Download presentation
Presentation is loading. Please wait.

1
Clinical laboratory diagnostics of anemias

2
Anemia - is the decreasing of hemoglobin and red blood cells level in the unit of blood volume Reduction in one or more of the major red blood cell (RBC) measurements: Hemoglobin concentration Hematocrit RBC count From data of WHO: a hematocrit less than 40 in men and 37 in women, or hemoglobin less than 130 g/l in men and less than 120 g/l in women.
 measurements: Hemoglobin concentration Hematocrit RBC count From data of WHO: a hematocrit less than 40 in men and 37 in women, or hemoglobin less than 130 g/l in men and less than 120 g/l in women.")
4
Anemia Symptoms Because a low red blood cell count decreases oxygen delivery to every tissue in the body, anemia may cause a variety of signs and symptoms. It can also make almost any other underlying medical condition worse. If anemia is mild, it may not cause any symptoms. If anemia is slowly ongoing (chronic), the body may adapt and compensate for the change; in this case there may not be any symptoms until the anemia becomes more severe.
, the body may adapt and compensate for the change; in this case there may not be any symptoms until the anemia becomes more severe.")
6
Signs and symptoms Symptoms of anemia may include the following:
Fatigue Chest pain Abdominal pain Weight loss Weakness Dizziness and passing out, especially upon standing

7
Anemia Symptoms Fatigue decreased energy weakness lightheadedness
palpitations (feeling of the heart racing or beating irregularly) looking pale
 looking pale.")
9
Symptoms of severe anemia may include:
chest pain, angina, or heart attack dizziness fainting or passing out rapid heart rate

10
Depending on the level of hemoglobin in the blood anemia is divided on:
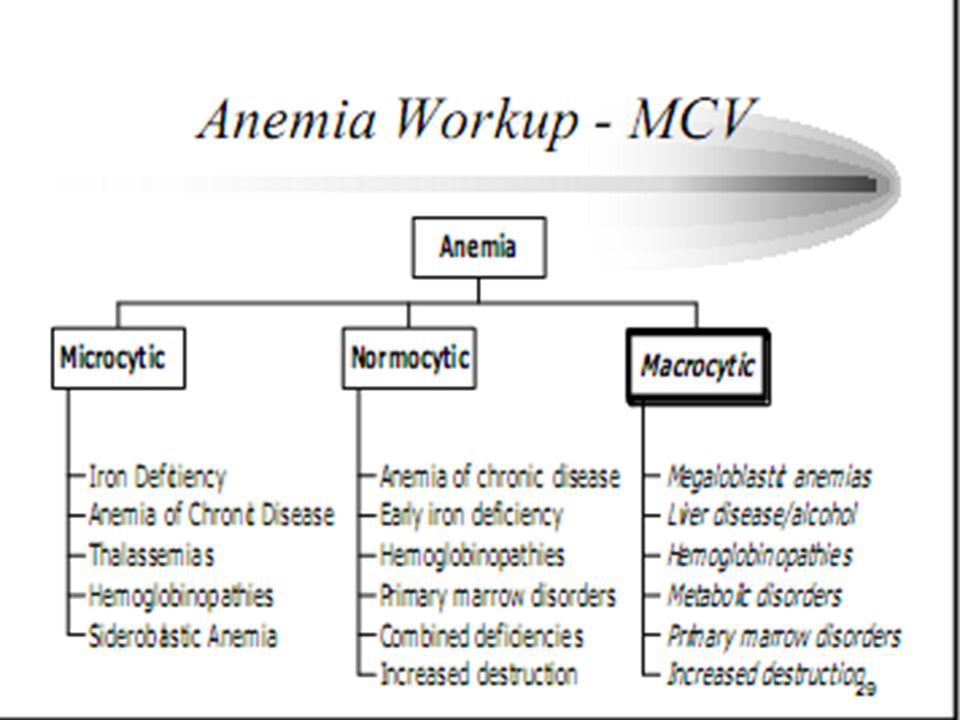
- mild degree (Hb g/l), - moderate degree (Hb g/l), - severe degree (Hb less than 69 g/l). Depending on the size of RBC and their saturation by hemoglobin (from data of colour index - CI) anemia is divided on: - Normocytic anemia (can be normochromic anemia: colour of RBC is normal and CI is 0,86-1,1); - Microcytic anemia (can be hypo- or normochromic): microcytosis , anizopoykilocytosis, hypochromia, CI < 0,7; - Macrocytic anemia: macrocytosis, megalocytosis, CI > 1,1.
, - moderate degree (Hb g/l), - severe degree (Hb less than 69 g/l). Depending on the size of RBC and their saturation by hemoglobin (from data of colour index - CI) anemia is divided on: - Normocytic anemia (can be normochromic anemia: colour of RBC is normal and CI is 0,86-1,1); - Microcytic anemia (can be hypo- or normochromic): microcytosis , anizopoykilocytosis, hypochromia, CI < 0,7; - Macrocytic anemia: macrocytosis, megalocytosis, CI > 1,1.")
11
Approaches to Anemia Kinetic approach Decreased RBC production
Increased RBC destruction Blood loss Morphologic approach Macrocytic Normocytic Microcytic

12
Decreased RBC Production
Nutrient deficiency Dietary, malabsorption Bone marrow disorders/suppression Anemia of chronic diseases Low levels of trophic hormones Epo, thyroid hormone, androgens

13
Blood Loss Most common cause of anemia
Fe deficiency almost always due to blood loss Obvious bleeding Occult bleeding Induced bleeding Operative blood loss

16
Normocytic anemia (MCV - 80-100)
A loss or destruction of RBC is increased Acute bleeding Early iron deficiency - Hemolytic anemia - Hypersplenism Decreasing of RBC synthesis -Anemia of chronic diseases (most commonly) Endocrine dysfunctions Renal insufficiency Pathology of bone marrow (for example, action of medications, infection, aplastic anemia, myelodysplastic syndrome, multiple myeloma and other infiltrative diseases).
 Endocrine dysfunctions. Renal insufficiency. Pathology of bone marrow (for example, action of medications, infection, aplastic anemia, myelodysplastic syndrome, multiple myeloma and other infiltrative diseases).")
17
Anemia of Chronic Disease
•Common • Develops over 1 to 2 months • Non-progressive • Usually mild to moderate – but hematocrit < 0.20 occasionally • 30% mildly microcytic • WBC, platelets normal or increased

18
Hemolytic Anemia • Anemia of increased destruction normochromic anemia
– Shortened RBC survival – Reticulocytosis - Response to increased RBC Destruction

20
Hemolytic Anemia

21
Equired hemolytic anemia Reticulocytosis

22
Equired hemolytic anemia Reticulocytosis

23
Hereditary disorders include erythrocyte membrane and enzymatic defects and hemoglobin abnormalities. Some hereditary disorders include the following:G6PD deficiency Herediditary spherocytosis Sickle cell anemia Thalassemia

24
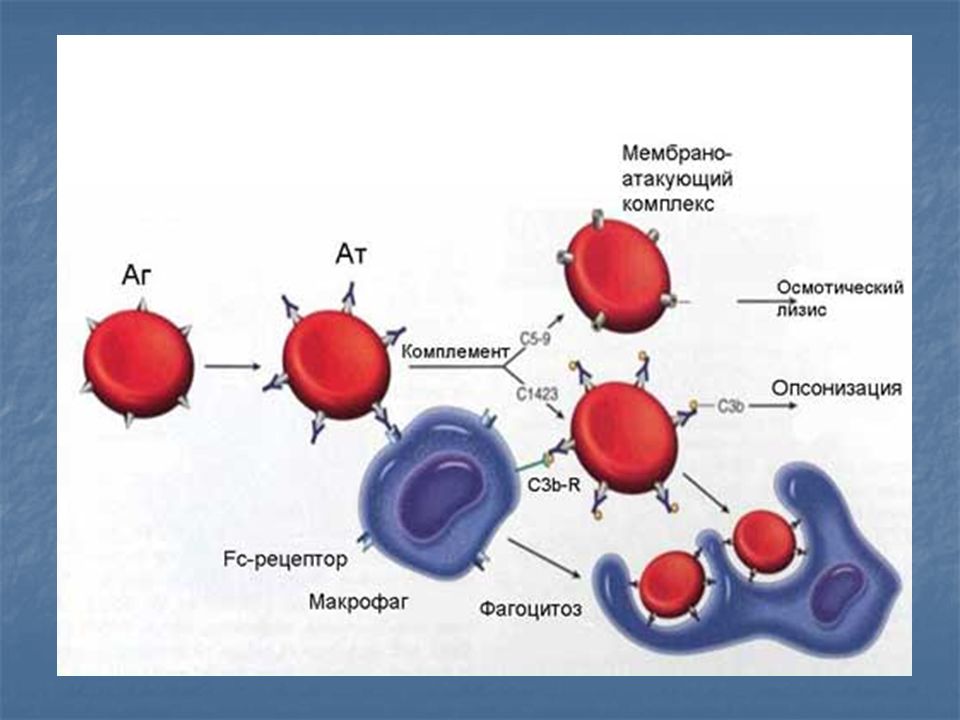
Acquired hemolytic conditions
can be due to immune disorders, toxic chemicals and drugs, antiviral agents (eg, ribavirin) physical damage, and infections Autoimmune hemolytic anemia (AIHA) may result from warm or cold autoantibody types; rarely, mixed types occur. Most warm autoantibodies are immunoglobulin (Ig) G and can be detected with the direct Coombs test, which is also known as the direct antiglobulin test (DAT)
 physical damage, and infections. Autoimmune hemolytic anemia (AIHA) may result from warm or cold autoantibody types; rarely, mixed types occur. Most warm autoantibodies are immunoglobulin (Ig) G and can be detected with the direct Coombs test, which is also known as the direct antiglobulin test (DAT)")
25
Acquired hemolytic conditions
Autoimmune hemolytic anemia and hereditary spherocytosis are classified as examples of extravascular hemolysis because the red blood cells are destroyed in the spleen and other reticuloendothelial organs. Intravascular hemolysis occurs in hemolytic anemia due to prosthetic cardiac valves, G6PD deficiency, thrombotic thrombocytopenic purpura, disseminated intravascular coagulation, and paroxysmal nocturnal hemoglobinuria (PNH).
.")
26
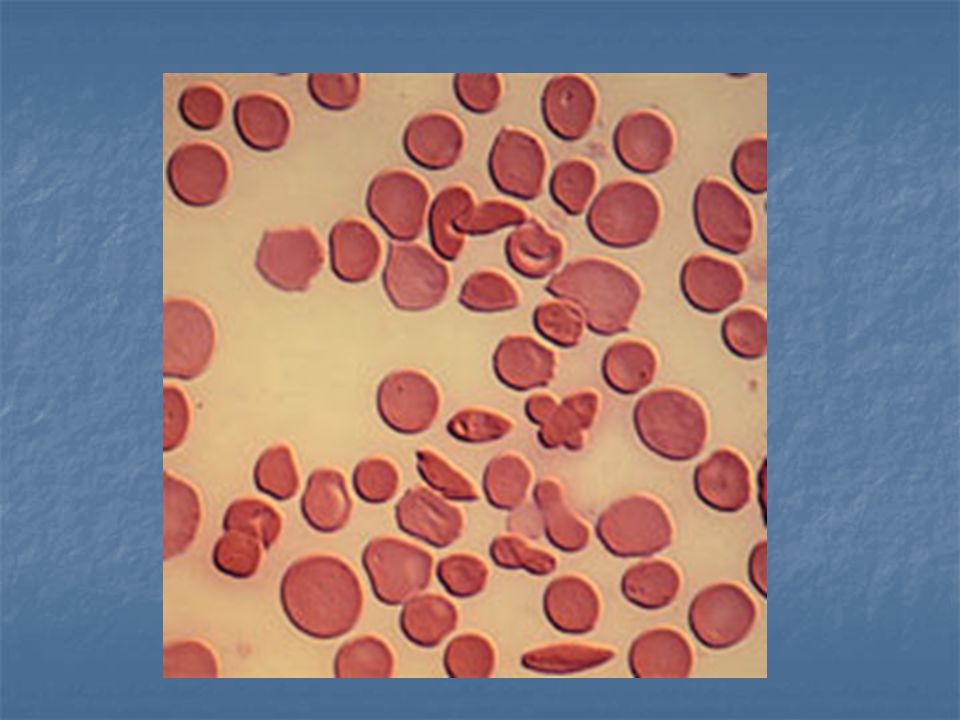
Peripheral blood smear with sickled cells

27
Spherocytes. One arrow points to a spherocyte; the other, to a normal RBC with a central pallor.

28
Hemolytic anemia due to pyruvate kinase insefficiency. Reticulocytosis

29
Membranopathy Hereditary microspherocytosis - blood

30
Membranopathy Hereditary eliptocytosis – blood

31
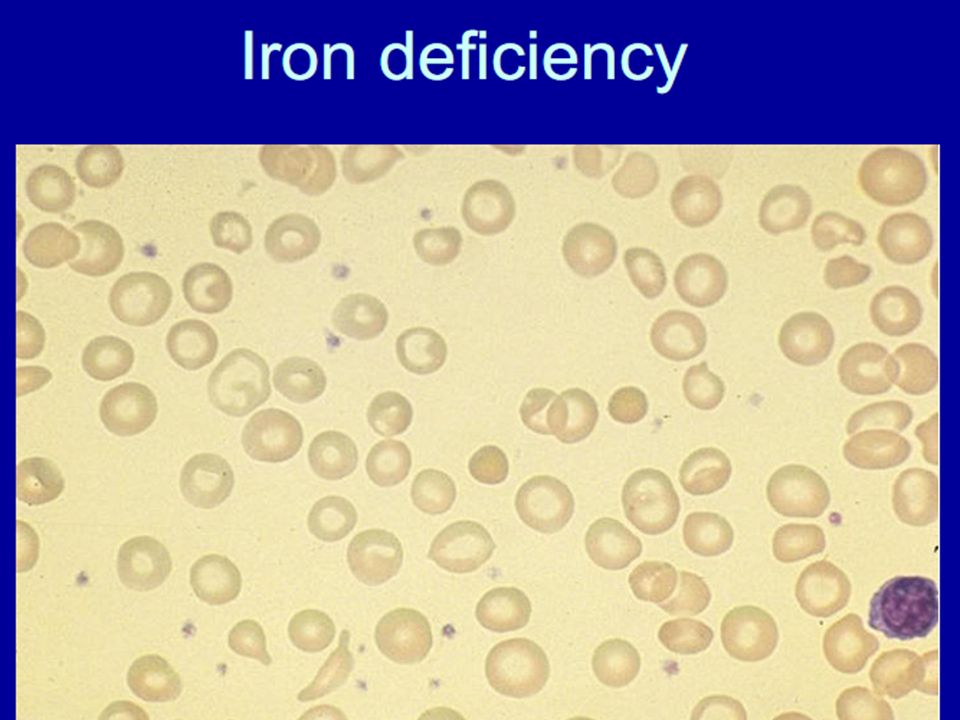
Microcytic anemia (MCV less than 80)
- Usually hypochromic as well Iron-deficiency anemia Anemia of chronic diseases(rare) Sideroblastosis Hereditary anemia (thalassemia) Lead poisoning Deficit of copper, poisoning by zinc
 Sideroblastosis. Hereditary anemia (thalassemia) Lead poisoning. Deficit of copper, poisoning by zinc.")
34
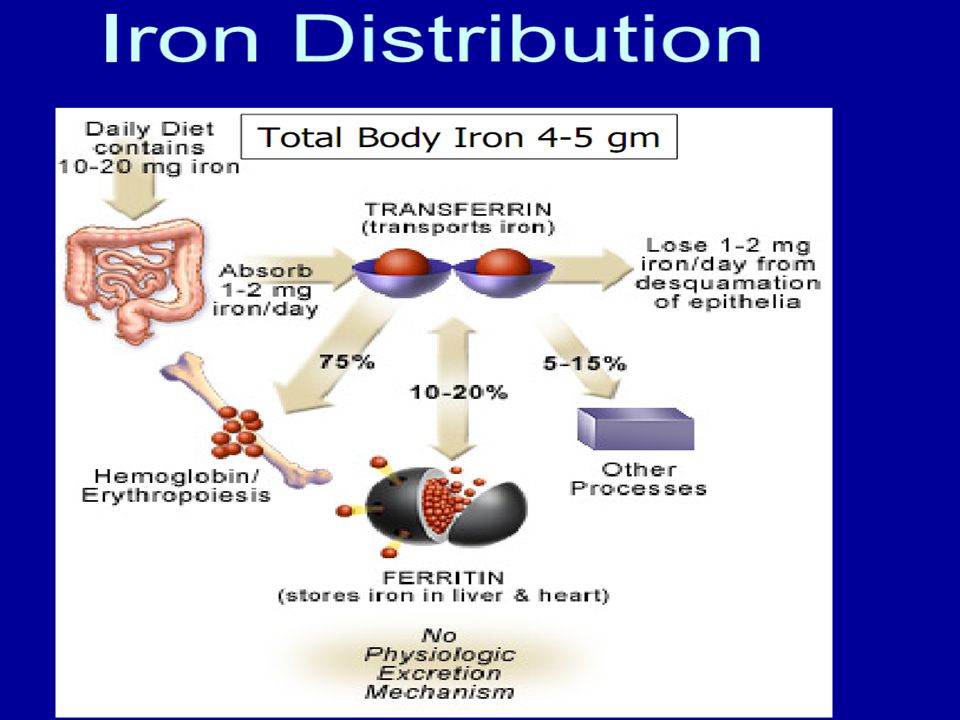
Iron Absorption • Stomach acid converts ferric (insoluble) to
ferrous (absorbable) state Decreased absorption w/ acid blockers Increased w/ citrate & ascorbate (chelators) Increased absorption w/ orange juice Decreased w/ plant phytates, tannins, soil clay, & laundry starch – Pica may exacerbate Fe deficiency
 state. Decreased absorption w/ acid blockers. Increased w/ citrate & ascorbate. (chelators) Increased absorption w/ orange juice. Decreased w/ plant phytates, tannins, soil. clay, & laundry starch. – Pica may exacerbate Fe deficiency.")
35
Iron Deficiency Causes
– Blood loss • GI tract • Renal (rare) • Pulmonary (rare) – Insufficient dietary iron Decreased absorption
 • Pulmonary (rare) – Insufficient dietary iron. Decreased absorption.")
36
Consequences of Iron Deficiency Hematologic
• Microcytic, hypochromic anemic • Low grade hemolysis d/t stiff RBC membrane • Thrombocytosis w/ plts k – Erythropoietin may cross react w/ plt Precursors

39
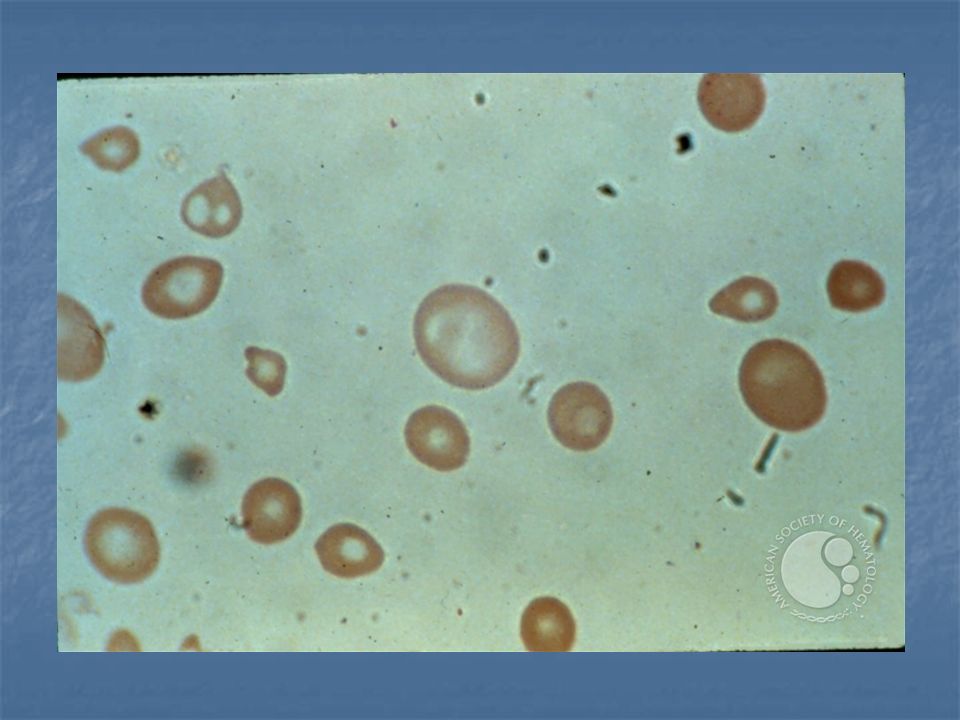
Makrocytic anemia (MCV more than 100 fl)
- Megaloblastic anemia (vitamin В12 or folic acid deficiency ) - Toxic effect of chemotherapeutic agents (methotrexate) or other medications (zidovudine (AZT), phenytoin) - Pathology of bone marrow - Chronic abuse by alcohol (toxic effect) - Liver disease
 - Toxic effect of chemotherapeutic agents (methotrexate) or other medications (zidovudine (AZT), phenytoin) - Pathology of bone marrow. - Chronic abuse by alcohol (toxic effect) - Liver disease.")
40
Macrocytosis (MCV > 100 fl)
•Common – Drugs (cytotoxics, immunosuppressants, AZT, anticonvulsants) – Alcohol – Liver disease – Reticulocytosis –B12/folate deficiency – Myelodysplastic syndrome – Marrow infiltration (malignancy, fibrosis) • Less common –Aplasia – Cold agglutinins – Hyperglycemia – Hyperleukocytosis
 – Alcohol. – Liver disease. – Reticulocytosis. –B12/folate deficiency. – Myelodysplastic syndrome. – Marrow infiltration (malignancy, fibrosis) • Less common. –Aplasia. – Cold agglutinins. – Hyperglycemia. – Hyperleukocytosis.")
41
Megaloblastic Hematopoiesis
• Marrow failure due to: disrupted DNA synthesis & ineffective hematopoiesis • Giant precursors and nuclear:cytoplasmic dyssynchrony in marrow • Neutrophil hypersegmentation & macroovalocytes in blood • Anemia (and often leukopenia & thrombocytopenia) • Almost always due to Cbl or folate deficiency
 • Almost always due to Cbl or folate deficiency.")
43
Megaloblastic Anemia Smear Macro-ovalocytic Polychromasia
Hypersegmented neutrophil

44
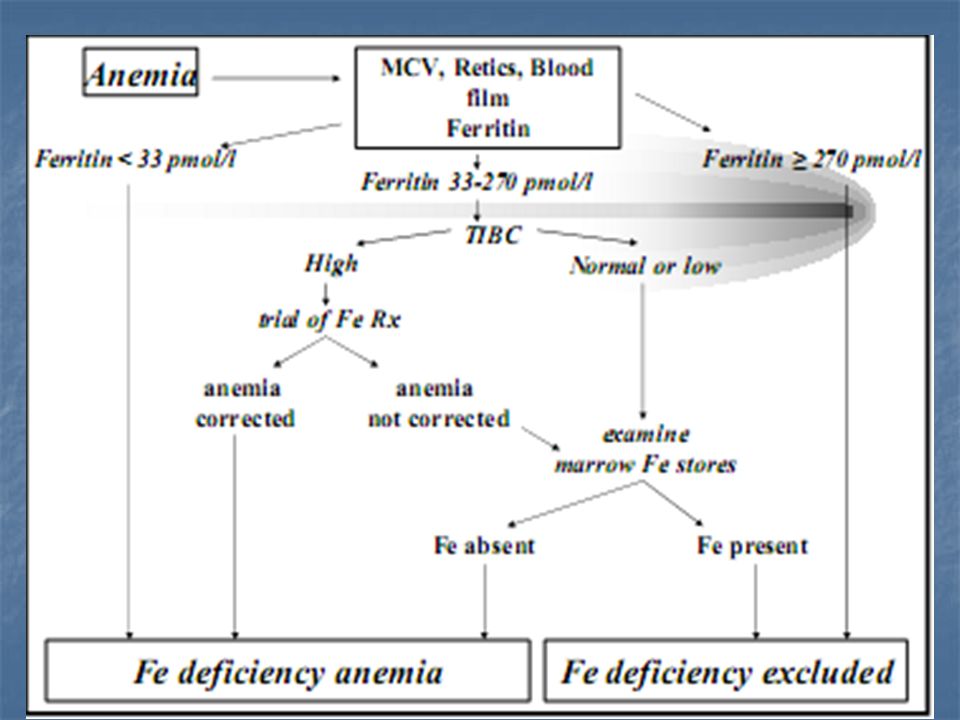
Diagnosis The only way to diagnose anemia is with a blood test. Generally, a full blood count is done. Apart from reporting the amount of red blood cells and the hemoglobin level, the automatic counters also measure the size of the red blood cells, which is an important tool in distinguishing between the causes. Occasionally, other tests are required to further distinguish the cause for anemia. These are discussed with the differential diagnosis. The doctor may also decide to take some other screening blood tests that might identify the cause of fatigue; glucose levels, ESR, ferritin, renal function tests and electrolytes may be part of such a workup.

45
Lab tests for anemia may include the following:
Complete blood count - Determines the severity of the anemia and is almost always the first test ordered Stool guaiac - Tests for blood in stool Peripheral blood smear - Looks at the red blood cells under a microscope Iron level - Low iron is one of the most common causes of anemia Transferrin level - Looks at a protein that carries iron around the body Ferritin - Looks at the total iron available in the body Folate - A vitamin needed to produce red blood cells, which is low in people with poor eating habits

46
Thank for your attention!

Similar presentations








/ HYPOCHROMIC &/or (NORMO)/ MICROCYTIC ANEMIAS 1. Disorders of iron utilization a. iron deficiency b. anemia of.>")













