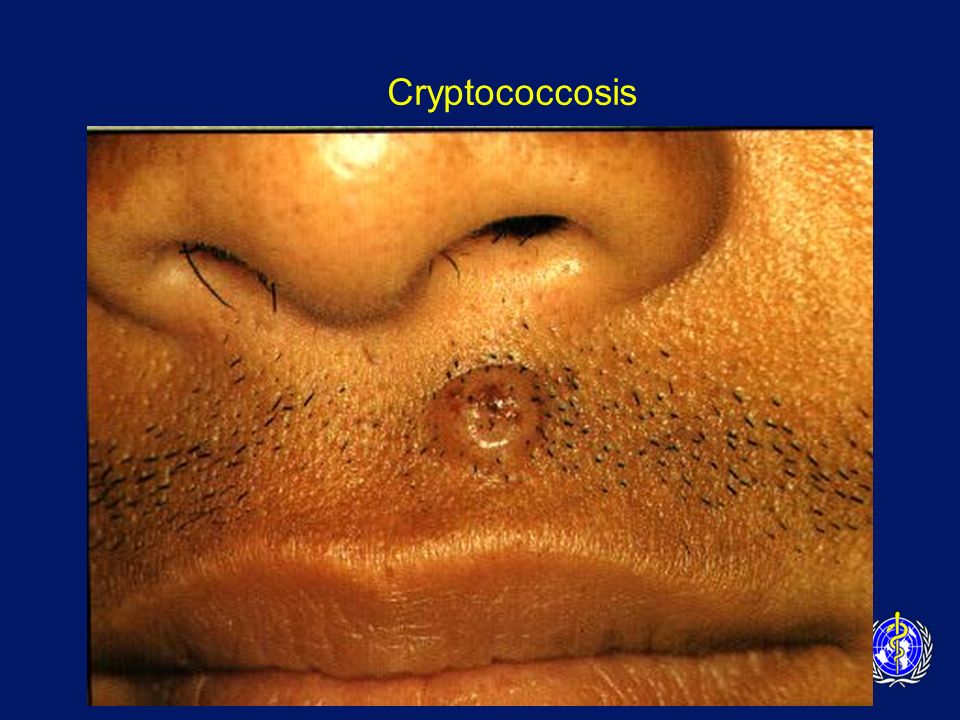
Cryptococcosis l Clinical features –fever –headache –signs of meningism & photophobia –malaise, nausea and vomiting –alteration of mental status

31
Cryptococcosis l Diagnosis –Lumbar puncture - India ink staining –Cryptococcal antigen, and culture –Cryptococcal Ag highly sensitive and specific (CSF and blood) Titre > 1:8 presumptive evidence of infection l Differential Diagnosis –pyogenic meningitis, TB meningitis, toxoplasmosis, neurosyphillis
 Titre > 1:8 presumptive evidence of infection l Differential Diagnosis –pyogenic meningitis, TB meningitis, toxoplasmosis, neurosyphillis")
32
Encapsulated yeast of Cryptococcus neoformans in CSF India ink preparation

33
Cryptococcosis

35
l Treatment of Cryptococcal Meningitis –Induction phase amphotericin B iv daily for 14 days consider adding 5-flucytosine (5-FC) –Consolidation phase fluconazole 400 mg po daily for 8 week
 –Consolidation phase fluconazole 400 mg po daily for 8 week")
36
Cryptococcosis l Prognosis –mortality rates as high as 30% despite therapy l Secondary Prophylaxis –fluconazole 200-400 mg daily –itraconazole 100-200 mg po bid (less effective than fluconazole)
")
37
Toxoplasmosis l Organism: Toxoplasma gondii l Epidemiology: – Cats the definitive hosts –Ingestion of faecally contaminated material –Ingestion of undercooked meat l CD4 count < 100

38
Toxoplasmosis l Clinical Features: –encephalitis the most common manifestation (90%) fever (70%), headaches (60%), focal neurological signs, reduced consciousness (40%), seizures (30%) Constellation of fever, headache, and neurological deficit is classic –chorio-retinitis –pneumonitis –disseminated disease
 fever (70%), headaches (60%), focal neurological signs, reduced consciousness (40%), seizures (30%) Constellation of fever, headache, and neurological deficit is classic –chorio-retinitis –pneumonitis –disseminated disease")
39
Toxoplasmosis l Diagnosis –positive serology with typical syndrome –suggestive CT/MRI scan: multiple, bilateral cerebral lesions; hypodense with ring enhancement –Differential diagnosis –CNS lymphoma, tuberculoma, fungal abscess, cryptococcosis, PML

40
Toxoplasmosis

42
Toxoplasmosis- Response to therapy

43
Toxoplasmosis l Treatment –Empirical therapy reasonable as trial, at least for 2 weeks –Pyrimethamine plus folinic acid plus either sulfadiazine or clindamycin –6 weeks therapy at least, or until 3 weeks after complete scan resolution –Corticosteroids for raised intracranial pressure

44
Toxoplasmosis l Secondary Prophylaxis –Essential because latent (cyst) phase cannot be erdicated –Pyrimethamine plus folinic acid plus sulfadiazine (or clindamycin) –relapse occurs in 20-30% of patients despite maintenance therapy –Improve immunity with HAART
 phase cannot be erdicated –Pyrimethamine plus folinic acid plus sulfadiazine (or clindamycin) –relapse occurs in 20-30% of patients despite maintenance therapy –Improve immunity with HAART")
45
Oesophageal Candidiasis l Organism: Candida yeast l CD4 count < 200 l Clinical symptoms –dysphagia, retrosternal pain –oral thrush in 50-90% –endoscopy ulceration plaques

46
Oesophageal Candidiasis

47
Oesophogeal Candidiasis l Diagnosis –oral thrush and dysphagia sufficient –consider endoscopy if symptoms without oral thrush failure of empirical antifungal therapy –Treatment –Fluconazole 200-400 mg /day until resolved –Long term suppressive therapy if recurrent

48
Mycobacterium Avium Complex (MAC) l Organism: M.avium/M. intracellulare l CD4 count: < 100 cells l Clinical symptoms –fever & night sweats –anorexia & weight loss –Nausea & abdominal pain & diarrhoea –lymphadenopathy –hepatosplenomegaly –anaemia

49
MAC l Diagnosis; –Blood cultures –2 blood cultures will detect 95% of cases –microscopy and culture of bone marrow, lymph nodes l DDx: –MTB, disseminated fungal disease, malignancy

50
MAC Treatment l Option 1 l clarithromycin + ethambutol l Option 2 l clarithromycin + ethambutol + rifabutin l Option 3 l HAART

51
MAC l Prognosis (pre HAART): –Untreated: 4 months –Treated: 8 months l Secondary Prophylaxis –lifelong maintenance required
: –Untreated: 4 months –Treated: 8 months l Secondary Prophylaxis –lifelong maintenance required")
52
CMV Disease l Epidemiology: –a worldwide human herpes virus –3 periods of transmission perinatal, chidhood, reproductive years –in LDC’s, > 90% of children infected by 2 yo l CD4 < 50 l emerging pathogen in SE Asia?

53
CMV Retinitis l Clinical: –field defects –floaters –blurred vision –rapid deterioration in vision l Diagnosis: –typical fundoscopic appearance in a seropositive patient

54
CMV Retinitis

55
Toxoplasma Retinitis

56
Managing CMV retinitis l Treatment –expensive and toxic –maintenance therapy essential –ganciclovir/foscarnet –IVI or intra-vitreal –HAART

57
CMV Disease l Other clinical manifestations of CMV –oesophagitis –colitis –sclerosing cholangitis –encephalitis –polyradiculomyelopathy –adrenalitis –pneumonitis

58
Opportunistic infection prophylaxis in the era of HAART l Stopping rules –Fluconazole after CD4 > 100 for 3 months –Azithromycin after CD4 > 100 for 3 months –Cotrimoxazole after CD4 > 200 for 3 months l Cessation of secondary prophylaxis more controversial l Stopping prophylaxis should always be done by trained HCW on a case per case basis

59
Opportunistic Infections Key Points l Very uncommon in those on successful ARV l Predictable according to CD4 count l Prevention better than cure Secondary ‘ maintenance ’ therapy required l Educate patients

Similar presentations


 in Children>")

















