Download presentation
Presentation is loading. Please wait.

1
Ken Mautner, MD Emory Sports Medicine Center
Point: Counterpoint Exercise vs Intervention for Recalcitrant Tendinopathy Ken Mautner, MD Emory Sports Medicine Center

3
The Continuum of Tendinopathy
Harmon K G , and Rao A L Hematology 2013;2013: ©2013 by American Society of Hematology

4
20-25% do not get better with consesrvative tx- PT, etc
What to do with them ?? Patella tendon even worse? Insertional achilles/ HS tendon ?

5
Before we get started…….
Rehabilitation is the cornerstone of any successful treatment for tendinopathy Eccentric exercise programs have a proven track record to be successful in treatment of tendinosis, especially Achilles tendon There are other modalities that are not going to be discussed here that also have some efficacy in the treatment of tendinosis STM (CFM, Graston, ASTYM) NO patches ECSWT In most cases, interventions should be reserved for tendons that have failed appropriate conservative/ less invasive treatments
 NO patches. ECSWT. In most cases, interventions should be reserved for tendons that have failed appropriate conservative/ less invasive treatments.")
6
However …. 20-25% of recalcitrant tendinopathy does not get better with optimal rehabilitation Rigorous program to be compliant Outside of Achilles tendon, results may be even worse Certain body regions seem to do even worse with traditional care: Insertional Achilles tendinosis Proximal Patella tendinosis Proximal HS tendinosis

7
“There is strong evidence that PRP injections are not efficacious in the management of chronic lateral elbow tendinopathy” BJSM, Feb 2014 Arthroscopy, Nov, 2013 ”The current evidence suggests that PRP may be of benefit over standard treatment as a second line intervention…the current evidence is promising but limited”

9
“God heals, and the doctor takes the fees”
“The art of medicine involves amusing the patient while nature takes it course” “God heals, and the doctor takes the fees” Both cynical….

10
Intervention for Tendinopathy
Dexamethasone Rehabilitation Lidocaine Thrombin pH ?? Marcaine Cytokines ?? Plt Concentr. Intervention for Tendinopathy Dextrose CaCL RBC’s WBC’s ABX analogy Needle ACP Plt lysate Orthokine Autologous Blood Ropivicaine

11
Corticosteroids Injections for Tendinopathy ?

12
Lancet, 2010

13
Corticosteroid Injections
Lancet, 2010

14
JAMA, 2013 Corticosteroid injection resulted in lower complete recovery or much improvement at 1 year vs placebo injection (83% vs 96%, respectively; P=.01) and greater 1-year recurrence The physiotherapy and no physiotherapy groups did not differ on 1-year ratings of complete recovery or much improvement (91% vs 88%, respectively; RR, 1.04 [99% CI, ]; P=.56) or recurrence (29% vs 38%) Similar patterns were found at 26 weeks, with lower complete recovery or much improvement after corticosteroid injection vs placebo injection (55% vs 85%, respectively; RR, 0.79 [99% CI, ]; P.001) No difference between the physiotherapy and no physiotherapy groups (71% vs69%, respectively; RR, 1.22 [99% CI, ]; P=.84). At 4 weeks: significant interaction between corticosteroid injection and physiotherapy (P=.01), patients receiving the placebo injection plus physiotherapy had greater complete recovery or much improvement vs no physiotherapy (39% vs 10%, respectively; P=.004). However, there was no difference between patients receiving the corticosteroid injection plus physiotherapy vs corticosteroid alone (68% vs 71%, respectively; RR, 0.95 [99% CI, ]; P=.57).
 and greater 1-year recurrence. The physiotherapy and no physiotherapy groups did not differ on 1-year ratings of complete recovery or much improvement (91% vs 88%, respectively; RR, 1.04 [99% CI, ]; P=.56) or recurrence (29% vs 38%) Similar patterns were found at 26 weeks, with lower complete recovery or much improvement after corticosteroid injection vs placebo injection (55% vs 85%, respectively; RR, 0.79 [99% CI, ]; P.001) No difference between the physiotherapy and no physiotherapy groups (71% vs69%, respectively; RR, 1.22 [99% CI, ]; P=.84). At 4 weeks: significant interaction between corticosteroid injection and physiotherapy (P=.01), patients receiving the placebo injection plus physiotherapy had greater complete recovery or much improvement vs no physiotherapy (39% vs 10%, respectively; P=.004). However, there was no difference between patients receiving the corticosteroid injection plus physiotherapy vs corticosteroid alone (68% vs 71%, respectively; RR, 0.95 [99% CI, ]; P=.57).")
15
Physiotherapy did not result in any significant differences .
JAMA, 2013 Among patients with chronic unilateral lateral epicondylalgia, the use of corticosteroid injection vs placebo injection resulted in worse clinical outcomes after 1 year. Physiotherapy did not result in any significant differences . Corticosteroid injection resulted in lower complete recovery or much improvement at 1 year vs placebo injection (83% vs 96%, respectively; P=.01) and greater 1-year recurrence The physiotherapy and no physiotherapy groups did not differ on 1-year ratings of complete recovery or much improvement (91% vs 88%, respectively; RR, 1.04 [99% CI, ]; P=.56) or recurrence (29% vs 38%) Similar patterns were found at 26 weeks, with lower complete recovery or much improvement after corticosteroid injection vs placebo injection (55% vs 85%, respectively; RR, 0.79 [99% CI, ]; P.001) No difference between the physiotherapy and no physiotherapy groups (71% vs69%, respectively; RR, 1.22 [99% CI, ]; P=.84). At 4 weeks: significant interaction between corticosteroid injection and physiotherapy (P=.01), patients receiving the placebo injection plus physiotherapy had greater complete recovery or much improvement vs no physiotherapy (39% vs 10%, respectively; P=.004). However, there was no difference between patients receiving the corticosteroid injection plus physiotherapy vs corticosteroid alone (68% vs 71%, respectively; RR, 0.95 [99% CI, ]; P=.57).
 and greater 1-year recurrence. The physiotherapy and no physiotherapy groups did not differ on 1-year ratings of complete recovery or much improvement (91% vs 88%, respectively; RR, 1.04 [99% CI, ]; P=.56) or recurrence (29% vs 38%) Similar patterns were found at 26 weeks, with lower complete recovery or much improvement after corticosteroid injection vs placebo injection (55% vs 85%, respectively; RR, 0.79 [99% CI, ]; P.001) No difference between the physiotherapy and no physiotherapy groups (71% vs69%, respectively; RR, 1.22 [99% CI, ]; P=.84). At 4 weeks: significant interaction between corticosteroid injection and physiotherapy (P=.01), patients receiving the placebo injection plus physiotherapy had greater complete recovery or much improvement vs no physiotherapy (39% vs 10%, respectively; P=.004). However, there was no difference between patients receiving the corticosteroid injection plus physiotherapy vs corticosteroid alone (68% vs 71%, respectively; RR, 0.95 [99% CI, ]; P=.57).")
16
Interventional guided treatment for calcific tendinopathy of the shoulder?

17
Rotator Cuff Calcific Tendinopathy
Intratendinous calcification Hydroxyapetite crystal Supraspinatus (>50%) > Infraspinatus > Subscapularis Uncertain Etiology Degenerative Reactive Females > males Age most common Seen on % of radiographs Speed et al, 1999 NEJM
 > Infraspinatus > Subscapularis. Uncertain Etiology. Degenerative. Reactive. Females > males. Age most common. Seen on % of radiographs. Speed et al, 1999 NEJM.")
18
Calcific Tendinopathy (RTC)
Process may be blocked

19
Studies Several non-controlled studies from showing good – excellent results with US guided aspiration and lavage 60-74% success rate from published studies

20
American Journal Of Roentgenology, 2007
67 consecutive pts treated and evaluated up till 1 year after treatment 91% of shoulders had substantial or complete improvement 64% with perfect motion 89% complete or near complete resolution of calcifications 44% transient recurrence in symptoms (around 6 wks after procedure)
")
21
Radiology, 2009 Rotator Cuff Calcific Tendonitis: short term and 10 year outcome after 2 needle US guided percutaneous treatment- non randomized controlled trial 219 treated 68 refused treatment – control group 1 treatment performed with 16g needle and 2 needles

22
Shoulder Function Scores (Constant)
Graphs illustrate evolution of (a) Constant and (b) VAS scores in control subjects and patients with rotator cuff calcific tendonitis; 235 shoulders were treated, and 68 shoulders were not treated. Data are mean scores ± standard deviations. Significant differences (∗) between treated and nontreated patients are illustrated. (See also Table 3.) Scores 1 mo- 73.2 Scores 1 yr Serafini G et al. Radiology 2009;252:
 Constant and (b) VAS scores in control subjects and patients with rotator cuff calcific tendonitis; 235 shoulders were treated, and 68 shoulders were not treated. Data are mean scores ± standard deviations. Significant differences (∗) between treated and nontreated patients are illustrated. (See also Table 3.) Scores 1 mo Scores 1 yr Serafini G et al. Radiology 2009;252:")
23
VAS scores VAS 1 mo- 4.8 VAS 1 yr- 2.7
Graphs illustrate evolution of (a) Constant and (b) VAS scores in control subjects and patients with rotator cuff calcific tendonitis; 235 shoulders were treated, and 68 shoulders were not treated. Data are mean scores ± standard deviations. Significant differences (∗) between treated and nontreated patients are illustrated. (See also Table 3.) VAS 1 mo- 4.8 VAS 1 yr Serafini G et al. Radiology 2009;252:
 Constant and (b) VAS scores in control subjects and patients with rotator cuff calcific tendonitis; 235 shoulders were treated, and 68 shoulders were not treated. Data are mean scores ± standard deviations. Significant differences (∗) between treated and nontreated patients are illustrated. (See also Table 3.) VAS 1 mo VAS 1 yr Serafini G et al. Radiology 2009;252:")
24
Arthroscopic removal (20) vs PNT/aspiration (16) vs Control (17)
Joint Bone Spine, 2009 102 pts 53 did not improve with steroid injection Arthroscopic removal (20) vs PNT/aspiration (16) vs Control (17) At 4 month f/u > 70% improvement PNT 62% vs Scope 65% > 90% improvement PNT-48% vs Scope 8% 2 year f/u Arthroscopy = PNT group >> Control PNT/aspiration equal or better than Scope
 vs PNT/aspiration (16) vs Control (17) At 4 month f/u. > 70% improvement. PNT 62% vs Scope 65% > 90% improvement. PNT-48% vs Scope 8% 2 year f/u. Arthroscopy = PNT group >> Control. PNT/aspiration equal or better than Scope.")
25
Is Rehabilitation Effective for Tendinopathy?
Need another stu

26
20 studies with 625 patients included CONCLUSIONS:
BJSM, Ocotober, 2012 Systematic review of the relationship between observable structural changes and clinical outcomes following response to therapeutic exercise 20 studies with 625 patients included CONCLUSIONS: “The available literature does not support observable structural changes as an explanation for the response to therapeutic exercise when treated by eccentric exercise training” Not arguing against effectiveness or eccentrics- but healing may not be the end result…..

27
NEED ANOTHER STUDY HERE

28
Conclusion: “Limited evidence exists to suggest that EE has a positive effect on clinical outcomes such as pain, function, and patient satisfaction/ return to work when compared to various control interventions such as concentric exercises, stretching, splinting, friction, and ultrasound.” “ This review demonstrates a dearth of high quality research in support of the clinical effectiveness of EE over other treatments in the management of tendinopathies. Further adequate powered studies…. Are required”

29
Does needling a tendon lead to healing?

30
Basic science of needling
Eliasson et al, 2013, FASEB Needling an unloaded rat Achilles tendon induced same gene expression as early mechanical loading Mechanical loading may heal, at least in part, by micro trauma Dallaudiere et al, 2013, Eur Radiology, RCT on rat model of PRP vs Serum Had clinically significant improvement in PRP group vs serum group on joint motion, ultrasound appearance, and histology Tendon healing demonstrated as opposed to just clinical pain relief

31
COULD USE MORE DATA HERE

32
Early literature on ultrasound guided needle tenotomy for lateral epicondylosis
McShane et al, Journal of Ultrasound Med. 2006 Ultrasound guided PNT with steroid for chronic lat. epicondylitis Failed conservative tx 58 pts-- avg f/u 28 mo. 80 % Good or Excellent Outcome 85% would refer friend or family for procedure McShane et al, Journal of Ultrasound Med 2008 Ultrasound guided PNT without steroid for chronic lat. Epicondylitis Failed conservative tx 57 pts --avg f/u 22 mo. 92% Good or Excellent Outcome 90% would refer friend or close relative for procedure

33
PRP for chronic lateral epicondylosis
AJSM, 2006 140 pts evaluated for lateral epicondylosis 20 had refractory pain an avg. of 15 months later 15 in treatment group, 5 in bupivicaine control group Intervention Injection w/ autologous PRP once into common extensor tendon followed by gradual increase in rehab program through 4 weeks after which full activity allowed Outcome A 46%, 60% and 81% improvement in VAS pain scores at 1, 2 and 6 months respectively in tx group 3/5 in bupivicaine group withdrew/ sought other tx At final F/U (12-38 months) 93% pain free (<10/100 VAS) No complications, no one got worse
 93% pain free (<10/100 VAS) No complications, no one got worse.")
34
13 RCT included in the study
British Medical Bulletin, 2014 13 RCT included in the study 886 patients 53.8% with identical PRP protocol Areas of controversy Different comparators Outcome scores FU periods Diverse injection protocols Conclusion: Pooling pain outcomes over time suggest that L+PRP ameliorates pain in the intermediate and long term compared with control interventions Low power, precision Further studies needed

37
Why are we still debating if orthobiologics works?
Need to define what we are injecting ? Platelet concentration MSC concentration Leukocyte count RBC +/ RBC – Autologous/ allogenic Need to define the procedure US guidance Needle tenotomy performed ? How many needle passes ? Rehabilitation methods Need to be studied/ validated Immobilization Timing of eccentrics May need to separate out different body parts

38
First double blind, placebo controlled, RCT on PRP
JAMA, January 13, 2010 First double blind, placebo controlled, RCT on PRP 54 randomized patients age 18 to 70 with chronic (at least 2 mo) achilles tendon pain 2 to 7 cm above calcaneus Either 6cc PRP or Saline was injected with US guidance into achilles tendon Rehab for both groups involved rest and then after 2 weeks, started on 12 week daily (180 repetitions) eccentric exercise program No sports for at least 4 weeks and then only if pain <=3/10 f/u questionnaire at weeks 6,12,24 (6 mo) AJSM, 2011
 achilles tendon pain 2 to 7 cm above calcaneus. Either 6cc PRP or Saline was injected with US guidance into achilles tendon. Rehab for both groups involved rest and then after 2 weeks, started on 12 week daily (180 repetitions) eccentric exercise program. No sports for at least 4 weeks and then only if pain <=3/10. f/u questionnaire at weeks 6,12,24 (6 mo) AJSM,")
39
AJSM, 2011 Type I and II Represent normal/ organized tissue- 1 increased most, 2 a little, 3 and 4 decreased. Types 3 and 4 disorganized tissue

40
Eccentrics done early (started at 2 wks) Both groups improved
DISCUSSION Both groups were treated with eccentrics AFTER treatment; NONE treated before treatment Big confounder in study Eccentrics done early (started at 2 wks) Both groups improved Needle? Saline? Placebo? Eccentric Exercises?
 Both groups improved. Needle Saline Placebo Eccentric Exercises")
41
RCT-- ABI(n= 70) vs PRP (n=80) 2 injections done 1 month apart
BJSM, 2011 RCT-- ABI(n= 70) vs PRP (n=80) 2 injections done 1 month apart All patients had FAILED an eccentric loading program and stretching program At 6 mo 66% success rate in PRP group 10% converted to surgery 72%success rate in ABI group 20% converted to surgery
 vs PRP (n=80) 2 injections done 1 month apart. All patients had FAILED an eccentric loading program and stretching program. At 6 mo. 66% success rate in PRP group. 10% converted to surgery. 72%success rate in ABI group. 20% converted to surgery.")
42
Double blind RCT with 1 year follow up of 100 pts
AJSM, Feb, 2010 Double blind RCT with 1 year follow up of 100 pts No ultrasound guidance was used Success defined as >25% reduction in VAS or DASH score RESULTS At 1 yr, 49% of CSI group and 73% in PRP group were successful (p<.001)
")
43
AJSM, March 2011

44
46 patients RCT- PRP vs CSI to lateral epicondyle

45
AJSM, 2013 METHODS N = 60 PRP vs Saline vs glucocorticoid (+ Lidocaine) Primary end point - change in pain using Patient-Rated Tennis Elbow Evaluation (PRTEE) at 3 months Secondary Outcomes - were ultrasonographic changes in tendon thickness and color Doppler activity UTCOMES 1. PRTEE Pain score Reduction at 3 months in all 3 groups with no statistically significant difference between the groups; At 1 month glucocorticoid reduced pain more effectively than did both saline and PRP 2. PRTEE Disability score At 1 month glucocorticoid was superior to saline and PRP At 3 months no difference 3. US eval (tendon thickness and color doppler) Glucocorticoid was more effective than PRP and saline in reducing color Doppler activity and tendon thickness 4. Pain associated with INJXN PRP = 9 > Saline = 7 > CSI = 6 Main Outcome: Neither injection of PRP nor glucocorticoid was superior to saline with regard to pain reduction in LE at 3 months
 at 3 months. Secondary Outcomes - were ultrasonographic changes in tendon thickness and color Doppler activity. UTCOMES. 1. PRTEE Pain score. Reduction at 3 months in all 3 groups with no statistically significant difference between the groups; At 1 month glucocorticoid reduced pain more effectively than did both saline and PRP. 2. PRTEE Disability score. At 1 month glucocorticoid was superior to saline and PRP. At 3 months no difference. 3. US eval (tendon thickness and color doppler) Glucocorticoid was more effective than PRP and saline in reducing color Doppler activity and tendon thickness. 4. Pain associated with INJXN. PRP = 9 > Saline = 7 > CSI = 6. Main Outcome: Neither injection of PRP nor glucocorticoid was superior to saline with regard to pain reduction in LE at 3 months.")
46
Comparison of studies Krogh PRP CSI CSI PRP The regeneration of tissue is a process that last more than 3 months Results of PRP can not be adequately measured with only 3 months follow-up

47
Comparison of studies Krogh PRP CSI CSI Ferrero PRP The regeneration of tissue is a process that last more than 3 months Results of PRP can not be adequately measured with only 3 months follow-up

48
Is it the Needle? AJSM, 2013

51
Measured results using Shoulder Pain and Disability Index
Clinical Rehabilitation, 2012 2 PNT vs 2 PRP injections under US guidance for RTC tendinosis or small, partial tear Measured results using Shoulder Pain and Disability Index Baseline 2wks after 1st injection Right before second injection 2 wks after second injection 3 months 6 months

52
Greater than 6 months of pain (avg 36 months)
PMR journal, 2013 Pts age (avg 48 yrs) Greater than 6 months of pain (avg 36 months) Diagnosed by clinical exam plus MRI or diagnostic US ALL had Failed conventional treatments (not controlled) Medications Bracing Stretching PRP done under US guidance Patients either sent to PT or instructed to do HEP after treatment Strengthening CFM Modalities
 Greater than 6 months of pain (avg 36 months) Diagnosed by clinical exam plus MRI or diagnostic US. ALL had Failed conventional treatments (not controlled) Medications. Bracing. Stretching. PRP done under US guidance. Patients either sent to PT or instructed to do HEP after treatment. Strengthening. CFM. Modalities.")
53
Distribution of Tendons
Lateral Epicondyle Patella Tendon Achilles Rotator Cuff Hamstring 17 Gluteus Medius 16 Medial Epicondyle 11 Plantar Fascia 9 13 other tendons <5 each

54
Overall Improvement 82% reported moderate to complete improvement
65% mod-complete in non tendon group 82% reported moderate to complete improvement – 50%- 100% relief of symptoms 70 % reported mostly to complete improvement % relief of symptoms NO difference in outcomes in those who did PT vs No Therapy after treatment.

55
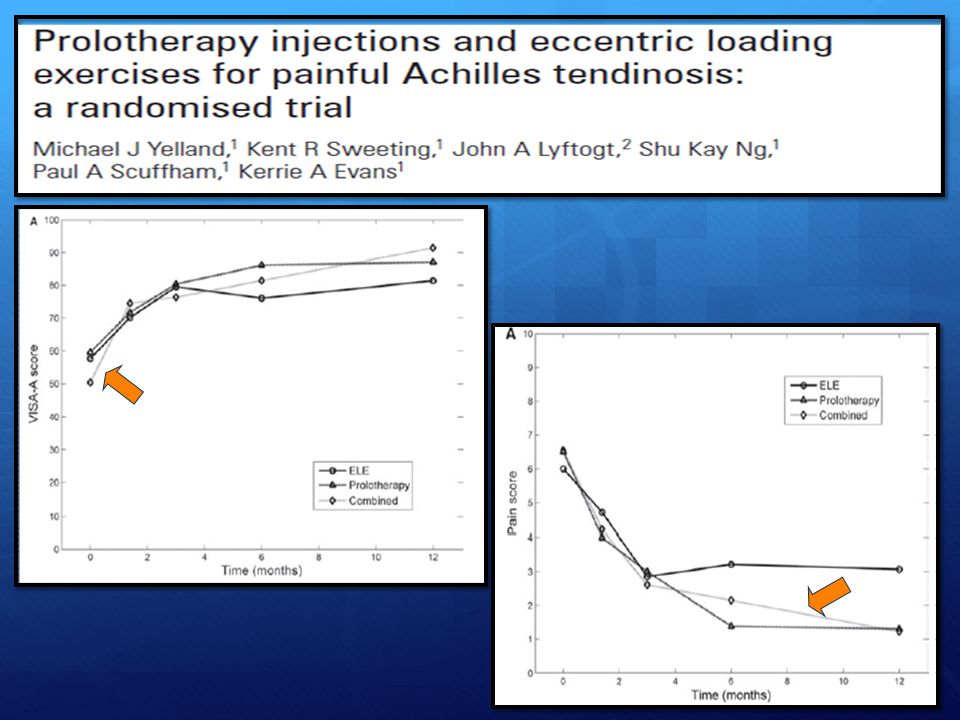
RCT with 43 patients randomized to 1 of 3 groups
BJSM, 2009 RCT with 43 patients randomized to 1 of 3 groups 12 week Eccentric training protocol (15) Prolotherapy with hypertonic glucose/ lidocaine (14) Combination of both EE + Prolo (14) Outcomes looked at Pain Function Stiffness/ limiation of activities Cost
 Prolotherapy with hypertonic glucose/ lidocaine (14) Combination of both EE + Prolo (14) Outcomes looked at. Pain. Function. Stiffness/ limiation of activities. Cost.")
57
Long term efficacy similar in all 3 groups, but ELE combined with prolo gave more rapid improvement in symptoms. Cost effectiveness analysis shows that ELEs was the lowest cost treatment, but when combined with prolotherapy, the cost per additional responder was exceptionally good value for money

58
Take Home points There are a certain percentage of tendons that will not improve with rehabilitation alone Corticosteroids offer only short term improvement in tendinosis and may provide long term detriment Level 1 studies demonstrating lavage/ aspiration of calcific tendinosis of shoulder is a successful intervention Basic science suggests that needling a tendon can lead to a healing response Emerging data that US guided needle tenotomy +/- PRP is successful for recalcitrant tendinopathies

59
Thank You

60
Outline Need for treatments beyond PT/ rehab No cortisone
History of tenotomy/ prolotherapy Basic science of how it works Level 1 data- dbrct showing positive benefits and those that do not!!!!

Similar presentations


















>")
>")





, Kaalund S.(3), Christensen M.(1),>")