Download presentation
Presentation is loading. Please wait.

1
Portland Gastroenterology Center
Diverticulosis Andreas Stefan MD Portland Gastroenterology Center Maine Medical Center March 21, 2015

2
Overview Epidemiology Pathophysiology Diverticulitis Bleeding
Segmental Colitis Associated with Diverticulosis (SCAD) Symptomatic Uncomplicated Diverticular Disease (SUDD)
 Symptomatic Uncomplicated Diverticular Disease (SUDD)")
3
Epidemiology Age – In the United States Male/female incidence the same
1/3 by age 60 2/3 by age 85 Male/female incidence the same Diet – low fiber, high meat and sugar Uncommon in Southeast Asia and Africa Very common in Australia, US, Europe and Canada Immigration studies (Africans moving to Sweden) First report of surgery for diverticular disease by Mayo 1907 R sided in Asia – e.g Singapore 75% R side vs 25 sigmoid Moving data: Africans/Asians to Sweden hospitalization gap went away after 10 years; Japanese moving to Hawaii
 First report of surgery for diverticular disease by Mayo R sided in Asia – e.g Singapore 75% R side vs 25 sigmoid. Moving data: Africans/Asians to Sweden hospitalization gap went away after 10 years; Japanese moving to Hawaii.")
5
Why does diverticulosis develop?

6
Pathogenesis of Diverticulosis
Exaggerated segmental contractions Laplace’s law P = kT/R (sigmoid colon is narrowest portion of colon) Patients with diverticular disease demonstrate higher pressures in colon than controls Old theory speculated that local trauma by stool contents that may injure the wall of colon – e.g. seeds, nuts etc . . . Typical diverticulum is in fact a pseudodiverticulum since not all layers are contained (no muscularis propria)
 Patients with diverticular disease demonstrate higher pressures in colon than controls. Old theory speculated that local trauma by stool contents that may injure the wall of colon – e.g. seeds, nuts etc Typical diverticulum is in fact a pseudodiverticulum since not all layers are contained (no muscularis propria)")
7
Segmental Contraction

8
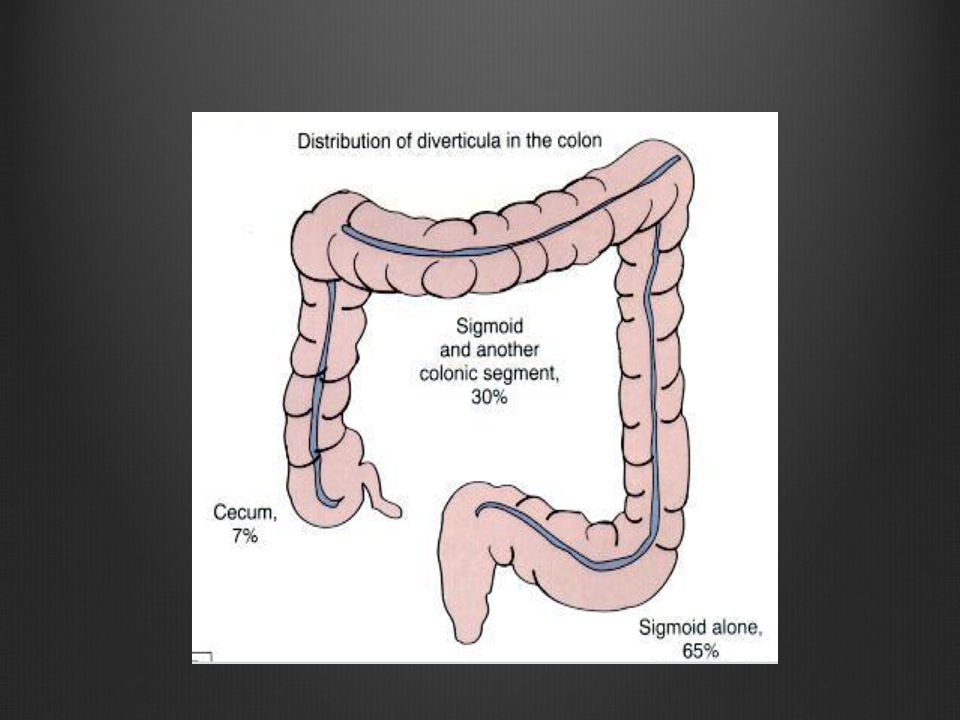
Etiology of Diverticulosis
Diverticuli don’t arise randomly around the circumference of the colon; 4 rows between mesenteric side of taenia libra and omentalis and not in anti mesenteric intertaenial area

9
Diverticulitis

10
Colonic Anatomy

11
Risk of Diverticulitis

12
Clinical Presentation
Symptoms Fever and/or chills 50% time Left lower quadrant or lower abdominal pain Change in bowel habits Urinary symptoms including dysuria or pneumaturia (no hx diverticulitis in many) Presence of localized or generalized peritonitis (micro/macroperforation) R sided disease can mimic appendicitis R sided diverticulitis can mimc appendicitis
 Presence of localized or generalized peritonitis (micro/macroperforation) R sided disease can mimic appendicitis. R sided diverticulitis can mimc appendicitis.")
13
Diagnosis Labs frequently show elevated WBC
Role of colonoscopy limited CT scan valuable Typically looking for 2 of 3 elements to establish diagnosis: symptoms, labs, and or CT One study with 45% normal WBC

14
Diagnosis Computed Tomography (CT)
CT Scan with contrast – diagnostic test of choice with sensitivity of 94% and specifity 81% in pts with classic symptoms Reliably shows the segment of bowel and the extent of disease Identifies abscess and fistula formation Reveals involvement of adjacent organs such as the small bowel, bladder and abdominal wall Can be used to guide percutaneous drainage Can be used to classify severity of diverticulitis

15
CT classification or grading
Modified Hinchey Staging – Originally based on clinical findings at surgery Stage 0: LLQ pain, elevated WBC, fever, no confirmation by imaging or surgery Stage Ia: Confined pericolic inflammation or phlegmon Stage Ib: Confined pericolic abscess Stage II: Pelvic, distant intraabdominal or retro-peritoneal abscess Stage III: Generalized purulent peritonitis Stage IV: Generalized feculent peritonitis

16
Stage 0 Often seen by PCP, GI or ER
Generally treated with oral antibiotics Cipro/Flagyl, Bactrim Augmentin, Avelox Low residue diet initially High fiber diet once symptoms resolve Need for interval colonoscopy being questioned

17
Stage Ia

18
Follow up of Stage 0 and Ia
Careful history regarding prior attacks including number, frequency, severity, and comorbidities including immunosuppression Interval colonoscopy to rule out malignancy High fiber diet <25% will have second attack Risk of third attack >50% after second attack Resection for patients with multiple attacks

19
Stage Ib or II Percutaneous drainage if possible
Transrectal drainage of pelvic abscess IV antibiotic Close clinical observation Affords possibility of single stage operation

20
Stage Ib or II Complicated Diverticulitis
Close follow up to assure resolution of symptoms and monitor for recurrence Interval colonoscopy to rule out malignancy Segmental resection with primary anastomosis 4-6 weeks after episode Risk of recurrence if managed conservatively secondary to complications of diverticulitis (abscess, stricture or fistula) MN study 42% pts not undergoing resection developed recurrent problems over 7 years (comorbidities) 2006 American Society of Colon and Rectum Surgeons guideline for resection Gaertner WB Dis Col Rectum 2013
 MN study 42% pts not undergoing resection developed recurrent problems over 7 years (comorbidities) 2006 American Society of Colon and Rectum Surgeons guideline for resection. Gaertner WB Dis Col Rectum")
21
Stage III and IV Complicated Diverticulitis
Can be difficult to distinguish on CT Scan or clinically Generalized or Localized Peritonitis Sepsis Fever Elevated WBC

22
Stage III and IV Complicated Diverticulitis
Usually require emergent operative intervention Hartman’s Procedure (1921) Colostomy with closure of distal bowel Primary anastomosis with diverting loop ileostomy in select cases Laparoscopic lavage with drainage and interval sigmoid colectomy
 Colostomy with closure of distal bowel. Primary anastomosis with diverting loop ileostomy in select cases. Laparoscopic lavage with drainage and interval sigmoid colectomy.")
23
Stage III and IV Complicated Diverticulitis

24
Stage III or IV Complicated Diverticulitis
Requires a second operation to restore intestinal continuity High percentage of patients never have them reversed (25- 70%) Morbidity associated with stomas Change in body image Difficulty with stomal pouching Peristomal hernia Stomal retraction Stomal prolapse
 Morbidity associated with stomas. Change in body image. Difficulty with stomal pouching. Peristomal hernia. Stomal retraction. Stomal prolapse.")
25
Indications for Elective Resection
After two episodes one should seriously consider elective resection Immunosuppression Ib and above disease Fistula Stricture

26
Colonic Fistulas Complicated Diverticulitis
Colo-cutaneous fistula May be a consequence of percutaneous drainage of pericolic abscess Colo-vesicular fistula 50% of patients will not remember having diverticulitis Men > Women Pneumaturia, fecaluria, frequent UTI’s Colo-vaginal fistula Generally seen in post hysterectomy female Sigmoid adhesions to the pelvis

27
Colonic Fistula Complicated Diverticulitis
Rarely a cause for emergent surgery Patient often improves with fistula formation IV antibiotics Await decrease in inflammation

28
Colonic Stricture Complicated Diverticulitis
Usually due to adhesion formation or as a result of recurrent inflammation and scarring Often difficult to distinguish from Crohn’s disease or carcinoma on imaging May be asymptomatic and identified at the time of colonoscopy Diagnosis may be accomplished with barium enema or CT with retrograde contrast If diagnostic uncertainty then surgical resection is recommended

29
Colonic Stricture

30
Can we eat Seeds, Nuts and Popcorn?

31
Can we eat Seeds, Nuts and Popcorn?
Recommendation to avoid seeds, nuts and popcorn was a result of the theory from the 1960’s (direct trauma, obstruction) – no data Current epidemiologic data supports the intraluminal pressure model of diverticulosis However, the avoidance of seeds, nuts and popcorn persists Luminal trauma ppt of diverticulitis and bleeding; but nuts are good for you
 – no data. Current epidemiologic data supports the intraluminal pressure model of diverticulosis. However, the avoidance of seeds, nuts and popcorn persists. Luminal trauma ppt of diverticulitis and bleeding; but nuts are good for you.")
32
Can we eat Seeds, Nuts and Popcorn?
Health Professionals Follow-up Study Cohort of US men (51,529) followed prospectively from – 2004 Follow diet, life style and medical history with biennially questionaire 90% mean followup Primary endpoints diverticulitis and diverticular bleeding Strate et al, JAMA 2008
 followed prospectively from 1986 – Follow diet, life style and medical history with biennially questionaire. 90% mean followup. Primary endpoints diverticulitis and diverticular bleeding. Strate et al, JAMA")
33
Can we eat Seeds, Nuts and Popcorn?
801 incident cases of diverticulitis and 383 incident cases of diverticular bleeding Looked at nut, corn and popcorn consumption and diverticulitis and diverticular bleeding Found nut, corn and popcorn consumption did not increase the risk of diverticulitis or diverticular complications Inverse associations between nut and popcorn consumption and the risk of diverticulitis in patient’s who consumed them >2x/week Strate et al, JAMA 2008

34
Can we eat Seeds, Nuts and Popcorn?
Yes!

35
Diverticular bleeding

36
Bleeding Colonic Diverticulum

37
Clipping of Bleeding Diverticulum

38
Diverticular Bleeding
5-15% with diverticulosis will develop bleeding Usually painless and not a/w diverticulitis 50% bleeding proximal to splenic flexure Stops spontaneously majority of time Risk of second bleed 20%, third bleed 50% Bursts of larger bleeding (not small frequent)
")
39
Therapeutic Colonoscopy
Jensen et al NEJM 2000 10 of 48 patients (21%) presenting with diverticular hemorrhage had bleeding site identified Treated with injection and/or cautery No rebleeds at median f/u 30 months Colonoscopy within 12 hours of admit
 presenting with diverticular hemorrhage had bleeding site identified. Treated with injection and/or cautery. No rebleeds at median f/u 30 months. Colonoscopy within 12 hours of admit.")
40
Findings May Not Be Generalizable
High rate of bleeding site identification, other studies 5-15% Endoscopic treatment riskier given tissue thickness Bit of an outlier in terms of rebleed (other studies show rates as high as 38%)
")
41
Segmental Colitis Associated with Diverticulosis (SCAD)
")
42
Segmental Colitis Associated with Diverticulosis

43
Segmental Colitis Associated with Diverticulosis
May be asymptomatic or have hematochezia and abdominal pain – rectum spared Average age onset 62 Dx made endoscopically and histologically Interdiverticular mucosa inflamed without involvement of diverticular orifices (oppose diverticulitis or IBD) Histologically ranges from modest inflammation to prolapse to chronic inflammation with crypt abscesses and distorted crypt architecture
 Histologically ranges from modest inflammation to prolapse to chronic inflammation with crypt abscesses and distorted crypt architecture.")
44
SCAD Natural history incompletely understood
Histologically resembles IBD, infx and ischemic colitis One study 10% went on to Crohns over 6 year f/u Treatment with 5 ASA, antibiotics, probiotics, even infliximab Elevated TNF alpha

45
Terminology

46
Symptomatic Uncomplicated Diverticular Disease (SUDD)
Commonly LLQ pain often worse after eating and better with defecation of passage of flatus Overlap with IBS and question late consequence Diverticulosis may not be just an intermittent condition Surgical resection series at Mayo: 47 pt with 12 month f/u on 68%. Resolution of symptoms 77% and 88% pain free (76% of specs with acute/chronic inflammation)
")
47
Medical Treatment Options for Recurrent Diverticulitis, SCAD and SUDD
Mesalamine Rifaximin Probiotics Fiber

48
Treatment Mesalamine Given evidence of chronic inflammation in patients with diverticular disease Trepsi et el: 400 bid mesalamine x 8 wks after acute attack: 15% vs 46% relapse after 4 years vs placebo Tursi et al: continuous mesalamine 1.6g/day better than 10d/month: 78 vs 56% symptom free (SUDD) Systematic review 818 pts with uncomplicated diverticulitis or SUDD found mesalamine better at relief of symptoms Studies with limitations including lack of adequate control groups and open label design More recently PREVENT 1 and 2 and DIVA trials performed
 Systematic review 818 pts with uncomplicated diverticulitis or SUDD found mesalamine better at relief of symptoms. Studies with limitations including lack of adequate control groups and open label design. More recently PREVENT 1 and 2 and DIVA trials performed.")
49
Treatment Mesalamine (for prevention of recurrent diverticulitis)
PREVENT 1 and 2 trials 584 pts with resolved diverticulitis 1.2, 2.4 or 4.8 g mesalamine daily for 2 years No difference in recurrent attacks DIVA trial (MC, PC, DB) mesalamine better symptom response compared with placebo (probiotic no additional benefit) in pts with CT documented diverticulitis but no change in recurrent diverticulitis
 mesalamine better symptom response compared with placebo (probiotic no additional benefit) in pts with CT documented diverticulitis but no change in recurrent diverticulitis.")
50
Treatment Rifaximin Tursi et al: 218 pts recurrent diverticulitis randomized to rifaximin 400 bid 7 days per month and mesalamine 800 mg bid: combination better than placebo at symptoms relief 86 vs 49% and preventing recurrence 3 vs 18%. Meta-analysis: 64% vs 35% pts treated with rifaximin and fiber vs fiber alone were symptom free at 1 year follow up. NNT 3 for rifaximin vs placebo to achieve symptom relief

51
Treatment Probiotics Small uncontrolled studies
DIVA (looked at preventing recurrence diverticulitis) study without benefit
 study without benefit.")
52
Fiber Probably protective
0.58 RR in Health Professionals Study (n= 51,000) between highest quintile vs. lowest quintile of fiber intake > 30g fiber a day likely necessary (apple = 4 g; Low fiber initially after an attack then high (although no clear evidence this prevents future attacks) Some patients with stricturing may not tolerate a high fiber diet
 between highest quintile vs. lowest quintile of fiber intake. > 30g fiber a day likely necessary (apple = 4 g; Low fiber initially after an attack then high (although no clear evidence this prevents future attacks) Some patients with stricturing may not tolerate a high fiber diet.")
53
Conclusions Common but most don’t go on to complications such as bleeding or diverticulitis OK to eat seeds/nuts and popcorn May not just be an acute disease – consider SCAD and SUDD New treatment regimens may be effective at preventing recurrent attacks and/or reducing symptoms

Similar presentations