Download presentation
Presentation is loading. Please wait.

1
Electrophysiology (Conduction System of Heart)
بسم الله الرحمن الرحيم Electrophysiology (Conduction System of Heart) Dr. Mohammed Sharique Ahmed Quadri Assistant Prof. physiology Al maarefa college
 Dr. Mohammed Sharique Ahmed Quadri. Assistant Prof. physiology. Al maarefa college.")
2
Objectives Identify the components of conducting system of heart .
Know the sequence of conduction of impulse in the heart Recognize the concept associated with pacemaker Appreciate the role of ANS in controlling rate of generation and conduction of impulse Recognize the difference between A.P of SA Node and ventricular muscle fiber

3
Electrical Activity of Heart
Heart beats rhythmically as result of action potentials it generates by itself (Autorhythmicity) Two specialized types of cardiac muscle cells Contractile cells( atrial & ventricular muscles 99% of cardiac muscle cells Do mechanical work of pumping Normally do not initiate own action potentials Auto rhythmic cells ( conductive tissue ) Do not contract Specialized for initiating ( excitation)and conducting action potentials responsible for contraction of working cells
 Two specialized types of cardiac muscle cells. Contractile cells( atrial & ventricular muscles. 99% of cardiac muscle cells. Do mechanical work of pumping. Normally do not initiate own action potentials. Auto rhythmic cells ( conductive tissue ) Do not contract. Specialized for initiating ( excitation)and conducting action potentials responsible for contraction of working cells.")
4
Conducting Tissues of the Heart (autorhythmic cells)
APs spread through myocardial cells through gap junctions. Impulses cannot spread to ventricles directly because of fibrous tissue. Conduction pathway: SA node. AV node. Bundle of His. Purkinje fibers.

5
Specialized Conduction System of Heart

6
Conducting Tissues of the Heart
Sinoatrial Node (SA node) Specialized region in right atrial wall near opening of superior vena cava Pacemaker of the heart INTERNODAL FIBERS Internodal Fibers – Anterior, Middle and Posterior [Bachman, Wenchkeback, Thorel]. Atrioventricular Node (AV node) Small bundle of specialized cardiac cells located at base of right atrium near inter atrial septum.
 Specialized region in right atrial wall near opening of superior vena cava. Pacemaker of the heart. INTERNODAL FIBERS. Internodal Fibers – Anterior, Middle and Posterior [Bachman, Wenchkeback, Thorel]. Atrioventricular Node (AV node) Small bundle of specialized cardiac cells located at base of right atrium near inter atrial septum.")
7
Conducting Tissues of the Heart
Bundle of His (atrioventricular bundle) It is a tract of specialized cardiac cells that originate at AV Node and passes through the fibrous ring and enters interventricular septum Divides to form right and left bundle branches which travel down septum, curve around tip of ventricular chambers, travel back toward atria along outer walls NOTE – Lt Bundle Branch has 2 fascicles Left Anterior Fascicle and Left Posterior Fascicle. Purkinje fibers Small, terminal fibers that extend from bundle of His and spread throughout ventricular myocardium
 It is a tract of specialized cardiac cells that originate at AV Node and passes through the fibrous ring and enters interventricular septum. Divides to form right and left bundle branches which travel down septum, curve around tip of ventricular chambers, travel back toward atria along outer walls. NOTE – Lt Bundle Branch has 2 fascicles Left Anterior Fascicle and Left Posterior Fascicle. Purkinje fibers. Small, terminal fibers that extend from bundle of His and spread throughout ventricular myocardium.")
8
What is AutoRhythmicity ?
Cardiac autorhythmic cells do not have stable resting membrane potential instead they show PACE MAKER POTENTIAL Membrane potential slowly depolarizes between action potential until threshold is reached. This spontaneous depolarization to threshold is known as PACE MAKER POTENTIAL

9
AUTORHYTHMICITY( PACE MAKER POTENTIAL)
")
10
Cause of Prepotential Na+ going inside ↓ K+ going outside
Ca++ going inside After Pre-potential we get Depolarization and Repolarization Cause of Depolarization - Ca++ going inside Cause of Repolarization - K+ going outside

11
S A NODE POTENTIAL PHASE 4 = Prepotential PHASE 0 = Depolarization
Repolarization

13
CONDUCTIVE TISSUE Why SA-Node is a Pace-maker?
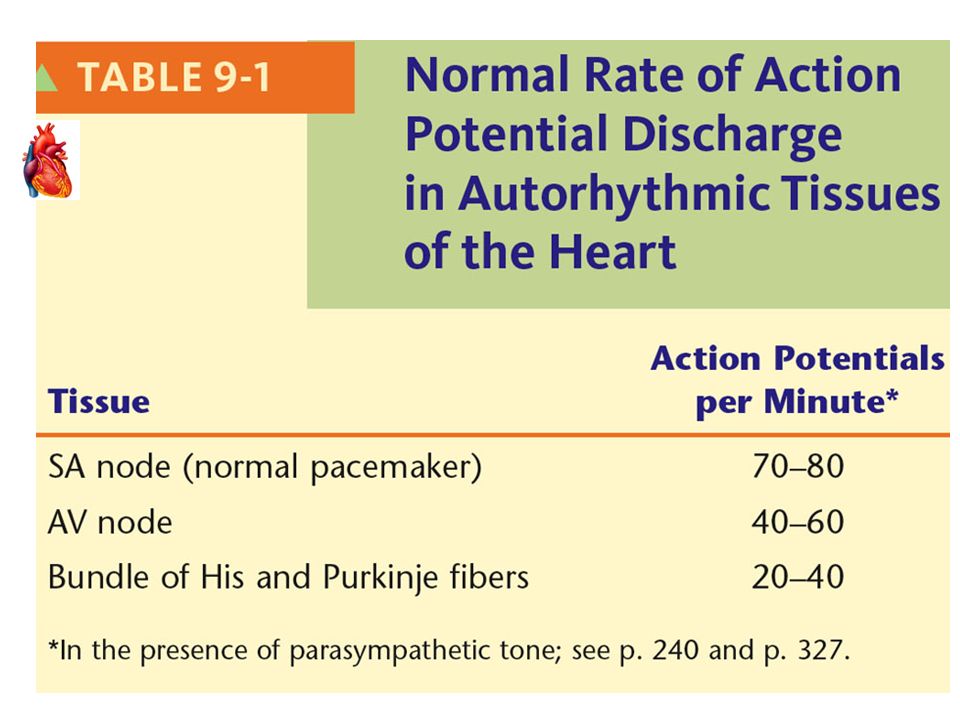
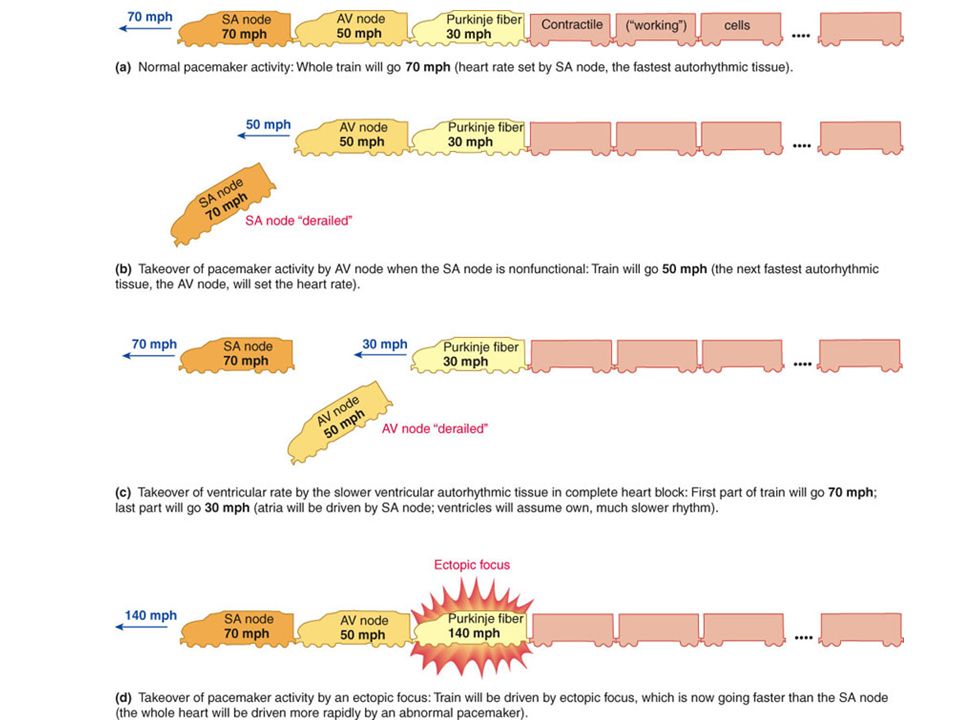
Because its discharge rate is high 70-80/min. This action potential/min drive rest of the heart, therefore, it is known as pace-maker of the heart.

14
CONDUCTIVE TISSUE Other auto - rhythmic tissue are firing at slow rate. They can work as pace-maker, if SA-Node is not functioning e.g. if AV Node takes over as pace-maker, heart rate will be about 50/min. Any pace-maker other than SA-Node is called ‘Ectopic Pace-maker’. ( associated with organic heart disease or lack of sleep, anxiety, excess caffeine, nicotine)
")
16
APPLIED – HEART BLOCKS Sino-atrial block: The sinus node fires but the stimulus does not excite the atria because it is blocked at the junction between the two. AV junctional block: The blocks at the level of the AV junction are classified according to the severity of the block.

17
APPLIED – HEART BLOCKS FIRST DEGREE HEART BLOCK – Every impulse is conducted but very slowly, therefore, there is increase in conduction time [we can see on ECG]. SECOND DEGREE HEART BLOCK – Some impulses are conducted and other are not conducted.

18
APPLIED – HEART BLOCKS THIRD DEGREE HEART BLOCK – Complete heart block, no conduction occurs from SA Node to the ventricle through AV node, therefore, atrial rate is separate [75/min] from the ventricular rate which follows the Purkinje fibers and is about 30/min. IMPORTANT If ventricular rate is very slow e.g. complete heart block, we need artificial pace-maker [implanted device which generates impulse].

19
APPLIED – HEART BLOCKS Bundle Branch block: Conduction at one of the branches become blocked. The wave of excitation spread from the intact branch to depolarize the whole ventricle, which take longer time than if both branches are intact. Right bundle branch block. Left bundle branch block.

20
Control of Excitability by ANS

21
SA NODAL POTENTIAL & CHANGES

22
Epinephrine & Norepinephrine
Effect 0f Sympathetic and parasympathetic Stimulation on Prepotential (Pace Maker Potential) Epinephrine & Norepinephrine (Adrenaline and Noradrenaline) causes Prepotential to occur faster therefore increase the heart rate Acetylcholine causes Prepotential to occur at slow rate therefore decrease the heart rate
 Epinephrine & Norepinephrine. (Adrenaline and Noradrenaline) causes Prepotential to occur faster therefore increase the heart rate. Acetylcholine causes Prepotential to occur at slow rate therefore decrease the heart rate.")
23
Effect 0f Sympathetic Stimulation on Prepotential
Why Sympathetic Stimulation causes Prepotential to occur faster? Because Sympathetic Stimulation causes - more Na+ influx [entry] - more Ca2+ influx [entry] - decreased K+ efflux [going outside] Therefore, membrane potential changes quickly from -60mV to -40mV [increases the slope of Prepotential] and when it reaches the threshold level, AP starts.

24
Effect 0f parasympathetic Stimulation on Prepotential
Why parasympathetic causes Prepotential to occur after long time? Because Parasympathetic Stimulation causes - decreased Na+ influx [entry] - decreased Ca2+ influx [entry] - increased K+ efflux [going outside] Therefore, membrane potential changes slowly from -60mV to -40mV [decreases the slope of Prepotential] and when it reaches the threshold level, AP starts.

25
Control of heart rate: Heart rate is determined by balance between Inhibition of SA node by vagus(parasympathetic) & stimulation by sympathetic Under resting condition parasympathetic discharge dominates

26
POINT TO PONDER In Transplanted Heart, where there is no sympathetic and parasympathetic nerve supply, what will be the rate of SA Node discharge [Heart Rate] ?

27
Spread of Cardiac Excitation

28
Normal Impulse Conduction
Sinoatrial node AV node Bundle of His Bundle Branches Purkinje fibers

29
SPREAD OF CARDIAC EXCITATION
Cardiac impulse originates at SA node and spread to the atria [via gap junction] – Atrial Syncytium, therefore, both atria depolarize same time. Impulse [AP] goes to AV-Node by Internodal pathway. AV-Node is the only point of electrical contact between atria and ventricle [as atria and ventricle are separated by fibrous ring which is non-conductive].

30
SPREAD OF CARDIAC EXCITATION
AV – Node At AV-Node, there is delay of 0.1 sec [100 milli- sec]. This delay is important to allow complete ventricular filling because it allows the atria to contract and empty their blood into the ventricle, before impulse reaches the ventricle and causes ventricular depolarization and contraction

31
SPREAD OF CARDIAC EXCITATION
Ventricular Excitation After AV delay of 0.1sec, impulse [AP] travels quickly via Right Bundle Branch and Left Bundle Branch [branches of Bundle of His] to Purkinje Fibers to the ventricles. Both ventricle depolarize, than contract at same time. Conduction in Purkinje Fiber is fastest 2-4 meter/sec, therefore, both ventricle depolarize quickly and at the same time.

32
Conduction speed in cardiac tissue
Slowest Conduction at AV – Node Fastest Conduction – Purkinje Fibers

33
SPREAD OF CARDIAC EXCITATION
Why Conduction is slow at AV-Node? Because there are less gap junctions. Diameter of the fiber is small.

34
Myocardial Action Potential ( Excitability )
Once myocardial cells are stimulated by action potential originating in SA node, it produces its own action potential Ventricular Muscle membrane has resting membrane potential of -90mV. Action Potential of ventricular muscle fiber has four phases 0, 1, 2, 3 ,4.

35
Ventricular action potential
Rapid depolarization (Phase 0) – due to Na+ influx Early brief Repolarization (Phase 1) - Due to closure of Na+ channels & opening of transient K+ channels. Slow depolarization (Phase 2) - this is called Plateau phase and is maintained for 200 – 300 ms – due to Ca++ influx Rapid Repolarization (Phase 3) – due to K+ efflux Resting Membrane Potential (Phase 4)
 – due to Na+ influx. Early brief Repolarization (Phase 1) - Due to closure of Na+ channels & opening of transient K+ channels. Slow depolarization (Phase 2) - this is called Plateau phase and is maintained for 200 – 300 ms – due to Ca++ influx. Rapid Repolarization (Phase 3) – due to K+ efflux. Resting Membrane Potential (Phase 4)")
36
Relationship of an Action Potential and the Refractory Period to the Duration of the Contractile Response in Cardiac Muscle

37
Electrical Activity of Heart
Because long refractory period occurs in conjunction with prolonged plateau phase, summation of twitch and tetanus of cardiac muscle is impossible This Ensures alternate periods of contraction and relaxation which are essential for pumping blood

38
References Human physiology by Lauralee Sherwood, seventh edition
Text book physiology by Guyton &Hall,11th edition Text book of physiology by Linda .s contanzo,third edition

Similar presentations


>")












>")


>")
