Download presentation
Presentation is loading. Please wait.

1
VCU Death and Complications Conference

2
Introduction Complication Procedure Primary Diagnosis
Readmission, delayed diagnosis of colon perforation Procedure Hartmann’s procedure Primary Diagnosis ESRD s/p living donor kidney transplant Give a synopsis of each case to start the presentation.

3
Clinical History 58 yo man with DM1, and ESRD s/p living donor kidney transplant 2/21. Readmitted on 4/1 for syncope. Pt states that he got lightheaded when he got up to go to the restroom after eating dinner. He passed out and hit his head on the floor. PMH: HTN, DM1, ESRD s/p LDKT, hypothyroid, HLD, CAD, diverticulosis on colonoscopy 12/2011. PSH: LDKT Meds: amlodipine, carvedilol, insulin pump, esomeprazole, levothyroxine, prednisone, cellcept, tacrolimus, senna, SOC: 36 pack year tob, quit 2 years ago Allergic to PCN Prednisone 15mg

4
Hospital Course BP 132/70, HR 84, afebrile Phys exam:
Alert, oriented, comfortable Normal respirations, CTAB NSR, Not tachycardic, no diaphoresis Abdomen soft, nondistended, mild ttp bilateral lower quadrants WBC 11.6, hgb 10.8, electrolytes normal Syncope workup Orthostatic hypotension, 30mm Hg difference in BP On further discussion c/o crampy abdominal pain Acute series Initial workup included orthostatic blood pressures, drug levels, held BP meds, carotid doppler, EKG, cardiac enzymes, chest xray, c spine xray, kidney US. The pt mentioned crampy abdominal pain that started after eating the hamburger and fries the previous night. No N/V. No fevers. Last BM was two days ago. Pt passing gas. Acute series was ordered.

5
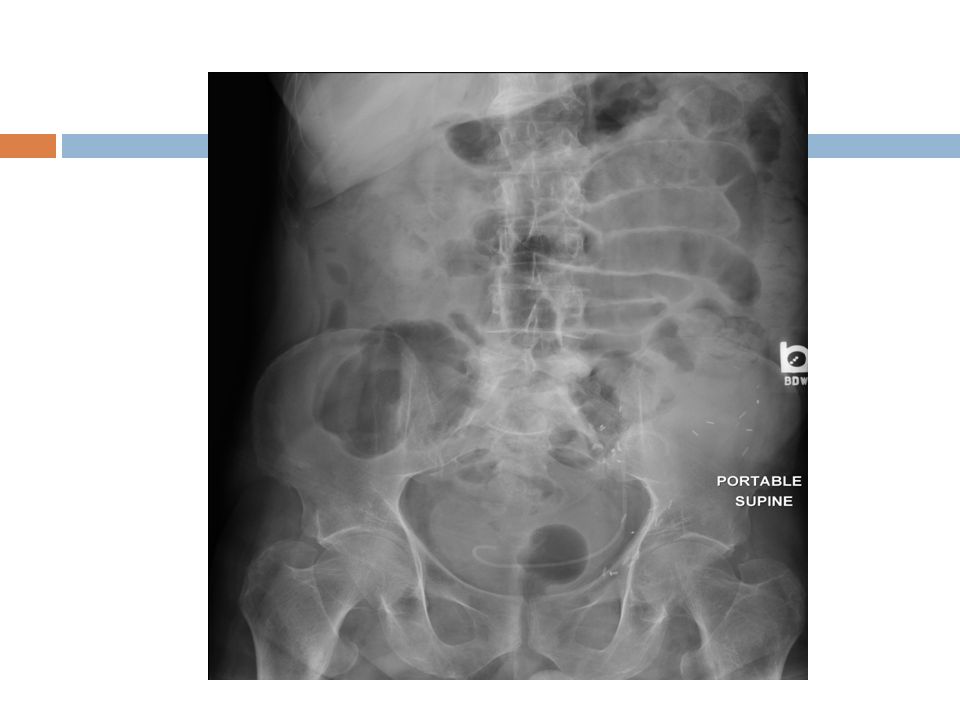
Hospital Course 4/1/12 Indication: Status post kidney transplant T12, elevated white count and abdominal pain with cramping. Assess. The chest x-ray shows normal size heart with mild tortuosity of aorta. There is subsegmental atelectasis in the right lung base. There are multiple mild moderately dilated small bowel loops in the abdomen with mild dilatation of the cecum. The remainder the colon is relatively decompressed with stool in the descending colon. Is no evidence of free air. There are mild degenerative changes lumbar spine. Conclusions: 1. Mildly dilated small bowel loops. May be seen with early partial obstruction or postop ileus. Followup recommended No evidence of free air or organomegaly. 2. Postoperative changes from renal transplant left iliac fossa

6
Hospital Course 4/1/12 Indication: Status post kidney transplant T12, elevated white count and abdominal pain with cramping. Assess. The chest x-ray shows normal size heart with mild tortuosity of aorta. There is subsegmental atelectasis in the right lung base. There are multiple mild moderately dilated small bowel loops in the abdomen with mild dilatation of the cecum. The remainder the colon is relatively decompressed with stool in the descending colon. Is no evidence of free air. There are mild degenerative changes lumbar spine. Conclusions: 1. Mildly dilated small bowel loops. May be seen with early partial obstruction or postop ileus. Followup recommended No evidence of free air or organomegaly. 2. Postoperative changes from renal transplant left iliac fossa

8
Hospital Course 2/21/12 CXR from 2/21: Persistent opacity noted at the right cardiophrenic angle consistent with fat within morganii hernia, better delineated on abdominal CT dated 9/27/11

9
Hospital Course Pt continued to be orthostatic, afebrile, tolerated clears and full liquid diet, +flatus, no BM Continued intermittent complaint of abdominal pain WBC 12.8, 12.6 CT abdomen obtained on 4/3

10
CT scan 1. Status post left lower quadrant renal transplant with nephroureteral stent in place. No evidence of hydronephrosis or perinephric fluid. 2. Free intraperitoneal air and multiple collections of free intraperitoneal fluid, findings consistent with bowel perforation. A collection of free air and fluid in the left lower quadrant medial to the transplant kidney, measuring 5.1 cm AP x 5.6 cm transverse, with tract extending inferiorly and medially to the distal sigmoid colon. Additional free air is seen underneath the anterior abdominal wall, adjacent to the liver and extending into the patient's known fat-containi ng morganii hernia. This is likely related to diverticulitis as there are numerous diverticula in this region and there is adjacent fat stranding. Iatrogenic perforation is not excluded. 3. Stable low-attenuation lesions in the liver, consistent with cysts. 4. Bilateral renal atrophy with stable hypoattenuating renal lesions, incompletely characterized on this noncontrast study. Large cyst lower pole left kidney. 5. Small hiatal hernia. No evidence of bowel obstruction. 6. Interval development of trace bilateral pleural effusions. 7. Remainder stable.

11
CT scan

12
CT scan

13
CT scan

14
Hospital Course Taken to OR that night
Perforated sigmoid colon with many diverticula Sigmoid colectomy, Hartman’s pouch, end colostomy Subsequent improvement in BP, orthostasis, WBC, abdominal pain Uneventful recovery, discharged on POD #7

15
Analysis of Complication
Was the complication potentially avoidable? Yes, could have avoided transplantation and immunosuppression; could have removed the sigmoid prior to transplant; could have diagnosed the problem sooner Would avoiding the complication change the outcome for the patient? Yes. Avoid syncope/fall/readmission, avoid ostomy; less pain, shorter hospital stay What factors contributed the complication? Presence of sigmoid diverticula, immunosuppression, diet Error in diagnosis Error in judgment Error in technique Nature of disease Systems error

16
Complicated Diverticulitis in the Transplant Patient
Complicated Diverticulitis: diverticular disease associated with abscess, phlegmon, fistula, stricture, bowel obx, peritonitis. Immunocompromised patients: Atypical signs/symptoms More likely to have free perforation Less likely to respond to conservative management Higher postoperative risk of complications and death

17
Possible contributing factors:
History of diverticulosis/diverticulitis Immunosuppression, especially high dose steroids Infection (CMV, mucormycosis) Polycystic kidney disease Age over 50 yo BASED ON MANY SMALL STUDIES LITTLE DEFINITIVE EVIDENCE
 Polycystic kidney disease. Age over 50 yo. BASED ON MANY SMALL STUDIES LITTLE DEFINITIVE EVIDENCE.")
18
Retrospective review of 875 renal transplant patients 1986-2004
8 patients with colon perforation (0.9%) Methods: analyzed age, gender, steroid dosage, time interval from transplantation, clinical presentation, delay between symptom onset and surgery, surgical procedure, graft/patient outcomes University of Parma, in parma italy
 Methods: analyzed age, gender, steroid dosage, time interval from transplantation, clinical presentation, delay between symptom onset and surgery, surgical procedure, graft/patient outcomes. University of Parma, in parma italy.")
19
Results Mean age: 58.5 Presentation: fever, abdominal pain, localized or diffuse peritonitis, leukocytosis in 7 of 8 patients All c/o constipation prior to presentation Steroid dose: 3 pts were on steroid-free immunosuppression 5 on steroids, 2 pts were on steroid dose >20mg Mean 4.1 year interval between transplant and perforation 2 patients within 1 month of transplant 6 between 1 year and 15 years

20
Procedures, outcomes 7 of 8 patients taken to the OR within 48 hrs of onset Hartmann’s procedure: 5 of 8 cases 1 patient underwent ostomy closure within 6 months 3 patients refused ostomy takedown Resection with primary anastomosis: 2 cases No fecal contamination present No complications Primary repair of perforation: 1 case Mortality: 12.5% (one patient) Outcome: at 6.1 year median follow up, 6 surviving patients (75%) surviving, 5 functioning grafts
 Outcome: at 6.1 year median follow up, 6 surviving patients (75%) surviving, 5 functioning grafts.")
21
Conclusions Aggressive diagnostic and treatment approach
Hartmann’s procedure Primary anastomosis with or without protective ileostomy may be used in selected patients Steroid sparing immunosuppressive regimen Prevent constipation

22
Retrospective review:1,137 renal transplant patients
Complicated Diverticulitis Following Renal Transplantation Lederman, et al, Department of Surgery, Albany Medical College, Albany, New York Diseases of the Colon Rectum, May 1998 Retrospective review:1,137 renal transplant patients 1.1% (13 pts) with complicated diverticulitis 25 days to 14 yrs after transplant Atypical presentation (2 asymptomatic) From asymptomatic pneumoperitoneum (2 patients) to generalized peritonitis Complicated diverticulitis: free perforation, abscess, phlegmon, fistula (stricture disease, bowel obstruction, peritonitis) PKD: 5.6 % of PKD patients end up with perfed diverticulitis 27 year review Almost half the pts in this study had PKD The addition of cyclosporin reduced colon perf rates in half, though not SS The first 388 patients ( ) received prednisone and azathioprine, with cyclosporine added to the immunosuppressive regimen for the subsequent 823 recipients ( ). Clinical presentation was highly variable, ranging from asymptomatic pneumoperitoneum (2 patients) to generalized peritonitis. Patients with polycystic kidney disease as the cause of renal failure had a significantly higher rate of complicated diverticulitis. Neither treatment with cyclosporine nor donor source had a significant effect on the rate of diverticular complications Complicated diverticulitis following renal transplantation is rare, and the clinical presentation may be atypical in the immunosuppressed transplant recipient. pretransplant screening and prophylactic sigmoid resection in this high-risk population deserve consideration and further study
 with complicated diverticulitis 25 days to 14 yrs after transplant. Atypical presentation (2 asymptomatic) From asymptomatic pneumoperitoneum (2 patients) to generalized peritonitis. Complicated diverticulitis: free perforation, abscess, phlegmon, fistula (stricture disease, bowel obstruction, peritonitis) PKD: 5.6 % of PKD patients end up with perfed diverticulitis. 27 year review Almost half the pts in this study had PKD. The addition of cyclosporin reduced colon perf rates in half, though not SS. The first 388 patients ( ) received prednisone. and azathioprine, with cyclosporine added to the. immunosuppressive regimen for the subsequent 823 recipients. ( ). Clinical presentation was highly variable, ranging from. asymptomatic pneumoperitoneum (2 patients) to generalized. peritonitis. Patients with polycystic kidney disease as the. cause of renal failure had a significantly higher rate of. complicated diverticulitis. Neither. treatment with cyclosporine nor donor source had a significant. effect on the rate of diverticular complications. Complicated diverticulitis following renal transplantation is rare, and the clinical presentation. may be atypical in the immunosuppressed transplant recipient. pretransplant screening and prophylactic. sigmoid resection in this high-risk population deserve consideration and further study.")
23
Associated factors PKD etiology of renal failure (46% of pts)
Reported elsewhere, no clear explanation Cyclosporin Age over 50 Diverticulosis pre transplant Small patient volume, most of these numbers did not approach significance The addition of cyclosporin reduced colon perf rates in half, though not SS

24
Operative intervention:
10 sigmoidectomy, end colostomy +/- mucus fistula 1 primary anastomosis 1 primary with diverting colostomy 1 primary diversion with later resection and anastomosis Outcomes 6 pts had colostomy reversal within one year One death (MI POD#6) All survivors had graft function at 5 years Graft survival in all pts except for one who died post op day 6 of an MI
 All survivors had graft function at 5 years. Graft survival in all pts except for one who died post op day 6 of an MI.")
25
Conclusions High index of suspicion Early operative intervention
Immunosuppressed with mild abdominal pain, no pertionitis PKD Known diverticulosis Early operative intervention Sigmoid colectomy with end colostomy

26
Summary of Conclusions/ Recommendations:
Prevention: steroid sparing immunosuppressive regimen, fiber diet, prevent constipation High index of suspicion for intra-abdominal catastrophe in spite of benign exam Treatment: aggressive diagnostic and treatment approach, early CT scan, early surgical intervention, decrease immunosuppression, broad spectrum antibiotic coverage, evaluate for infectious etiology Hartman’s procedure preferred, especially if stool spillage

27
Learning Points Have an elevated level of concern for abdominal pain in immunosuppressed patients, early CT scan. Do not just watch clinically. Recognize Morgagni hernia. Surgical management is best for diverticular disease in immunosuppressed patients, especially if any spillage.

28
Hinchey Stage 1: small, confined pericolic or mesenteric abscess
Stage 2: larger abscess, often confined to pelvis Stage 3: perforated diverticulitis, ruptured abscess, purulent peritonitis Stage 4: ruptured diverticulitis with fecal contamination of the peritoneal cavity Stage 1 or 2 risk of death is less than 5% Stage 3: 13% Stage 4: 43% Stage 1 or 2: may be drained Stage 3 or 4: Indications for emergent surgery: generalized peritonitis, uncontrolled sepsis, uncontained visceral perforation, large/undrainabel abscess, lack of improvement or deterioration within 3 days of medical management

29
Helderman JH: Colonic screening prior to renal transplantation and its impact on post-transplant colonic complications. Clin Transplant 6:91–96, 1992 Review of 1186 renal transplants pretransplantation colonic screening of pts >50yo was ineffective in predicting posttransplantation colonic complications 20 cases of diverticular disease identified among older patients >25% associated with adult polycystic disease. No pretransplantation colectomy No posttransplantation symptomatic colon disease Recommendation: abandon pretransplantation colonic screening in asymptomatic patients >50 yr of age. Screening should be done selectively in certain transplant candidates Pts with PKD, with documented active diverticulitis, symptomts suggestive of diverticular disease Gastrointestinal Complications of Transplant Immunosuppression. Helderman,JH. Jnl Am Soc Nephrol 13: 277–287, 2002 performed at Vanderbilt University

Similar presentations