Download presentation
Presentation is loading. Please wait.

1
Ultrasound-guided Regenerative Medicine Procedures: Pandora or Panacea Ken Mautner, MD Director, Primary Care Sports Medicine Emory Sports Medicine

2
Goal of talk ““I would like you to talk about stem cells and PRP, the evidence for them in tendons and joints, and why ultrasound guidance is important” JJon Finnoff, DO DDo it less than 20 minutes !

3
Outline Ultrasound guidance for regenerative medicine procedures Dangers of steroids in treating tendinopathy Regenerative injections for recalcitrant tendons Needle Tenotomy PRP Stem cells Regenerative Medicine for Cartilage/OA (knee) 1-2:30 pm today!
 1-2:30 pm today!")
4
Is ultrasound guidance needed for regenerative medicine procedures ? Accuracy Efficacy Cost-effectiveness

5
Reactive vs Degenerative Tendon

6
What is ideal way to treat tendinopathy? “Old School” Treatments Rest Ice Immobilization NSAIDS Physical Therapy/ biomechanics Possible corticosteroid Injection (CSI) RTP when pain free/ functional But is tissue healed? If symptoms persist Surgery LACK OF EVIDENCE FOR TRADITIONAL TREATMENTS
 RTP when pain free/ functional But is tissue healed. If symptoms persist Surgery LACK OF EVIDENCE FOR TRADITIONAL TREATMENTS.")
7
Lancet, 2010

9
JAMA, 2013

10
What is ideal way to treat tendinopathy? Evolving algorithm -- “New School” Pathology specific conservative treatments NSAIDS If inflammatory Mechanotransduction for tendinosis Eccentrics exercises IASTM/ CFM/ART Nitric Oxide ESWT Regenerative intervention Percutaneous needle tenotomy (PNT) High Volume Injection (HVIGI) Scraping PRP TENEX (FAST) ADSC +/- PRP BMAC TIMING OF INTERVENTION AND TYPE OF INTERVENTION HAS NOT BEEN FIGURED OUT
 High Volume Injection (HVIGI) Scraping PRP TENEX (FAST) ADSC +/- PRP BMAC TIMING OF INTERVENTION AND TYPE OF INTERVENTION HAS NOT BEEN FIGURED OUT.")
11
Percutaneous Needle Tenotomy (PNT) and Platelet Rich Plasma (PRP)
 and Platelet Rich Plasma (PRP)")
12
PNT (needle tenotomy) for lateral epicondylosis McShane et al, Journal of Ultrasound Med. 2006 Ultrasound guided PNT with steroid for chronic lat. epicondylitis Failed conservative tx 58 pts-- avg f/u 28 mo. 80 % Good or Excellent Outcome 85% would refer friend or family for procedure McShane et al, Journal of Ultrasound Med 2008 Ultrasound guided PNT without steroid for chronic lat. Epicondylitis Failed conservative tx 57 pts --avg f/u 22 mo. 92% Good or Excellent Outcome 90% would refer friend or close relative for procedure

13
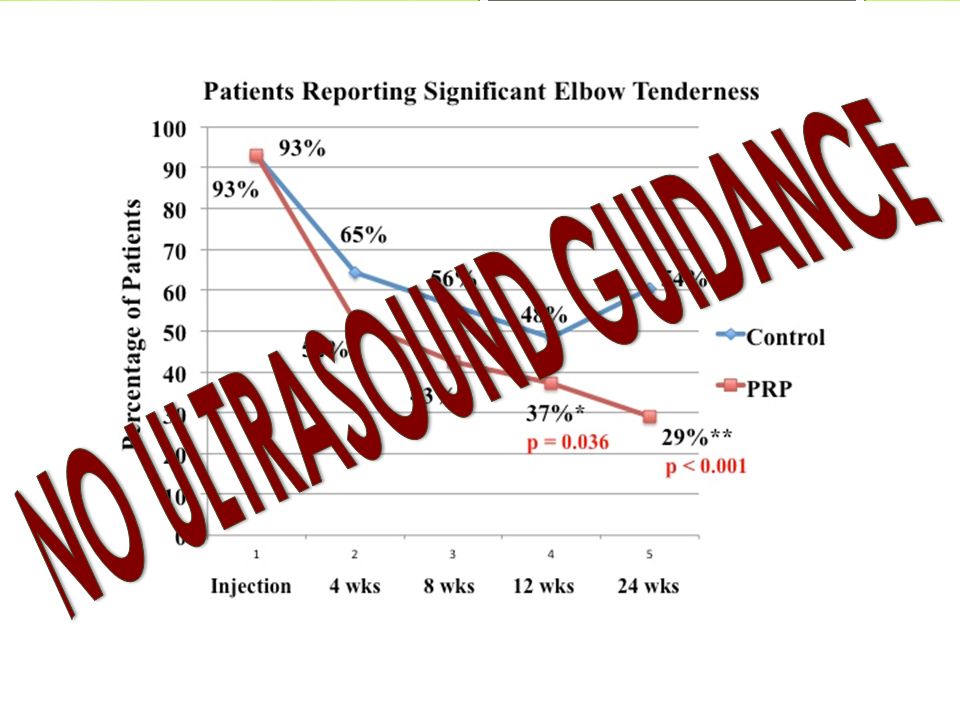
PRP for chronic lateral epicondylosis 140 pts evaluated for lateral epicondylosis 20 had refractory pain an avg. of 15 months later 15 in treatment group, 5 in bupivicaine control group Intervention – Injection w/ autologous PRP once into common extensor tendon followed by gradual increase in rehab program through 4 weeks after which full activity allowed Outcome – A 46%, 60% and 81% improvement in VAS pain scores at 1, 2 and 6 months respectively in tx group – 3/5 in bupivicaine group withdrew/ sought other tx – At final F/U (12-38 months) 93% pain free (<10/100 VAS) – No complications, no one got worse AJSM, 2006
 93% pain free (<10/100 VAS) – No complications, no one got worse AJSM,")
14
Pts age 16-70 (avg 48 yrs) Greater than 6 months of pain (avg 36 months) Diagnosed by clinical exam plus MRI or diagnostic US Failed conventional treatments Medications Bracing Stretching Strengthening CFM Modalities PRP done under US guidance PMR journal, 2013
 Greater than 6 months of pain (avg 36 months) Diagnosed by clinical exam plus MRI or diagnostic US Failed conventional treatments Medications Bracing Stretching Strengthening CFM Modalities PRP done under US guidance PMR journal, 2013")
15
Data of PRP procedures 325 patients with isolated tendinopathy sent questionnaire Eliminated all non tendons and regional PRP treatments 180 responded (55%) All retrospective data analyzed with following questions: Overall improvement Not at all, slightly, moderately, mostly, completely VAS score –pre and post Overall satisfaction Nirchl phase scale
 All retrospective data analyzed with following questions: Overall improvement Not at all, slightly, moderately, mostly, completely VAS score –pre and post Overall satisfaction Nirchl phase scale")
16
Distribution of Tendons Lateral Epicondyle30 Patella Tendon27 Achilles27 Rotator Cuff21 Hamstring17 Gluteus Medius16 Medial Epicondyle11 Plantar Fascia9 13 other tendons<5 each

17
Improvement 82% reported moderate to complete improvement – 50%- 100% relief of symptoms 70 % reported mostly to complete improvement -- 75-100% relief of symptoms

18
Pain Score pre and post PRP ➤ 74 % Reduction in VAS 7.3 2.1

19
Why are we still debating if orthobiologics works? Need to define what we are injecting ? Platelet counts MSC counts Leukocyte +/ - Differential RBC +/ RBC – Autologous/ Allogenic Need to define the procedure US guidance Needle tenotomy? Rehabilitation methods Immobilization ? Timing of eccentrics Do different body regions require different formulas ? Slide from 2011

20
____________________________ 1 If WBC are present (+) the % of neutrophils should also be reported. 2 The method of exogenous activation should be reported. April, 2015

21
80 patients randomized PRP vs Placebo ACP vs saline 2 injections 5 days apart 5 days after injury End point was RTP No difference Average 42 days 2014, Reurink

22
Rehabilitation L+ PRP 42 days vs 26 days

23
Why the difference ? MY TAKE: L+ PRP may reduce recovery from acute hamstring muscle injury

24
Is it the Needle? AJSM, 2013

27
PRP vs PNT for RTC pathology DBRCT comparing 2 PNT vs 2 PRP injections under US guidance for RTC tendinosis or small, partial tear Measured results using Shoulder Pain and Disability Index Clinical Rehabiliation, 2012

28
60 patients randomized to US- guided injection of PRP vs no injection on POD 7, 14 Outcomes tracked through 16 wks MRI done at 16 wks RESULTS: PRP did NOT improve early fxnl recovery, ROM, or strength NO difference in structural integrity at 16 wks. Did not look at long term outcomes…. AJSM, 2015

29
Stem cells for Tendinopathy April, 2015

30
Stem Cells for soft tissue Surprisingly few clinical studies examining stem cells use for soft tissue injuries Many more studies looking at cartilage Soft tissue studies predominantly involve PRP Early clinical studies promising but much more work needed in the area.

31
46 pts, 60 patellar tendons Dermal fibroblasts Cultured for 4 wks Injected in autologous plasma US guidance used Compared to autologous plasma only AJSM, 2011

32
Is it worth it? High cost Lag time (4 wks) Regulatory issues
 Regulatory issues")
33
45 patients in received BMC during single-row arthroscopic RTC repair 51,000 MSC +/- 25,000 45 age matched controls Up to 10 years follow up with MRI imaging RESULTS: 6 mo 100% of MSC group healed 67% of control group healed 10 years 87% of MSC group with intact RTC 44% of control group Results most correlated with MSC concentration

34
Conclusions Needle tenotomy is effective for tendinosis US guidance will improve accuracy Tenotomy helpful no matter the injectate Saline, WB, ACP, PRP, Stem Cells PRP may have better results than needling alone Unsure if related to pathology (tendinosis vs tear) Stem cells may have better results than PRP/ needling No head to head studies Is it worth the cost and increased risk to perform this procedure for tendons ? I rarely utilize stem cells as a first line treatment for recalcitrant tendinopathy

35
Ken.mautner@emory.org

Similar presentations
















>")




