Download presentation
Presentation is loading. Please wait.

1
VCU DEATH AND COMPLICATIONS CONFERENCE

2
Introduction Complication Return to OR for scrotal hematoma Procedure Laparoscopic right inguinal hernia repair Primary Diagnosis Right inguinal hernia

3
Clinical History 31yo m with large right inguinal hernia since 2007. The hernia causes discomfort and limits activity. He has no obstructive symptoms, no fevers. The pt states that the hernia has always been easily reducible, but has become more uncomfortable in recent months. He is a smoker since age 12, and has a chronic cough. No other significant medical or surgical history.

4
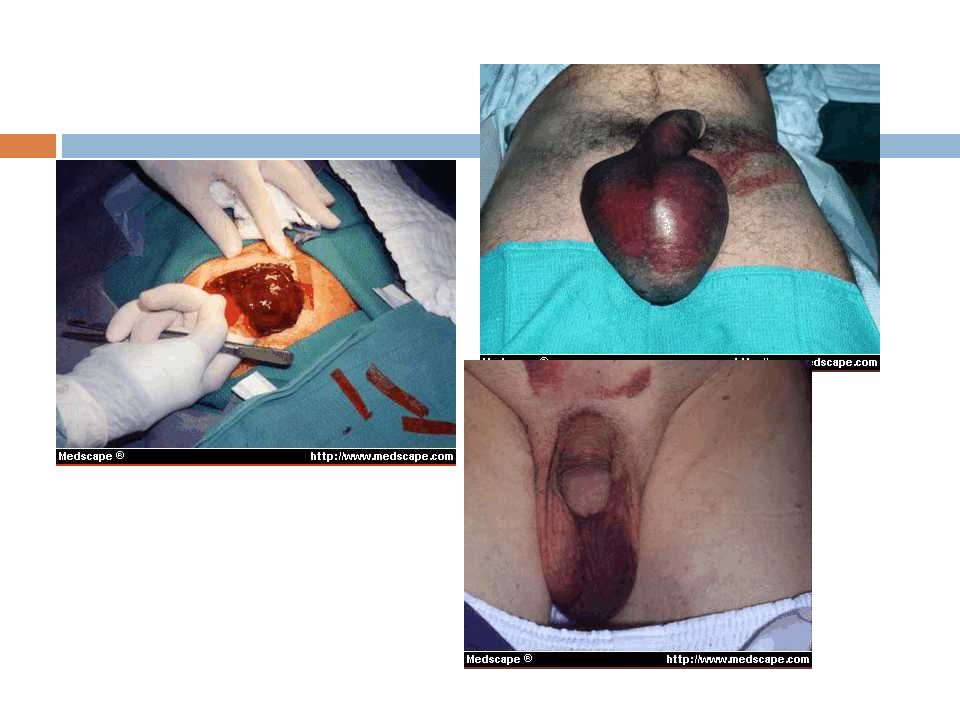
Clinical History Pt taken to the OR for laparoscopic TAP procedure. Within two hours after surgery, the right scrotum was enlarged, tense and tender. Pt taken back to OR emergently for groin exploration, evacuation of hematoma, evaluation of testicle by urology, placement of penrose drains, and closure. Penrose drains removed on POD#3 Pt discharged home on POD#4

5
MEDIALLATERAL

7
Analysis Was the complication potentially avoidable? – Yes. Not doing the surgery, possibly changing technique or leaving a drain Would avoiding the complication change the outcome for the patient? – Yes. Shorter hospital stay, less pain/discomfort, avoid risk of additional anesthesia and reoperation. What factors contributed the complication? – Extensive blunt dissection without electrocautery

8
Hematocele after Herniorrhaphy Hematocele is an accumulation of blood in the tunica vaginalis testis

10
65 yo presents with nonreducible mass in the right scrotum10 days post right inguinal herniorraphy US: multilocular, septated mass Tagged red cell scan c/w ischemia in the right testicle Immediate surgical exploration indicated Hematoma evacuated, hematocele excised through a groin incision Penrose drain placed through separate incision, exiting scrotum at most dependent point and sutured to skin Penrose removed POD#2 Hospital physician, 1999

11
Rare; testicular infarction more common U/S of testicle may not rule out testicular ischemia; flow doppler or Technicium 99 tagged red cell scan should be done Early surgical exploration for suspected hematocele to prevent/alleviate testicular compression Surgical recommendations: sharp division of cremasteric muscle fibers, incision and spread without tearing; avoiding blunt dissection reduces trauma to panpiniform plexus; if hernia sac is strongly adherent to spermatic cord, free only the proximal end of the sac and incise the remainder; avoid dissection of the spermatic cord beyond the pubic tubercle Patient instructions regarding post operative pain and swelling, color change

12
Early detection of hematocele and other causes of testicular ischemia is critical to avoid orchiectomy Swelling should be nonenlarging, without color change, limited to the vicinity of the incision, and noticable only on close inspection

13
Complications in groin hernia surgery and the way out. J Min Access Surg 2006;2:174-7, Symposium Lecture Chowbey PK, Pithawala M, Khullar R, Sharma A, Soni V, Baijal M. Seroma / hematoma after lap inguinal hernia repair: Indicence 5-25% More common after large indirect hernia repair. Most resolve spontaneously over 4-6 weeks. Seroma can be avoided by minimizing dissection of the hernial sac from the cord structures Some surgeons put in a drain if there is excessive bleeding or after extensive dissection

14
Vascular injury The incidence of vascular injury in laparoscopic inguinal hernia repair has been documented to be about 0.5-1 % and inferior epigastric artery is the one most commonly traumatized. Injury to Iliac Vessels: Chances of Mortality Inferior Epigastric Vessel: Hematoma Iliopubic vein and artery which traverse the lacunar ligament: Hematoma Injury to Spermatic vessels: Postoperative scrotal hematoma

16
Postoperative hematoma following inguinal herniorrhaphy: patient characteristics leading to increased risk Mayo Clinic, Rochester, MN Hernia (2008) 12:261–265 Case control study, 53 patients with groin hematomas matched with 106 age and gender matched controls. No significant difference based on location, type of inguinal hernia, technique (open sutured, open mesh, laparoscopic) Coumadin usage (P < 0.001), valvular disease (P < 0.001), atrial fibrillation (P = 0.02), vascular disease (P = 0.04), blood abnormalities (P = 0.02), and previous bleeding episodes (P = 0.02) as significant factors Only preoperative Coumadin usage was important in multivariate analysis Conclusion: perioperative management of anticoagulation in patients undergoing inguinal herniorrhaphy
 Coumadin usage (P < 0.001), valvular disease (P < 0.001), atrial fibrillation (P = 0.02), vascular disease (P = 0.04), blood abnormalities (P = 0.02), and previous bleeding episodes (P = 0.02) as significant factors Only preoperative Coumadin usage was important in multivariate analysis Conclusion: perioperative management of anticoagulation in patients undergoing inguinal herniorrhaphy.")
18
Laparoscopic techniques versus open techniques for inguinal hernia repair (Review) McCormack K, Scott N, Go PM, Ross SJ, Grant A, Collaboration the EU Hernia Trialists Chochrane Library, 2008 Objectives: To compare minimal access laparoscopic mesh techniques with open techniques. Search strategy: MEDLINE, EMBASE, and The Cochrane Central Controlled Trials Registry were searched for relevant randomized controlled trials. Data: 41 eligible controlled trials with a total of 7161 randomized to laparoscopic or open repair. Duration of follow up was 6 to 36 months. Conclusions: Longer operation times; higher risk of rare serious complications (bladder, vascular injuries). Faster return to usual activities; less persisting pain and numbness. Hernia recurrence not different to open mesh methods. Reduced hernia recurrence by 30-50% related to the use of mesh rather than the method of mesh placement. No difference in hematoma formation.
. Faster return to usual activities; less persisting pain and numbness. Hernia recurrence not different to open mesh methods. Reduced hernia recurrence by 30-50% related to the use of mesh rather than the method of mesh placement. No difference in hematoma formation..")
19
Laparoscopic Inguinal Hernia Repair Surgical Clinics of North America 2008, 88 (157-178) Review of current literature on laparoscopic inguinal hernia repair techniques Indications Recurrence after open repair Bilateral Diagnosis of inguinal hernia is uncertain Pts eager to return to normal activity more quickly Contraindications Comorbidities Recurrence from prior laparoscopic repair Strangulated hernia Prior or planned pelvic surgery Incarceration is not considered a contraindication, but makes the operation more difficult, requires significant experience
 Review of current literature on laparoscopic inguinal hernia repair techniques Indications Recurrence after open repair Bilateral Diagnosis of inguinal hernia is uncertain Pts eager to return to normal activity more quickly Contraindications Comorbidities Recurrence from prior laparoscopic repair Strangulated hernia Prior or planned pelvic surgery Incarceration is not considered a contraindication, but makes the operation more difficult, requires significant experience")
20
More data Mesh use, regardless of approach, has results superior to primary sutured repair Post operative complications not significantly different between open and laparoscopic Urinary retention, groin hematoma, neuralgia, groin pain, testicular problems, wound infection, mesh complications Recurrence rates vary 0.4-0.7 % for TAPP and TEP respectively (1994 study) Most single institution, randomized trials 5% SCUR trial European metaanalysis showed not difference in recurrence VA trial 10% laparoscopic, 5% open Depends heavily on surgeon experience, technique Declining with overall improvement in technique, surgeon experience
 Most single institution, randomized trials 5% SCUR trial European metaanalysis showed not difference in recurrence VA trial 10% laparoscopic, 5% open Depends heavily on surgeon experience, technique Declining with overall improvement in technique, surgeon experience")
21
Take home points Avoid inguinal hernia repair in anticoagulated patients Limit blunt dissection, use sharp dissection; incise hernia sac if stuck to the cord Early recognition and surgical exploration for massive or expanding scrotal hematoma, especially if under pressure Evacuation of hematoma and evaluation of testicle for ischemia Orchiectomy if testicle is not viable Proper post op instructions to patient for hematoma recognition Not a reason to avoid laparoscopic repair but a reason to be careful

Similar presentations