Download presentation
Presentation is loading. Please wait.

2
Diabetes: What’s New? What’s Next? Robert P. Hoffman, M.D. Grand Rounds June 1, 2007

3
Introduction u Frederick Allen 1919 “The knowledge of diabetes is advancing rapidly enough that even the patient whose outlook seems darkest should take courage to remain alive in the hope of a treatment that can be called curative” u 1921 Banting and Best at the University of Toronto discovered insulin

4
DCCT u 1993 u 1441 subjects (age 13-35) randomized to intensive versus conventional therapy u Intensive diabetes therapy markedly reduces risk of long term complications in adults and adolescents u Increased risk of severe hypoglycemia u Did not tell us how to achieve good control
 randomized to intensive versus conventional therapy u Intensive diabetes therapy markedly reduces risk of long term complications in adults and adolescents u Increased risk of severe hypoglycemia u Did not tell us how to achieve good control")
5
What’s New?, What’s Next? u New insulins u New modes of delivery u New tecnology u Curative treatments u Prevention

6
New Insulins

7
Insulin Structure Zn

8
Short Acting Insulins 012345 Time Hours Insulin Glucose Normal Regular Lispro Aspart Glulysine

9
Long Acting Insulins 04812162024 Time Hours NPH/Lente INSULIN Glargine Levomir

10
Glargine Zn pH =7.4 pH =4

11
Levomir FFA

12
Intensive Insulin Regimens BfLuSuBt Lispro Glargine Levomir

13
Insulin Adjustment Morn LunchSupper Bed LP GlaLP

14
Intensive Insulin Regimens Lispro NPH BFLuSuBt

15
Intensive Insulin Regimens Lispro NPH BFLuSuBt NPH

16
Intensive Insulin Adjustment Morn LunchSupper Bed LPN N

17
Advantages of New Insulins u Better post prandial glucose control u Less nocturnal hypoglycemia u Better schedule flexibility u No major differences in overall glucose control

18
Inhaled Insulin

19
u Action profile similar to lispro u Well tolerated by subjects u Still need to take long acting u Need to work out dosing differences u Small decrease in lung diffusion capacity u Long term safety unknown

20
New Technology

21
Continuous Glucose Monitoring

22
Maia and Arau´jo; Diab Res Clin Pract 2007,

24
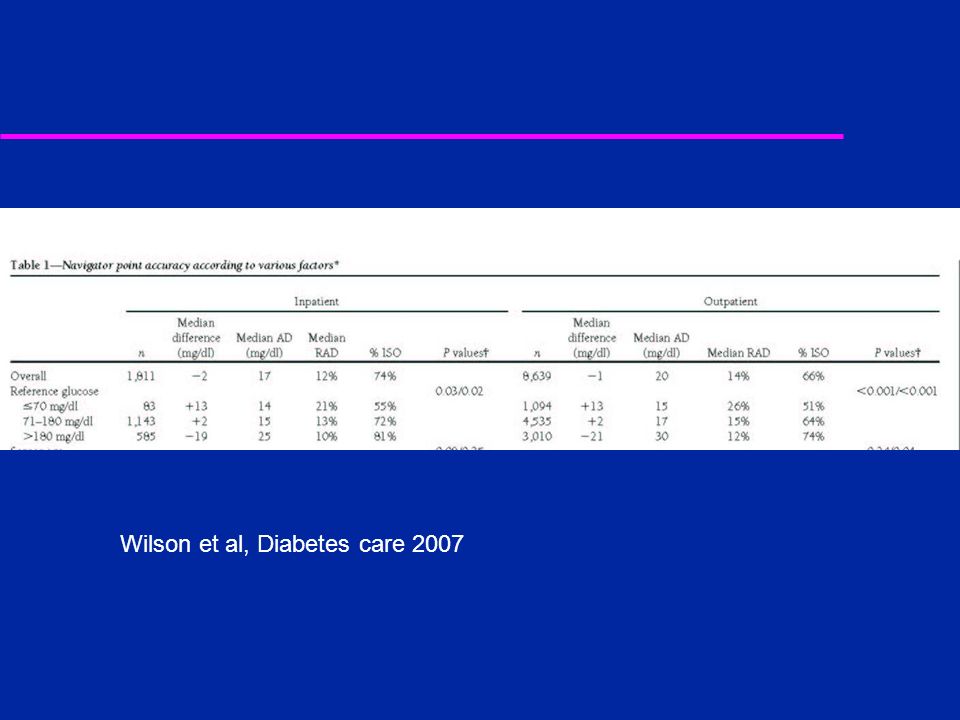
Wilson et al, Diabetes care 2007

26
Change from baseline at 1 and 3 months of AIC. Values are means SE. P values correspond to the difference in change from baseline between the continuous and control groups. F, continuous group (arm 1); f, biweekly group (arm 2); OE, control group. Deis et al Diabetes Care 2006
; f, biweekly group (arm 2); OE, control group. Deis et al Diabetes Care")
27
Insulin Pumps

28
Continuous Subcutaneous Insulin Infusion (CSII )
")
29
Insulin Pumps MiniMed

30
Infusion Sets

31
Results

32
Adolescents and Pumps White et al Diabetes 2000

33
Randomized Adult Tsui et al, Diabetes Care 2001

34
Randomized school age adolescents u Garcia-Garcia J Ped Endo Metab 2007 –At 24 months randomized study MDI versus CSII –Hemoglobin A1c was 7.70 +/- 0.64% vs 7.54 +/- 0.74% (p = 0.8); –Body mass index SDS was 0.33 +/- 0.74 vs 0.40 +/- 1.01 (p = 0.9); –Total daily insulin requirements were 0.95 +/- 0.10 vs 1.05 +/- 0.18 U/kg (p = 0.4), –Incidence of severe hypoglycemia was 0.00 +/- 0.00 vs 0.04 +/- 0.14 episodes/patient/year (p = 0.8); and –Incidence of ketoacidosis was 0.20 +/- 0.27 vs 0.04 +/- 0.14 episodes/patient/year (p = 0.2).
; –Body mass index SDS was / vs / (p = 0.9); –Total daily insulin requirements were / vs / U/kg (p = 0.4), –Incidence of severe hypoglycemia was / vs / episodes/patient/year (p = 0.8); and –Incidence of ketoacidosis was / vs / episodes/patient/year (p = 0.2).")
35
Preschool Children Fox et al Diabetes Care 2007 Wilson et al Diabetes Care 2005

36
Hypoglycemia

37
DKA-Metaanalysis Eggar Diabetic Medicine 1997

38
Advantages to CSII u Effectively treats “dawn” phenomenon –Adjust basal rate at 3 AM u No shots u Bolus for snacks without extra shot u Flexibility of meals, exercise and travel –Decreased need for snacks

39
Disadvantages to SCII u Requires more time/effort u Contact sports, swimming, bathing can be difficult u Increased risk of DKA

40
Cure

41
Pancreas Transplant u Successful –95% one year survival –70% one year insulin free u Problems –Life long immunosuppression –Donor availability u Indications –Renal failure or near renal failure –Combined pancreas kidney

42
Islet Transplantation

43
Results u Insulin free for 4 to 12 months –Normal hemoglobin A1c –Near normal glucose profiles –No complications u Problems –2 cadaver pancreases per patient –Harvesting technique critical –Required immunosuppression

44
Autologous Bone Marrow Transplant

45
Complications

46
Prevention u Diabetes Prevention Trial Type 1 –First degree relatives type 1 diabetic patients »High Risk-received subcutaneous insulin u No effect »Intermediate Risk-oral insulin ongoing enrollment u No effect u European Nicotinamide Diabetes Intervention Trial –No effect

47
TrialNet u Series of multicenter studies to prolong beta cell function or prevent type 1 diabetes u Prolong beta cell function –Anti CD3 –Anti CD20 –Anti CD3 plus GLP-1 agonist u Oral insulin

48
Conclusion u The knowledge of diabetes is advancing rapidly enough that all patients should work to maintain the best possible glycemic control to prevent complications now and in the future with the hope of new technologies and treatments that will make their task and lifestyle easier if not eliminate the disease all together.

Similar presentations



 Any Glucose Level Age Rapid onset Weight loss Tablets fail Pregnancy Illness Ketoacidosis Pancreat-ectomy.>")




. Who needs screening for DM? Age >45 Obese – BMI >25 1 st degree relative with DM Racial groups: –African American –Hispanic American.>")












