Download presentation
Presentation is loading. Please wait.

1
Carpal Tunnel Syndrome Presented By NathaëlF Hyppolite RIII MF

2
Objectives How to evaluate the patient clinically How to treat the patient effectively When to treat surgically

3
Plan Definition Epidemiology Etiology Clinical Features Physical examination Diagnostic Differential Diagnostics Treatment

4
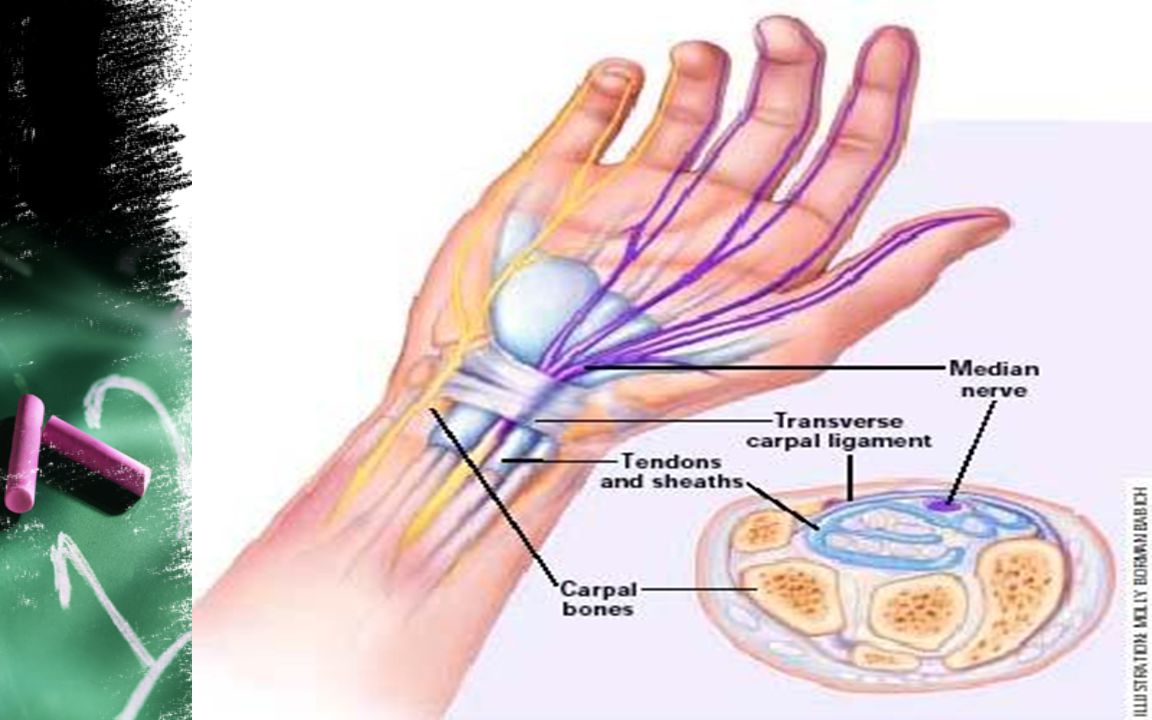
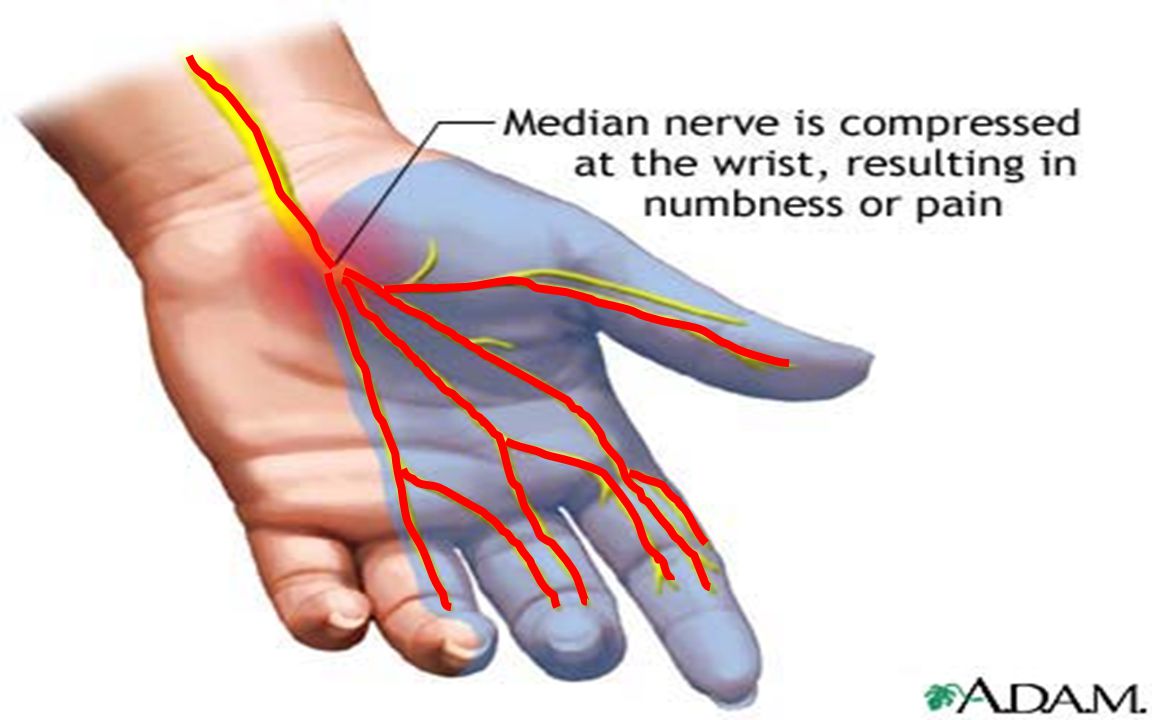
Definition Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist.

8
epidemiology Affects an estimated 3 percent of adult Americans Three times more common in women than in men High prevalence rates have been reported in persons who perform certain repetitive wrist motions (frequent computer users) 30% hand paresthesias 10% clinical criteria for carpal tunnel syndrome 3.5% abnormal nerve conduction studies
 30% hand paresthesias 10% clinical criteria for carpal tunnel syndrome 3.5% abnormal nerve conduction studies")
10
Clinical Features Pain Numbness Tingling Symptoms are usually worse at night and can awaken patients from sleep. To relieve the symptoms, patients often “flick” their wrist as if shaking down a thermometer (flick sign).
..")
12
Clinical Features Pain and paresthesias may radiate to the forearm, elbow, and shoulder. Decreased grip strength may result in loss of dexterity, and thenar muscle atrophy may develop if the syndrome is severe.

13
Atrophy

14
Physical examination Phalen’s maneuver Tinel’s sign weak thumb abduction. two-point discrimination

15
Phalen’s maneuver

16
Tinel’s sign

17
Diagnostic History Physical examination Nerve Conduction Study

18
Differential Diagnostics Tendonitis Tenosynovitis Diabetic neuropathy Kienbock's disease Compression of the Median nerve at the elbow

19
Treatment CONSERVATIVE TREATMENTS –GENERAL MEASURES –WRIST SPLINTS –ORAL MEDICATIONS –LOCAL INJECTION –ULTRASOUND THERAPY –Predicting the Outcome of Conservative Treatment SURGERY

20
GENERAL MEASURES Avoid repetitive wrist and hand motions that may exacerbate symptoms or make symptom relief difficult to achieve. Not use vibratory tools Ergonomic measures to relieve symptoms depending on the motion that needs to be minimized

22
WRIST SPLINTS Probably most effective when it is applied within three months of the onset of symptoms Optimal splinting regimen ?

23
WRIST SPLINTS

24
ORAL MEDICATIONS Diuretics Nonsteroidal anti-inflammatory drugs (NSAIDs) pyridoxine (vitamin B6) Orally administered corticosteroids –Prednisolone –20 mg per day for two weeks –followed by 10 mg per day for two weeks DO NOT WORK !!!
 pyridoxine (vitamin B6) Orally administered corticosteroids –Prednisolone –20 mg per day for two weeks –followed by 10 mg per day for two weeks DO NOT WORK !!!")
25
LOCAL INJECTION A mixture of 10 to 20 mg of lidocaine (Xylocaine) without epinephrine and 20 to 40 mg of methylprednisolone acetate (Depo-Medrol) or similar corticosteroid preparation is injected with a 25-gauge needle at the distal wrist crease (or 1 cm proximal to it).
 without epinephrine and 20 to 40 mg of methylprednisolone acetate (Depo-Medrol) or similar corticosteroid preparation is injected with a 25-gauge needle at the distal wrist crease (or 1 cm proximal to it).")
26
LOCAL INJECTION

28
Splinting is generally recommended after local corticosteroid injection. If the first injection is successful, a repeat injection can be considered after a few months Surgery should be considered if a patient needs more than two injections

29
ULTRASOUND THERAPY May be beneficial in the long term management More studies are needed to confirm it’s usefulness

31
SURGERY Should be considered in patients with symptoms that do not respond to conservative measures and in patients with severe nerve entrapment as evidenced by nerve conduction studies,thenar atrophy, or motor weakness. It is important to note that surgery may be effective even if a patient has normal nerve conduction studies

32
SURGERY Complications of surgery Injury to the palmar cutaneous or recurrent motor branch of the median nerve Hypertrophic scarring laceration of the superficial palmar arch tendon adhesion Postoperative infection Hematoma arterial injury stiffness

35
SURGERY

36
PREGNANCY Alterations in fluid balance may predispose some pregnant women to develop carpal tunnel syndrome. Symptoms are typically bilateral and first noted during the third trimester. Conservative measures are appropriate, because symptoms resolve after delivery in most women with pregnancy-related carpal tunnel syndrome.

37
Conclusion Most common focal peripheral neuropathy Pain and paresthesias in the distribution of the median nerve are the classic symptoms. While Tinel’s sign and a positive Phalen’s maneuver are classic clinical signs of the syndrome, hypalgesia and weak thumb abduction are more predictive of abnormal nerve conduction studies.

38
Conclusion Conservative treatment options include splinting the wrist in a neutral position and ultrasound therapy Orally administered corticosteroids can be effective for short-term management (two to four weeks), but local corticosteroid injections may improve symptoms for a longer period. If symptoms are refractory to conservative measures or if nerve conduction studies show severe entrapment, open or endoscopic carpal tunnel release may be necessary.

39
bibliography American family physician july 15 2003 www.aafp.org/afp Essantials of musculoskeletal care C.Cabrol anatmie tome 1

Similar presentations












 Pathology Pathology 30 – 50 years old Repetitive micro-trauma Chronic tear in the origin of the extensor.>")

 By far the most common entrapment neuropathy, especially of the upper extremity. By.>")






 SCPHN.>")


 is defined as compression of the median nerve at.>")


