Download presentation
Presentation is loading. Please wait.

1
Clinic Case Alev Wilk, MD Primary Care Conference 4/28/04

2
No conflict of interest

3
Cases 49 y.o. AA woman seen with a h/o multiple musculoskeletal symptoms 49 y.o. AA woman seen with a h/o multiple musculoskeletal symptoms –Pain in lower back & neck, bilateral elbows & shoulders for months to years –PMH: Mild scoliosis, OA, lateral epicondylitis, TMJ dysfunction, left shoulder tendonitis, fibromyalgia –SH: Postal worker 5 yrs.; military service 9 yrs. –FH: possible Ehler-Danlos syndrome –PE: Musculoskeletal findings: hyperextension of MCP’s and thumbs; diffuse tenderness –Radiologic: osteoarthritic changes of the spine

4
Cases 39 y.o. woman seen for intermittent low back pain: 39 y.o. woman seen for intermittent low back pain: –10-20 year h/o low back pain worse with prolonged sitting & standing –PMH: de Quervain’s tenosynovitis, olecranon bursitis, fibromyalgia, umbilical hernia –SH: cashier; gymnast as a teenager –FH: noncontributory –PE: musculoskeletal findings: marked elbow, knee, back extension, thumb apposition –Radiologic: retrolisthesis at L3-4, mild DJD

5
Cases 27 y.o. woman seen for recurrent subluxation of her left shoulder 27 y.o. woman seen for recurrent subluxation of her left shoulder –Several year h/o of left shoulder pain with recurrent subluxations –PMH: right wrist and shoulder tendonitis –SH: school teacher; rock climbing –FH: sister with repeated shoulder subluxations –PE: musculoskeletal: hyperextension at elbows and knees. Tenderness over supraspinatus tendon. Skin: striae, hyperextensibility

6
Case summary Joint Hypermobility Joint Hypermobility Soft tissue injuries Soft tissue injuries Chronic pain Chronic pain Osteoarthritis Osteoarthritis

7
Objectives Presentation, diagnosis, prevalence of joint hypermobility syndrome Presentation, diagnosis, prevalence of joint hypermobility syndrome Relationship to associated conditions (soft tissue injury, chronic pain, osteoarthritis) Relationship to associated conditions (soft tissue injury, chronic pain, osteoarthritis) Treatment of associated conditions when present Treatment of associated conditions when present
 Relationship to associated conditions (soft tissue injury, chronic pain, osteoarthritis) Treatment of associated conditions when present Treatment of associated conditions when present")
8
Presentation Musculoskeletal symptoms in presence of joint laxity Musculoskeletal symptoms in presence of joint laxity Heritable disorder of connective tissue Heritable disorder of connective tissue Identical to the hypermobility type of Ehler-Danlos syndrome (EDS type III) Identical to the hypermobility type of Ehler-Danlos syndrome (EDS type III) Mechanism of injury: Increased ligamentous laxity; decreased joint proprioception Mechanism of injury: Increased ligamentous laxity; decreased joint proprioception
 Identical to the hypermobility type of Ehler-Danlos syndrome (EDS type III) Mechanism of injury: Increased ligamentous laxity; decreased joint proprioception Mechanism of injury: Increased ligamentous laxity; decreased joint proprioception")
9
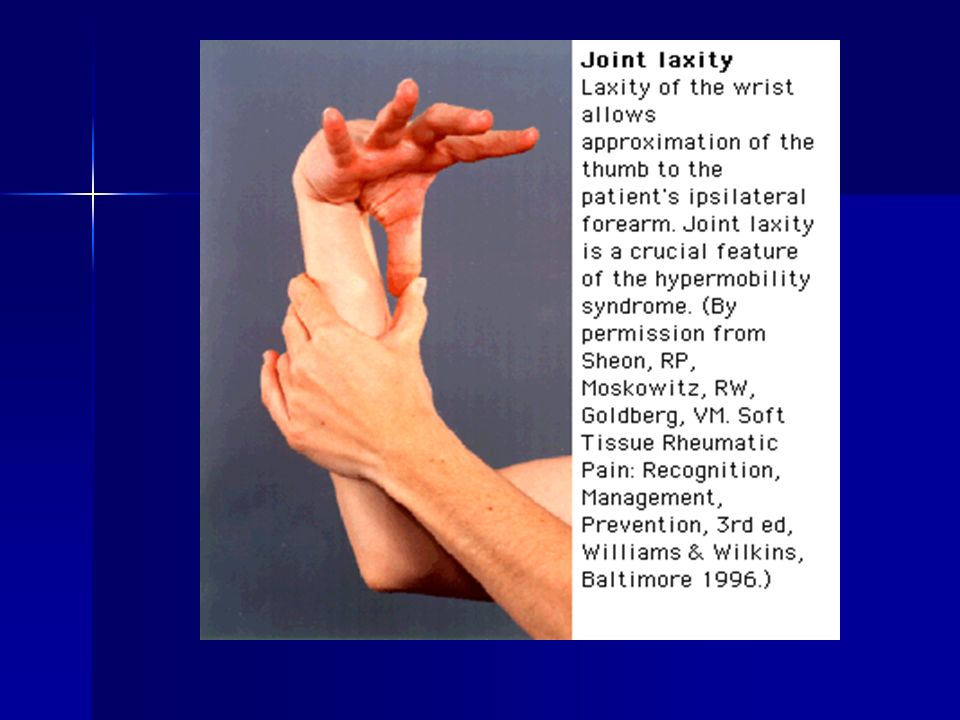
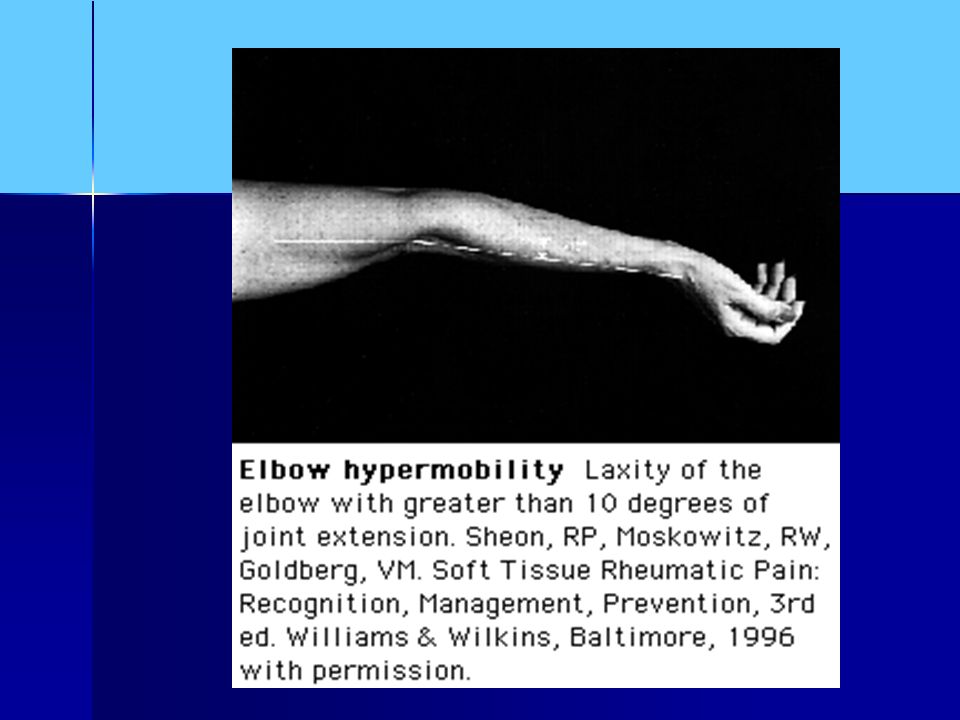
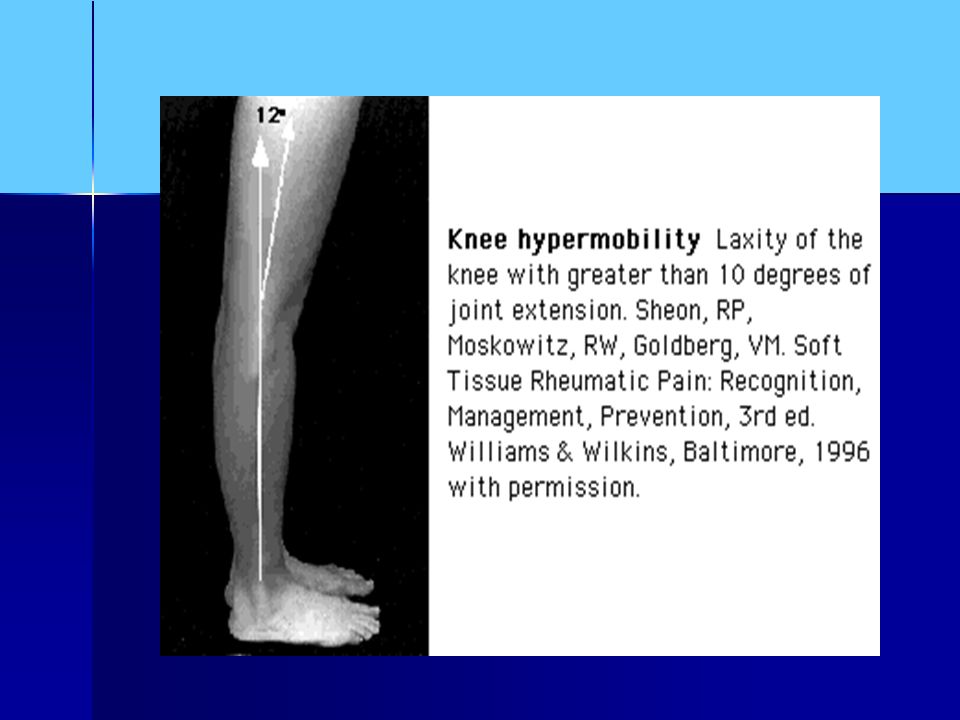
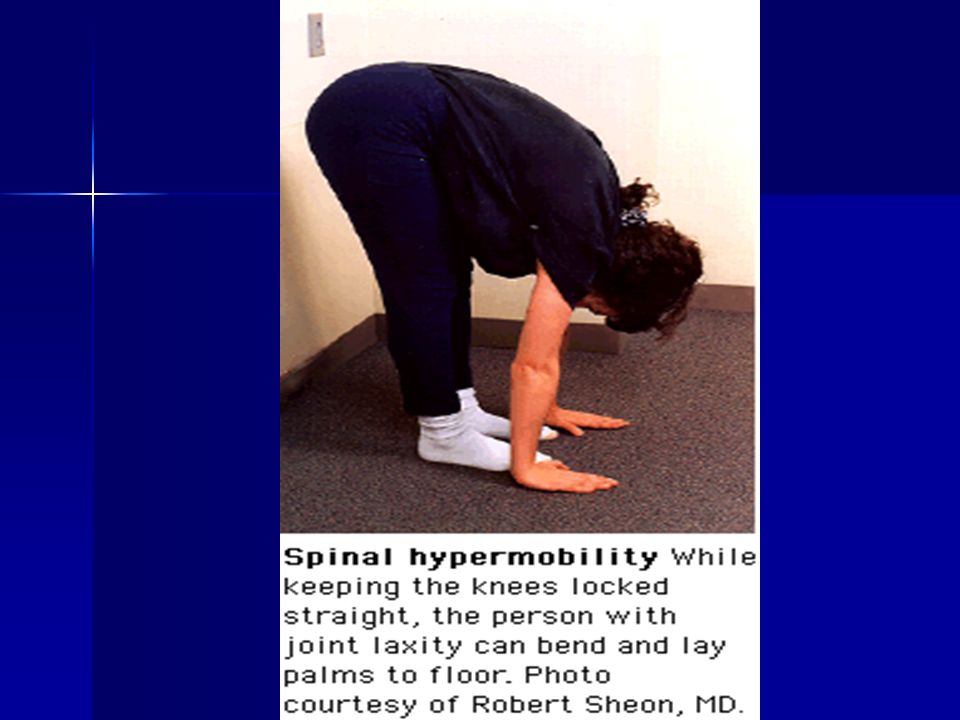
Diagnosis Nine-Point Beighton hypermobility score* Nine-Point Beighton hypermobility score* –Passive dorsiflexion of the metacarpophalangeal joint to 90 degrees –Apposition of the thumb to the flexor aspect of the forearm –Hyperextension of the elbow to > 10 degrees –Hyperextension of the knee to > 10 degrees –Forward trunk flexion with hands flat on the floor and with knees extended *Ann Rheum Dis 1973;32:413-7

14
Revised diagnostic criteria Major criteria Major criteria –Beighton score of 4/9 or greater –Arthralgia for longer than 3 months in 4 or more joints Minor criteria Minor criteria –Beighton score of 1,2 or 3/9 –Arthralgia (>3 mo) in 1-3 joints, or back pain, spondylosis, spondylolysis/listhesis –Dislocation/subluxation in more than one joint, or in one joint on more than one occasion –Soft tissue rheumatism > 3 lesions
 in 1-3 joints, or back pain, spondylosis, spondylolysis/listhesis –Dislocation/subluxation in more than one joint, or in one joint on more than one occasion –Soft tissue rheumatism > 3 lesions")
15
Revised diagnostic criteria Minor criteria continued Minor criteria continued –Maranoid habitus (tall, slim, span/height > 1.03, arachnodactyly) –Abnormal skin: striae, hyperextensibility, thin skin, papyraceous scarring –Eye signs: drooping eyelids or myopia or antimongoloid slant –Varicose veins or hernia or uterine/rectal prolapse 2 major criteria or one major and 2 minor criteria; 4 minor criteria or 2 minor and an affected first-degree relative
 –Abnormal skin: striae, hyperextensibility, thin skin, papyraceous scarring –Eye signs: drooping eyelids or myopia or antimongoloid slant –Varicose veins or hernia or uterine/rectal prolapse 2 major criteria or one major and 2 minor criteria; 4 minor criteria or 2 minor and an affected first-degree relative")
17
Prevalence 5-13% in childhood 5-13% in childhood 4-5% in the general population 4-5% in the general population 13-15% in rheumatology clinics 13-15% in rheumatology clinics Higher rates reported in women Higher rates reported in women Higher rates reported in West Africans & Middle-Eastern women Higher rates reported in West Africans & Middle-Eastern women

18
Benign Condition? Heritable Disorder of Connective Tissue Heritable Disorder of Connective Tissue Hypermobility syndrome Hypermobility syndrome Benign Joint Hypermobility Syndrome Benign Joint Hypermobility Syndrome Mechanisms Mechanisms –Increased ligamentous laxity may lead to soft tissue pain/ligamentous injury –Decreased proprioception of hypermobile joints

19
Associated conditions Tendency towards dislocation Tendency towards dislocation Traumatic synovitis Traumatic synovitis Chronic joint pain Chronic joint pain Fibromyalgia and depression Fibromyalgia and depression Premature osteoarthritis Premature osteoarthritis

20
Bridges AJ et al. Joint hypermobility in adults referred to rheumatology clinics. 130 adult patients referred to a rheumatology clinic with musculoskeletal problems 130 adult patients referred to a rheumatology clinic with musculoskeletal problems 97 women, 33 men 97 women, 33 men Beigton score > 5 out of 9 Beigton score > 5 out of 9 Exclusion criteria: signs of Ehler- Danlos syndrome (EDS) Exclusion criteria: signs of Ehler- Danlos syndrome (EDS) Annals of the Rheumatic Diseases 1992;51:793-796
 Exclusion criteria: signs of Ehler- Danlos syndrome (EDS) Annals of the Rheumatic Diseases 1992;51:")
21
Bridges AJ et al. Results 15% had joint hypermobility 15% had joint hypermobility Average Beighton score of 8; average age of 50; hypermobile features since childhood Average Beighton score of 8; average age of 50; hypermobile features since childhood All cases of hypermobility were women All cases of hypermobility were women 65% had a FH of joint hypermobility in a first degree relative 65% had a FH of joint hypermobility in a first degree relative Trunk hypermobility was noted in younger patients (average age of 37 y.o.) Trunk hypermobility was noted in younger patients (average age of 37 y.o.)
 Trunk hypermobility was noted in younger patients (average age of 37 y.o.).")
22
Bridges AJ et al. 50% had hypermobility of the fingers & ankles, 35% of the hips. 50% had hypermobility of the fingers & ankles, 35% of the hips. 85% flat feet 85% flat feet 35% scolioisis 35% scolioisis 40% soft tissue injury 40% soft tissue injury 60% OA 60% OA 30% fibromyalgia 30% fibromyalgia

23
Hudson N et al* Diagnostic associations with hypermobility in rheumatology patients. 378 consecutive referrals to a rheumatology clinic 378 consecutive referrals to a rheumatology clinic Beighton score of four or greater out of nine. Beighton score of four or greater out of nine. Assessed by physical exam and physical activity, leisure and work Assessed by physical exam and physical activity, leisure and work Brit J of Rheumatology 1995;34:1157-61

24
Hudson et al. 13.2% fulfilled criteria for hypermobility 13.2% fulfilled criteria for hypermobility 94% of the patients were women (73% in the control group); average age 45 y.o. 94% of the patients were women (73% in the control group); average age 45 y.o. 26% had tendonitis, bursitis or fasciitis (17% in the control group) 26% had tendonitis, bursitis or fasciitis (17% in the control group) 30% fit diagnositic criteria for fibromyalgia syndrome, the most frequent diagnosis (8% in the control group) 30% fit diagnositic criteria for fibromyalgia syndrome, the most frequent diagnosis (8% in the control group)
; average age 45 y.o. 94% of the patients were women (73% in the control group); average age 45 y.o. 26% had tendonitis, bursitis or fasciitis (17% in the control group) 26% had tendonitis, bursitis or fasciitis (17% in the control group) 30% fit diagnositic criteria for fibromyalgia syndrome, the most frequent diagnosis (8% in the control group) 30% fit diagnositic criteria for fibromyalgia syndrome, the most frequent diagnosis (8% in the control group).")
25
Hudson et al. 15% with axial or spinal complaints (15% in the control group) 15% with axial or spinal complaints (15% in the control group) 7% with OA (19% in the control group) 7% with OA (19% in the control group) 4% with inflammatory arthropathy (32% in the control group) 4% with inflammatory arthropathy (32% in the control group)
 15% with axial or spinal complaints (15% in the control group) 7% with OA (19% in the control group) 7% with OA (19% in the control group) 4% with inflammatory arthropathy (32% in the control group) 4% with inflammatory arthropathy (32% in the control group).")
26
Hudson et al. Pain breakdown: Pain breakdown: –Widespread in 44% –Multiple localized sites in 44% –Single site in 13% –Spinal-neck in 37% –Spinal-midthoracic & low back in 80% –Tendonitis (previous and present) in 63%
 in 63%.")
27
Living with Hypermobility* Everyday activities carry the price of pain Everyday activities carry the price of pain –ADL’s –Repetitive movement Absenteeism from work Absenteeism from work Adverse effects on family and relationships Adverse effects on family and relationships Depression & isolation from pain and disability Depression & isolation from pain and disability *Rheumatology 2001;40:487-489

28
Barriers to diagnosis and management Patients generally look well and present uniquely Patients generally look well and present uniquely Under-recognized and under- estimated Under-recognized and under- estimated Lack of a clear cause-and-effect relationship Lack of a clear cause-and-effect relationship Non-specialized physical therapy can exacerbate symptoms Non-specialized physical therapy can exacerbate symptoms

29
Treatment Specialized physiotherapy Specialized physiotherapy –Stabilizing lax joints with exercise to increase stability, reduce pain and diminish hypermobility –Improving proprioceptive acuity Drug therapy Drug therapy Cognitive-behavioral therapy Cognitive-behavioral therapy Patient support groups Patient support groups

30
Summary Joint hypermobility appears to be associated with multiple soft tissue injuries, fibromyalgia and osteoarthritis Joint hypermobility appears to be associated with multiple soft tissue injuries, fibromyalgia and osteoarthritis Joint hypermobility is relatively common in populations with & without musculoskeletal symptoms. Joint hypermobility is relatively common in populations with & without musculoskeletal symptoms. Joint hypermobility syndrome may be a true entity but like fibromyalgia is difficult to assess and treat. Joint hypermobility syndrome may be a true entity but like fibromyalgia is difficult to assess and treat.

31
References Hudson N. Fitzcharles MA. Cohen M. Starr MR. Esdaile JM. The association of soft-tissue rheumatism and hypermobility. British Journal of Rheumatology. 37(4):382-6, 1998 Apr. Hudson N. Fitzcharles MA. Cohen M. Starr MR. Esdaile JM. The association of soft-tissue rheumatism and hypermobility. British Journal of Rheumatology. 37(4):382-6, 1998 Apr. Hudson NFitzcharles MACohen MStarr MR Esdaile JM Hudson NFitzcharles MACohen MStarr MR Esdaile JM Acasuso-Diaz M. Collantes-Estevez E. Joint hypermobility in patients with fibromyalgia syndrome. Arthritis Care & Research. 11(1):39-42, 1998 Feb. Acasuso-Diaz M. Collantes-Estevez E. Joint hypermobility in patients with fibromyalgia syndrome. Arthritis Care & Research. 11(1):39-42, 1998 Feb. Acasuso-Diaz MCollantes-Estevez E Acasuso-Diaz MCollantes-Estevez E Hudson N, Starr MR, Esdaile JM, Fitzcharles MA. Diagnostic association hypermobility in Rheumatology Patients. British J of Rheumatology 1995;34:1157-1161. Hudson N, Starr MR, Esdaile JM, Fitzcharles MA. Diagnostic association hypermobility in Rheumatology Patients. British J of Rheumatology 1995;34:1157-1161. Bridges AJ, Smith E, Reid J. Joint hypermobility in adults referred to rheumatology clinics. Annals of the Rheumatic Diseases 1992;51:793-796. Bridges AJ, Smith E, Reid J. Joint hypermobility in adults referred to rheumatology clinics. Annals of the Rheumatic Diseases 1992;51:793-796.
:382-6, 1998 Apr. Hudson N. Fitzcharles MA. Cohen M. Starr MR. Esdaile JM. The association of soft-tissue rheumatism and hypermobility. British Journal of Rheumatology. 37(4):382-6, 1998 Apr. Hudson NFitzcharles MACohen MStarr MR Esdaile JM Hudson NFitzcharles MACohen MStarr MR Esdaile JM Acasuso-Diaz M. Collantes-Estevez E. Joint hypermobility in patients with fibromyalgia syndrome. Arthritis Care & Research. 11(1):39-42, 1998 Feb. Acasuso-Diaz M. Collantes-Estevez E. Joint hypermobility in patients with fibromyalgia syndrome. Arthritis Care & Research. 11(1):39-42, 1998 Feb. Acasuso-Diaz MCollantes-Estevez E Acasuso-Diaz MCollantes-Estevez E Hudson N, Starr MR, Esdaile JM, Fitzcharles MA. Diagnostic association hypermobility in Rheumatology Patients. British J of Rheumatology 1995;34: Hudson N, Starr MR, Esdaile JM, Fitzcharles MA. Diagnostic association hypermobility in Rheumatology Patients. British J of Rheumatology 1995;34: Bridges AJ, Smith E, Reid J. Joint hypermobility in adults referred to rheumatology clinics. Annals of the Rheumatic Diseases 1992;51: Bridges AJ, Smith E, Reid J. Joint hypermobility in adults referred to rheumatology clinics. Annals of the Rheumatic Diseases 1992;51:")
32
References Gurley-Green S. Living with the hypermobility syndrome. Rheumatology 2001;40:487-489. Gurley-Green S. Living with the hypermobility syndrome. Rheumatology 2001;40:487-489. Grahame R, et al. The Revised (Brighton 1998) Criteria for the Diagnosis of Benign Joint Hypermobility Syndrome (BJHS). J of Rheumatology 2000;27:7. Grahame R, et al. The Revised (Brighton 1998) Criteria for the Diagnosis of Benign Joint Hypermobility Syndrome (BJHS). J of Rheumatology 2000;27:7. Mishra MB, Ryan P, Atkinson P, et al. Extra-articular feature of benign joint hypermobility syndrome. Br J Rheumatol 1996;35:861-6. Mishra MB, Ryan P, Atkinson P, et al. Extra-articular feature of benign joint hypermobility syndrome. Br J Rheumatol 1996;35:861-6. Larsson LG, Mudholkar GS, Baum J, Srivastava DK. Benefits and liabilities of hypermobility in the back pain disorders of industrial workers. Journal of Internal Medicine 1995;238:461-467. Larsson LG, Mudholkar GS, Baum J, Srivastava DK. Benefits and liabilities of hypermobility in the back pain disorders of industrial workers. Journal of Internal Medicine 1995;238:461-467.
 Criteria for the Diagnosis of Benign Joint Hypermobility Syndrome (BJHS). J of Rheumatology 2000;27:7. Grahame R, et al. The Revised (Brighton 1998) Criteria for the Diagnosis of Benign Joint Hypermobility Syndrome (BJHS). J of Rheumatology 2000;27:7. Mishra MB, Ryan P, Atkinson P, et al. Extra-articular feature of benign joint hypermobility syndrome. Br J Rheumatol 1996;35: Mishra MB, Ryan P, Atkinson P, et al. Extra-articular feature of benign joint hypermobility syndrome. Br J Rheumatol 1996;35: Larsson LG, Mudholkar GS, Baum J, Srivastava DK. Benefits and liabilities of hypermobility in the back pain disorders of industrial workers. Journal of Internal Medicine 1995;238: Larsson LG, Mudholkar GS, Baum J, Srivastava DK. Benefits and liabilities of hypermobility in the back pain disorders of industrial workers. Journal of Internal Medicine 1995;238:")
33
References Larsson LG, Baum J, Mudholkar GS, Kollia GD. Benefits and disadvantages of joint hypermobility among musicians. N Engl J Med 1993;329:1079-81. Larsson LG, Baum J, Mudholkar GS, Kollia GD. Benefits and disadvantages of joint hypermobility among musicians. N Engl J Med 1993;329:1079-81. Fitzcharles MA. Is Hypermobility a Factor in Fibromyalgia. J of Rheumatology 2000;27:7. Fitzcharles MA. Is Hypermobility a Factor in Fibromyalgia. J of Rheumatology 2000;27:7. Al-Rawi ZS, Al-Aszawi AJ, Al-Chalabi T. Joint mobility among university students in Iraq. Br J Rheumatol 1985;24:326-31. Al-Rawi ZS, Al-Aszawi AJ, Al-Chalabi T. Joint mobility among university students in Iraq. Br J Rheumatol 1985;24:326-31. Birrell FN, Adebajo AO et al. High prevalence of joint laxity in West Africans. Br J Rheumatol 1994;33:56-9. Birrell FN, Adebajo AO et al. High prevalence of joint laxity in West Africans. Br J Rheumatol 1994;33:56-9.

Similar presentations






>")


 and pulsating in nature, lasting from 4 to 72 hours; symptoms include.>")





 standard population. Source: National Health Interview.>")



