Download presentation
Presentation is loading. Please wait.

1
Chapter 8 The diseases of digestive system

2
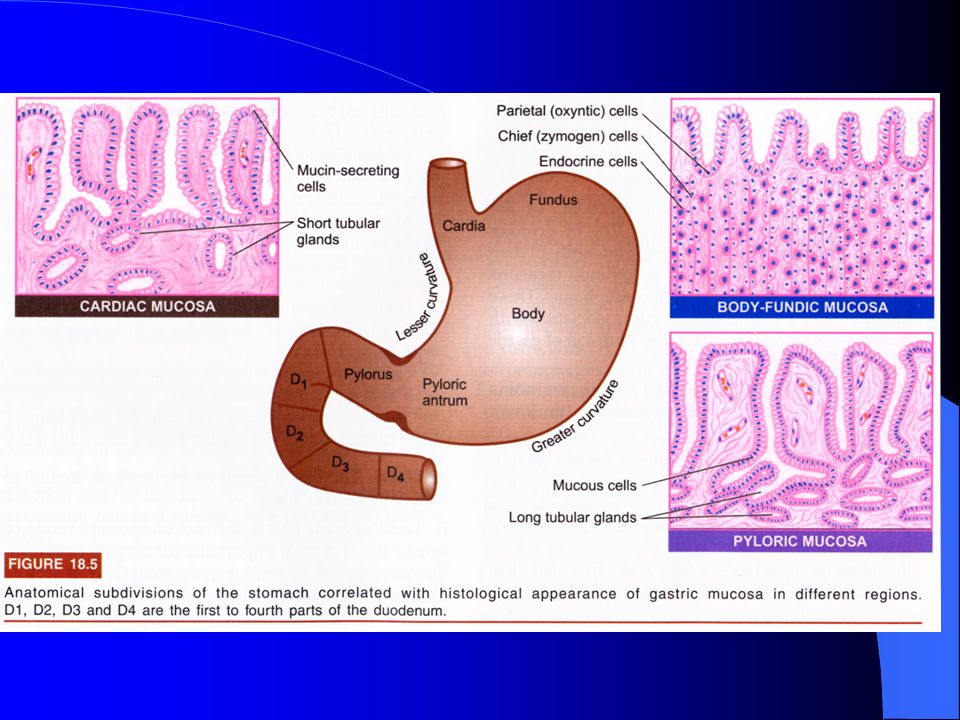
8.1.1 ESOPHAGITIS reflux esophagitis
Definition: esophageal irritation and inflammation due to reflux of gastric secretions into the esophagus Pathologic changes: Eosinophiles, with or without neutrophils, in the epithelial layer Basal zone hyperplasia Elongation of lamina propria papillae Intraepithelial neutrophils are markers of more severe injury Presentation: heartburn and reguritation Complications: bleeding, stricture, bronchospasm and asthma, barrett esophagus

3
2.Barret esophagus Definition: metaplasia of the squamous eosphageal mucosa to a more protective columnar type because of chronic exposure to gastric secretions Cause: gastroesophageal reflux disease Gross: irregular gastroesophageal junction with tongues of red granular mucosa extending up into the esophagus Increased risk of dysplasia and esophageal adenocarcinoma

4
Esophageal carcinoma Squamous cell carcinoma Adenocarcinoma
Epidemiology The most common type of esophageal cancer Males>females; age usually>50 Risk factors Heavy smoking and alchol use Achalasia Plummer-vinson syndrome Tylosis Prior lye ingestion Presentation Often asymptomatic until late in the course Progressive dysphagia Weight loss and anorexia Bleeding Hoarseness or cough (advanced cancers) Diagnosis: endoscopy and biopsy Treatment: surgery Prognosis: poor Adenocarcinoma Arises in the distal esophagus Associated with Barrett esophagus and dysplasia Prognosis: poor
 Diagnosis: endoscopy and biopsy. Treatment: surgery. Prognosis: poor. Adenocarcinoma. Arises in the distal esophagus. Associated with Barrett esophagus and dysplasia. Prognosis: poor.")
7
GASTRITIS

8
inflammation of gastric mucosa
acute gastritis pathogens clear acute inflammation (neutrophils ) chronic gastritis autoimmune bilious duodenal secretion reflex HP infection
 chronic gastritis. autoimmune. bilious duodenal secretion reflex. HP infection.")
9
acute gastritis Definition: acute inflammation, erosion, and hemorrhage of the gastric mucosa due to a breakdown of the mucosal barrier and acid-induced injury Etiology: chronic aspirin or NSAID use/ Alcohol use/ Smoking/ Postsurgery/ Burns/ Ischemia/ Stress/ Uremia/ Chemotherapy Presentation Epigastric abdominal pain Gastric hemorrhage, hematemesis, and melena

10
(1) acute irritated gastritis
1)pathogens:diet 2)lesions:edema, hyperemia, hypersection of mucus, erosion
pathogens:diet. 2)lesions:edema, hyperemia, hypersection of mucus, erosion.")
11
(2) acute hemorrhagic gastritis
1)pathogens: medicines ( aspirin )/alcoholism 2)lesion: usually in fundus and body
pathogens: medicines ( aspirin )/alcoholism. 2)lesion: usually in fundus and body.")
12
(3) acute corrosive gastritis
1)pathogen:engulf acid/ base 2)lesion:stomach wall necrosis →perforation
pathogen:engulf acid/ base. 2)lesion:stomach wall necrosis →perforation.")
13
(4) acute infective gastritis
1)pathogens: purulent bacterium 2)lesions: acute phlegmonous inflammation
pathogens: purulent bacterium. 2)lesions: acute phlegmonous inflammation.")
14
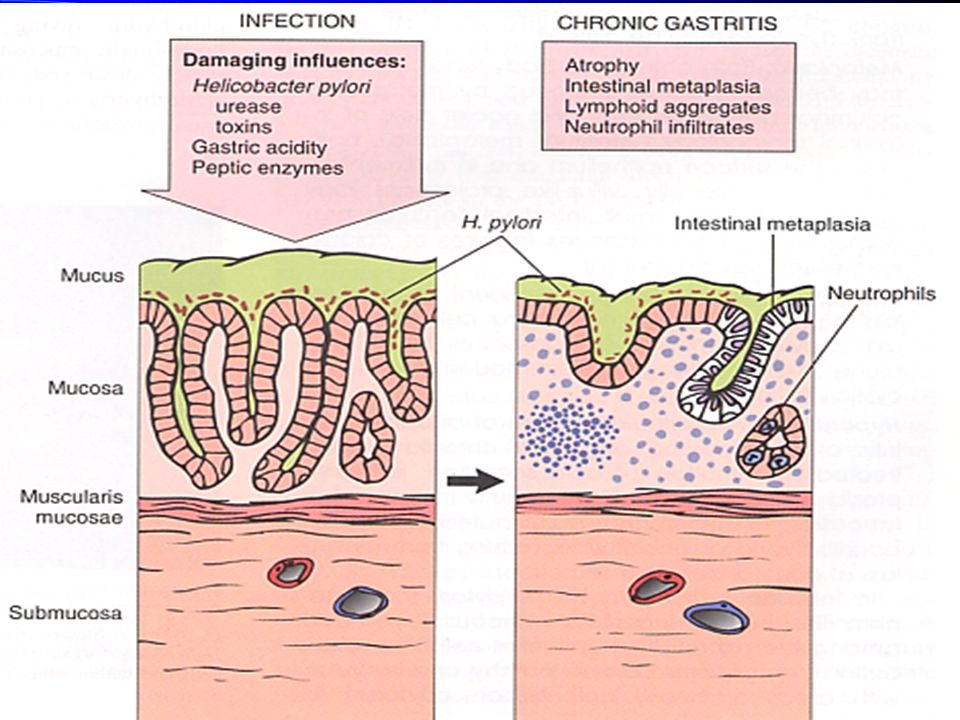
2. chronic gastritis—chronic mucosal inflammatory changes leading eventually to mucosal atrophy and epithelial metaplasia. Pathogenesis HP chronic infection chronic irritation autoimmune reflex of bilious duodenal secretion

17
(1) chronic superficial gastritis (CSG) common
glands in lamina propria intact, lymphocyte/plasma infiltrate in shallow mucosa

18
(2) chronic atrophic gastritis (CAG)
gross:mucosa thin, folds flatten LM within mucosa: lymphocyte, plasma cells infiltrate, aggregate, lymph follicle form mucosal proper glands (gastric glands,cardiac glands, pyloric glands)atrophy or disappear, dilate intestinal metaplasia (replacement of gastric epithelium with columnar and goblet cells of intestinal-type), pseudopyloric metaplasia
atrophy or disappear, dilate. intestinal metaplasia (replacement of gastric epithelium with columnar and goblet cells of intestinal-type), pseudopyloric metaplasia.")
19
chronic atrophic gastritis (CAG)
loss of rugal folds in the body and fundus

21
chronic atrophic gastritis

22
Persisting glands frequently undergo cystic dilation

23
Intestinal metaplasia
replacement of gastric epithelium with absorptive and goblet cells of intestinal-type Variable gland loss and mucosal atrophy, lymphocyte and plasma cell infiltration in the lamina propria.

25
Fundic type (type A) Antral type (type B)
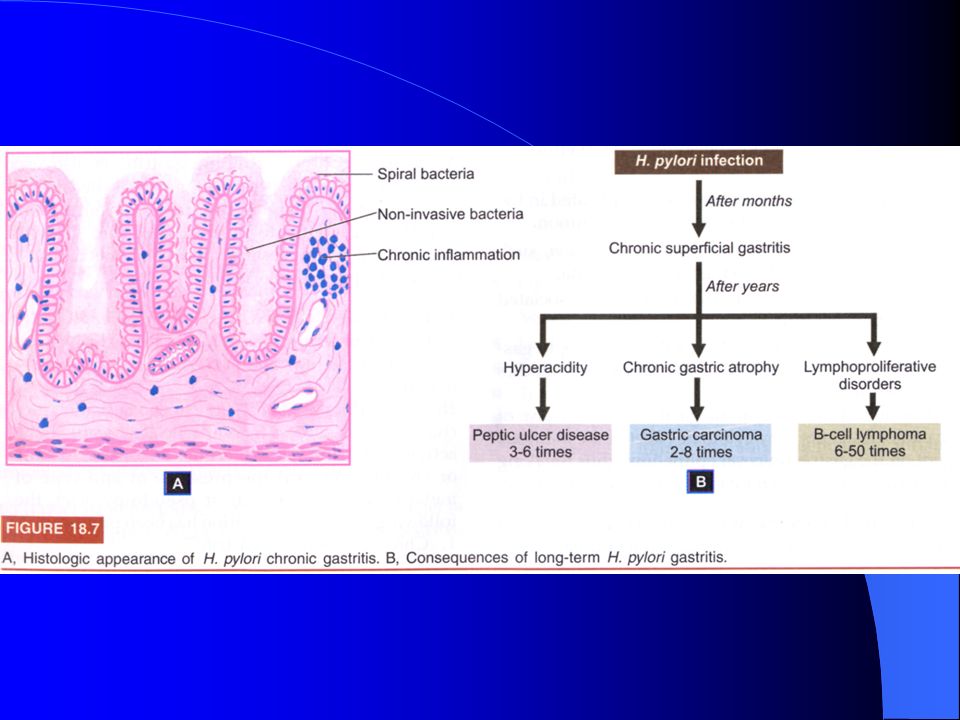
Autoimmune atrophic gastritis rare Involve the body and fundus Autoantibodies to parietal cells / intrinsic factor Loss of parietal cells Decreased acid secretion Increased serum secretion ( G cell hyperplasia) Pernicious anemia (megaloblastic anemia due to lack of intrinsic factor and B12 malabsorption) Helicobactor pylori gastritis Common Helicobactor pylori Curved, gram negative rods Urease producing Risk of infection increase with age Associated with chronic gastritis (type B) Associated with duodenal / gastric peptic ulcers Associated with gastric carcinoma Gross: loss of rugal folds in the body and fundus Micro: mucosal atrophy with loss of glands and parietal cells Chronic lymphoplasmacytic inflammation Intestinal metaplasia foci of acute inflammation Chronic inflammation with lymphoid follicules Increased risk of gastric carcinoma
 Pernicious anemia (megaloblastic anemia due to lack of intrinsic factor and B12 malabsorption) Helicobactor pylori gastritis. Common. Helicobactor pylori. Curved, gram negative rods. Urease producing. Risk of infection increase with age. Associated with chronic gastritis (type B) Associated with duodenal / gastric peptic ulcers. Associated with gastric carcinoma. Gross: loss of rugal folds in the body and fundus. Micro: mucosal atrophy with loss of glands and parietal. cells. Chronic lymphoplasmacytic inflammation. Intestinal metaplasia. foci of acute inflammation. Chronic inflammation with lymphoid follicules. Increased risk of gastric carcinoma.")
26
8.1.3 peptic ulcer Ulcer: defects in the mucosa that penetrate at least into the submucosa, and often into the muscularis propria or deeper Definition: ulcers of the distal stomach and proximal duodenum caused by gastric secretion (hydrochloric acid and pepsin) and impaired mucosal defenses Diagnosis: endoscopy ±biopsy Treatment: acid suppression (H2 blocker, proton pump inhibitor) eradication of H. pylori Complications: hemorrhage: 1/3,common, hematemesis, melena, shock iron deficiency anemia penetration into adjacent organs: 5%, acute diffuse peritonitis , local peritonitis perforation (X-ray: free air under the diaphragm) pyloric obstruction : 2- 3% gastric ulcer: 1%; duodenal ulcer: no
 and impaired mucosal defenses. Diagnosis: endoscopy ±biopsy. Treatment: acid suppression (H2 blocker, proton pump inhibitor) eradication of H. pylori. Complications: hemorrhage: 1/3,common, hematemesis, melena, shock. iron deficiency anemia. penetration into adjacent organs: 5%, acute diffuse peritonitis , local peritonitis. perforation (X-ray: free air under the diaphragm) pyloric obstruction : 2- 3% gastric ulcer: 1%; duodenal ulcer: no.")
27
2)Pathogenesis of peptic ulcer
Increased damage Damaging factors HP NSAIDs smoking alcohol gas. acidity Duo-gast.reflux Peptic acid pepsin hemorrhage p.stenosis Normal mucosa Peptic ulcer healing Impaired defenses Defensive factors ischeria shock Delayed gastric empty Malignant t. Surface mucus secr. HCO- into mucus Mucosal blood flow Epithelia regenera PG Epithelial barrier perforation 2)Pathogenesis of peptic ulcer NSAIDs:非类固醇类抗炎药
Pathogenesis of peptic ulcer. NSAIDs:非类固醇类抗炎药.")
31
gastric ulcer Associated with H. pylori (75%)
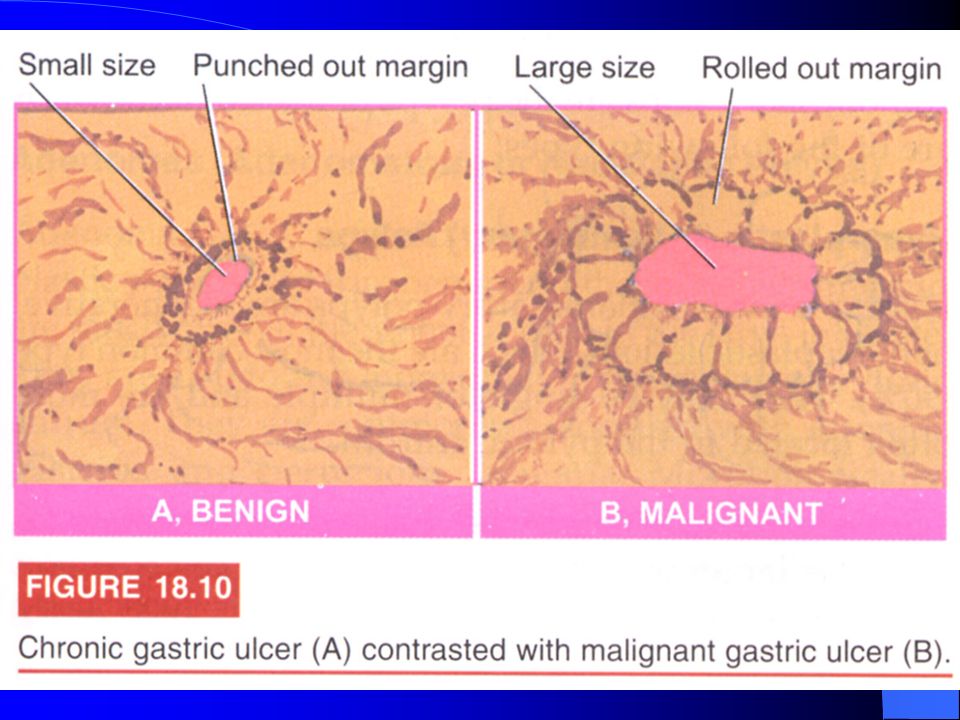
Location: lesser curvature of the antrum Gross: small (<2cm), solitary ulcers round or oval shape sharply demarcated, punched-out ulcers overhanging margins radiating mucosal folds, wheel spokelike fashion base clean, flat, smooth
, solitary ulcers. round or oval shape. sharply demarcated, punched-out ulcers. overhanging margins. radiating mucosal folds, wheel spokelike fashion. base clean, flat, smooth.")
33
gastric ulcer

34
exudate layer:WBC+fibrin necrosis layer granulation tissue scar tissue
LM exudate layer:WBC+fibrin necrosis layer granulation tissue scar tissue Proliferative endocarteritis: inhibit regeneration/ prevent hemorrhage Nodular regeneration of NF: pain Classic presentation: burning epigastric pain, which worsens with eating

38
A渗出层 B:坏死层C:肉芽组织层 D:瘢痕层E:增生性动脉内膜炎 血栓机化再通F:创伤性神经瘤

39
Duodenal ulcer common Location: anterior wall of the proximal duodenum
Classic presentation: burning epigastric pain 1-3 hours after eating, which is relived by food Peptic ulcer of the dudenum. The ulcer is small with a sharply punched-out appearance. Unlike cancerous ulcers, the margins are not elevated. The ulcer base shows a small amount of blood but is otherwise clean.

41
8.2 tumor of digestive system

42
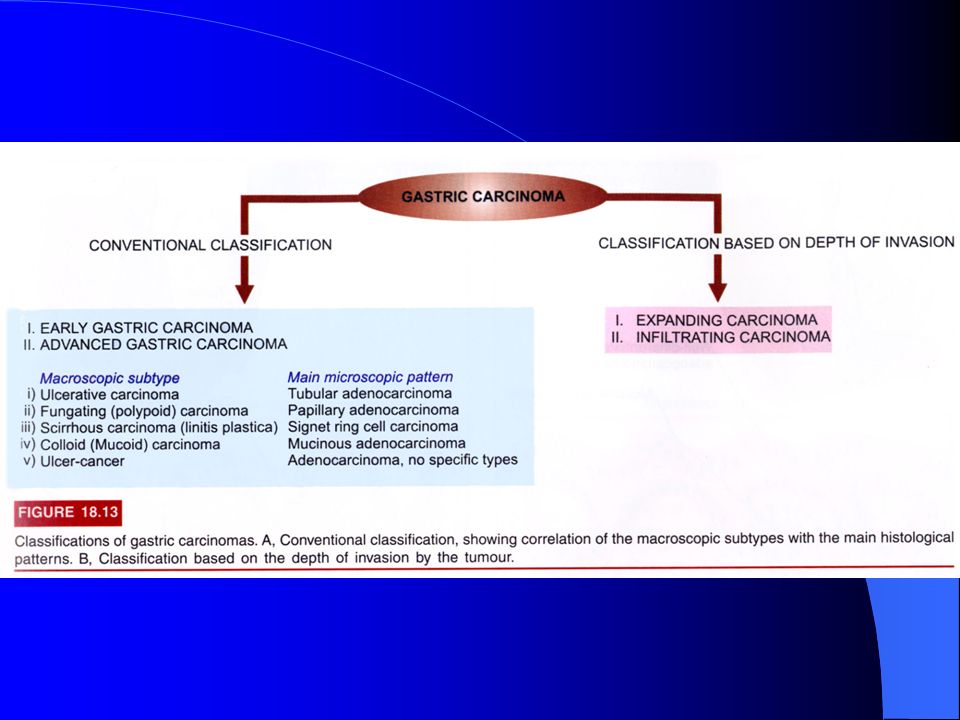
8.2.1 Gastric carcinoma Epidemiology: Japan/ Chile/ Columbia
Risk factors: dietary factors: smoked fish and meats/ pickled vegetables HP infection chronic atrophic gastritis smoking prior subtotal gastrectomy presentation often asymptomatic until late in the course weight loss and anorexia epigastric abdominal pain mimicking a peptic ulcer early satiety occult bleeding and iron deficiency anemia Location: lesser curvature of the antrum

44
Gross Large (>2cm), irregular ulcer Heaped-up margins and a necrotic ulcer base May also occur as a flat or polypoid mass Metastasis Virchow (sentinel) node: left supraclavicular lymph node Krukenberg tumor: spread to the ovary Diagnosis: endoscopy and biopsy Treatment: gastrectomy Prognosis: poor; over all 5-year survival 20%
 node: left supraclavicular lymph node. Krukenberg tumor: spread to the ovary. Diagnosis: endoscopy and biopsy. Treatment: gastrectomy. Prognosis: poor; over all 5-year survival 20%")
45
Intestinal type micro: gland-forming adenocarcinoma Diffuse type diffuse infiltration of stomach by poorly differentiated tumor cells signet-ring cells: nucleus is displaced to the periphery by intracellular mucin linitis plastica: thickened “leather bottle”-like stomach

47
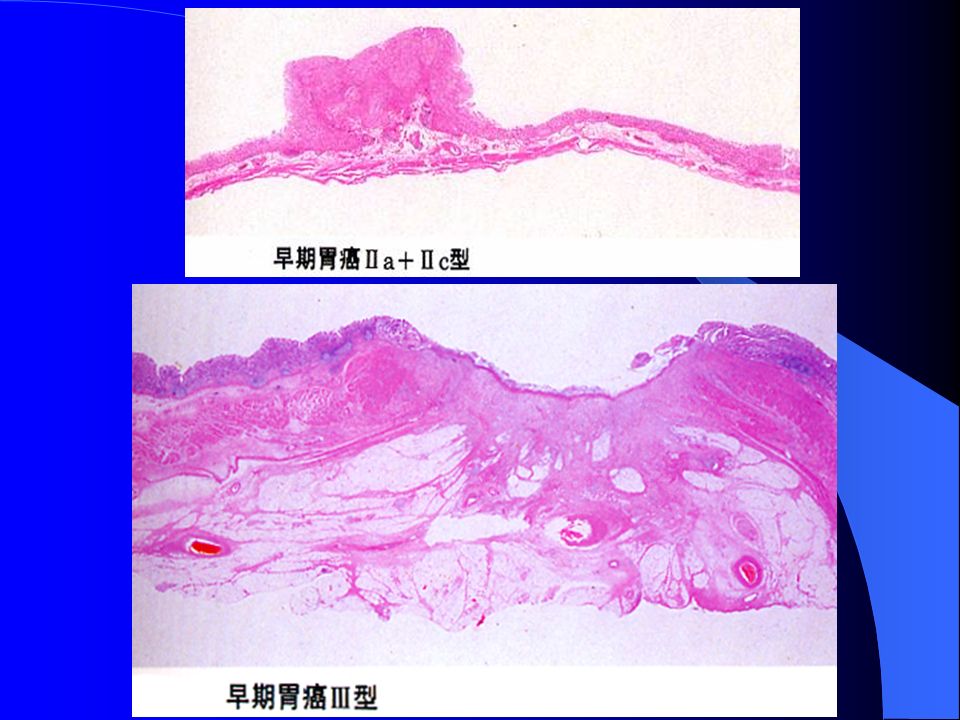
pathologic change (1) early gastric car. (shallow spread car.) concept
confined to the mucosa and submucosa, regardless of the size of area, or absence of perigastric lymph node metastasis

48
protruded type (typeⅠ) >2 times thickness gastric mucosa, polypoid
图9-10 早期胃癌各型模式图 2)gross types protruded type (typeⅠ) >2 times thickness gastric mucosa, polypoid superficial type (type Ⅱ) superficial elevated type(Ⅱa) < 2 times thickness superficial flat type (Ⅱb) superficial depressed ( Ⅱc) depth within mucosa excavated type (type Ⅲ) common, ulcer 早期胃癌各型模式图
gross types. protruded type (typeⅠ) >2 times thickness gastric. mucosa, polypoid. superficial type (type Ⅱ) superficial elevated type(Ⅱa) < 2 times thickness. superficial flat type (Ⅱb) superficial depressed ( Ⅱc) depth within mucosa. excavated type (type Ⅲ) common, ulcer. 早期胃癌各型模式图.")
53
3)histologic types tubular adenocarcinoma>papillary adenocarcinoma>undifferentiated carcinoma
histologic types tubular adenocarcinoma>papillary adenocarcinoma>undifferentiated carcinoma")
54
(2) advanced gastric carcinoma
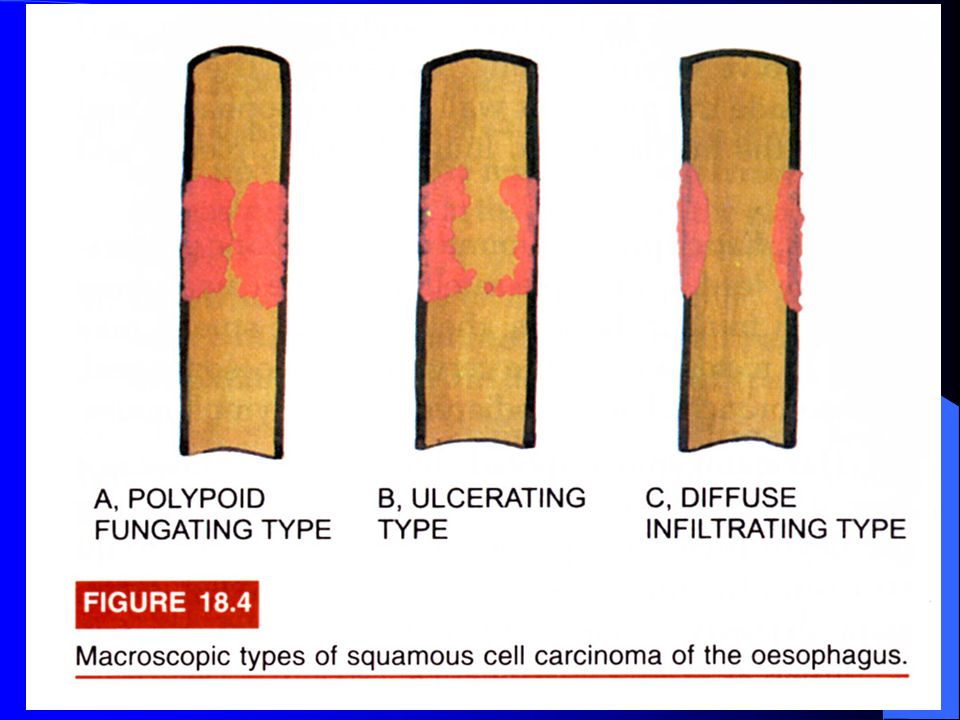
concept:extended below the submucosa into the muscular wall and has perhaps spread more widely gross ① polypoid or fungating type ② ulceration type: erosive crater, D>2.5cm ③ infiltrating type:(Linitis plastica)
")
56
3)histologic types: papillary adeno.,tubular adeno., mucous adeno., signal cell car., undifferentiated car. Lauren:intestine type, diffuse type

59
fungating type

64
ulceration type (the ulcer is large with irregular, heaped-up margins
ulceration type (the ulcer is large with irregular, heaped-up margins. There is extensive excavation of the gastric mucosa with a necrotic gray area in the ddepest portion.

65
ulceration type

66
infiltrating type (a broad region of the gastric wall, or the entire stomach, is extensively infiltrated by maglinancy. The rigid and thickened stomach is termed a leather bottle stomach, or linitis plastica.)
.")
67
Gastric adenocarcinoma (gland formation by malignant cells, which are invading the muscular wall of the stomach.)
")
68
Gastric mucous adenocarcinoma

69
Gastric signet cell carcinoma (permeate the mucosa and wall as scattered individual “signet-ring” cells or in small clusters.)
")
70
Gastric undifferentiated carcinoma

71
4)spread pathways ① direct spread:liver, pancreas ② lymphatic metastasis:main pathways Virchow lymph nodes ③ hematogenous metastasis: liver/ lung/ bone/ brain ④ seeding: abdominal cavity, peritonaeum, ovary—Krukenberg tumor

Similar presentations



























>")
![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")




>")
 Dr. Gehan Mohamed Dr. Abdelaty Shawky.>")







 Stomach ulcer or peptic ulcer is the damage of the protective layer (lining) of stomach or gastrointestinal tract It may be.>")