Download presentation
Presentation is loading. Please wait.

1
Delivering High-Impact Interventions: Afghanistan’s Experience in Scaling Up Skilled Birth Attendants Pashtoon Azfar, Jhpiego Midwifery Advisor and President of the Afghan Midwives Association

2
2 Presentation Outline Overview of ACCESS/HSSP Project A glance at Afghanistan’s Health Profile Progress to date Who helped make it happen Afghan Midwives Association and its role in: Strengthening the midwifery profession Improving maternal health in Afghanistan Lessons learned and recommendations

3
3 ACCESS HSSP Associate Award under ACCESS Program Jhpiego is prime with subs Futures Group and Save the Children US July 2006 – Mar 2011, $40 million Focus is on increasing the utilization of health services at the rural level by improving the quality of health services, increasing the number of skilled providers and generating demand for health services Four Intermediate Results (IRs)
")
5
5 A Glance at Afghanistan’s Health Profile Challenging Health Indicators Maternal Mortality Ratio: 1,600/100,000 Neonatal Mortality 60/1,000 live births Less than 9% of deliveries attended by a skilled birth attendant Few female health workers 467 midwives in 2002 21% of health facilities had female staff Socio-cultural demand for female providers Photo credit Med Air

6
6 Maternal Health in Afghanistan Estimated 26,000 women dying from pregnancy- related causes every year 1 woman dying every 27 minutes 78% of deaths are preventable Source: Bartlett et al 2005

7
7 Progress to Date Before: 8% of births attended by a skilled provider in 2003 Skilled antenatal care (ANC) at 4.6% in 2003 5 midwifery education programs in 2002 Outdated midwifery education curriculum with a focus on training hospital midwives 467 midwives in the country in 2002 Few female staff in health facilities After: Birth attendance by skilled provider increased to 19% in 2006 Skilled ANC increased to 32% in 2006 27 midwifery education programs in 2009 Competency-based training curriculum developed to train hospital and community midwives To date, 1,961 competent midwives have graduated, 1,675 deployed (85%) 61% of health centers staffed with at least 1 midwife
 at 4.6% in 2003 5 midwifery education programs in 2002 Outdated midwifery education curriculum with a focus on training hospital midwives 467 midwives in the country in 2002 Few female staff in health facilities After: Birth attendance by skilled provider increased to 19% in 2006 Skilled ANC increased to 32% in 2006 27 midwifery education programs in 2009 Competency-based training curriculum developed to train hospital and community midwives To date, 1,961 competent midwives have graduated, 1,675 deployed (85%) 61% of health centers staffed with at least 1 midwife")
8
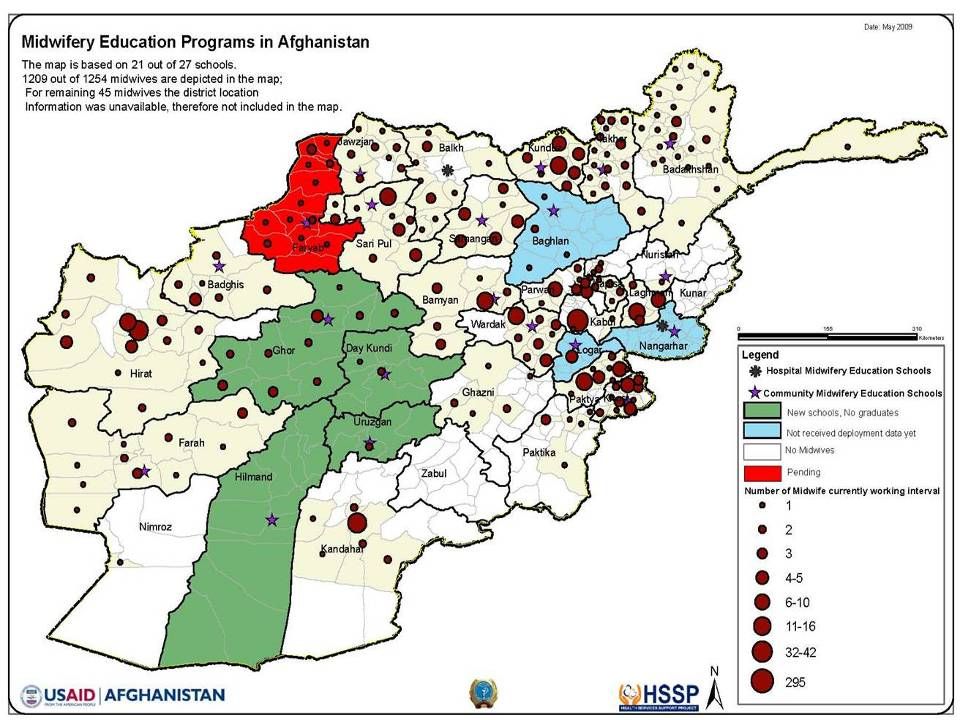
8 Community Midwifery Education Schools Badakshan Bamyan Jawzjan Khost Paktya Takhar Ghor Wardak Parwan Logar GhaniKhail 12.Samangan 13.Sari Pul 14.Baghdris 15.Farah 16.Kunduz 17.Helmand 18.Uruzgan 19.Faryab 20.Daikundi 21.Lagman 22.Baghlan Newly graduated community midwives in Badakhshan province take midwifery pledge.

9
9 Institute of Health Sciences— Hospital Midwives Kabul Herat Nangarhar Kandahar Balkh Photo by Hannah Gibson

12
12 Creating the Policy Environment 18-month competency-based curricula and training materials developed in February 2004; focus on required clinical skills Residential program addressed cultural concerns about women being away from families Testing and certification process of midwives trained previously was established Knowledge and skills of teachers and clinical preceptors updated Midwifery Education Policy endorsed 2005

13
13 Establishment of Accreditation System to Ensure Quality in Midwifery Education Unified national system built, based on education standards All programs initially “encouraged” to implement standards National Midwifery Education Accreditation Board established Standards and accreditation became mandatory Improvements extended to clinical areas

14
14 The Need for Midwives Calculation of required number of midwives based on number of health facilities (actual and planned) and population Approximately 5,000+ midwives needed to staff the expected ideal distribution of health facilities Human resource database established in Ministry of Health
 and population Approximately 5,000+ midwives needed to staff the expected ideal distribution of health facilities Human resource database established in Ministry of Health")
15
15 Selection of Students According to Human Resource Needs of the Country Mostly from rural areas Commitment to work post graduation Collaboration with national, provincial and local health authorities, as well as communities in selection and recruitment Follow selection policies of the Ministry of Public Health

16
16 Deployment, Supervision and Support Deployment Midwives deployed to community facility where they were recruited from Working within a defined Basic Package of Health Services Supportive supervision Supervision Supervision teams established and checklists used. Support to/from the Afghan Midwives Association Built capacity of AMA AMA promotes and strengthens the midwifery profession through –Organizational development and sustainability, leadership programs, advocacy and in-service trainings

17
17 Who Helped to Make it Happen? Ministry of Public Health, Afghanistan Donors — USAID, World Bank, European Commission USAID, REACH, ACCESS HSSP NGO partners implementing CME and I.H.S. schools WHO, UNICEF and other supporters of midwifery National Midwifery Education Accreditation Board Afghan Midwives Association Staff and students of all midwifery schools Jhpiego, the ACCESS Program and partners

18
18 Afghan Midwives Association The AMA aims to: Promote and strengthen the midwifery profession and the role of the midwife to ensure the well-being of women and families in Afghanistan.

19
19 AMA Inaugural Congress

20
20 AMA’s Progress More than 1,100 members 27 provincial chapters Governing body

21
21 AMA’s Accomplishments to Date During the last four years, the AMA recognized midwives who made significant contributions to maternal health.

22
22 Advocacy for Safe Motherhood Women are not dying of diseases we can’t treat …They are dying because societies have yet to make the decision that their lives are worth saving.” Mahmoud Fathalla This quotation was used as inspiration for the need to build political and social will for safe motherhood issues.

23
23 Advocacy for Safe Motherhood

24
24 Involving Men in Safe Motherhood

25
25 National Celebration of Safe Motherhood Day

26
26 Provincial Celebration of Safe Motherhood Day

27
27 Midwives and Obstetricians Come Together to Support the Lives of Mothers and Newborns

28
28 Celebration of AMA’s 5 th Annual Congress

29
29 Celebration of AMA’s 5 th Annual Congress

30
30 Mother’s Memorial Quilt

31
31 Celebrating International Day of Midwives 2009

32
32 AMA Promotes Women’s Empowerment Women’s participation in education programs Contribute to household economy Safeguard the health and well-being of families Women in leadership roles/positions

33
33 Lessons Learned and Recommendations Increasing skilled attendance at birth requires political will and commitment Focus should be on establishing and supporting a national system and processes Build on previous successes and approaches Selection and recruitment of midwives linked to deployment are key to success; think about the quality and deployment at the beginning Involve the community and think about creative and culturally appropriate approaches to attract students and the support of the community and families Midwives must be continually supported in maximizing their potential A professional association, such as the AMA, is important to providing advocacy for the profession and supporting the midwives, and contributes to sustainability Success of community midwifery programs has created demand

34
34 Thank You

Similar presentations



 Eastern and Southern Africa Aga Khan Health Services.>")
 Project University Research Co., LLC Center for Human Services.>")














>")

