Download presentation
Presentation is loading. Please wait.

2
Insulin therapy in Type 2 Diabetes: Current and Future Directions

3
When we started insulin?
Type 1 Sometimes Type 2

4
Pharmacologic Therapy for Type 2 Diabetes
Sulfonylureas (glyburide, glipizide, glimepiride) Biguanides (metformin) Alpha-glucosidase inhibitors (acarbose, miglitol, voglibose) Benzoic acid analogues (repaglinide) Thiazolidinediones (troglitazone, rosiglitazone, pioglitazone) Insulin (human insulin, insulin analogues)
 Biguanides (metformin) Alpha-glucosidase inhibitors (acarbose, miglitol, voglibose) Benzoic acid analogues (repaglinide) Thiazolidinediones (troglitazone, rosiglitazone, pioglitazone) Insulin (human insulin, insulin analogues)")
5
Treatment Algorithm Nonpharmacologic therapy Monotherapy
Very symptomatic Severe hyperglycemia Ketosis Latent autoimmune diabetes Pregnancy Monotherapy Sulfonylureas/Benzoic acid analogue Biguanide Alpha-glucosidase inhibitors Thiazolidinediones Insulin Combination therapy Insulin

6
All patients with type 1 diabetes need insulin treatment permanently, unless they receive an islet or whole organ pancreas transplant; many patients with type 2 diabetes will require insulin as their beta cell function declines over time.

7
Indications for insulin therapy
unexplained recent weight loss (irrespective of the initial weight), a short history with severe symptoms, the presence of moderate to heavy ketonuria. pregnancy
, a short history with severe symptoms, the presence of moderate to heavy ketonuria. pregnancy.")
8
Type 2 DM Patient with persistent elevated FPG leves ( mg/dl) or ketonuria or ketonemia FPG more than 300 mg/dl with polyuria, polydipsia and weight loss Gestational diabetes Uncontrolled diabetes with oral agents Physician-patient option wish to receive insulin as initial therapy Wasting state Latent autoimmune diabetes in adult Post MI Renal failure Allergy or serious reaction to oral agents

9
Types of insulin

10
Types of insulin Insulin glargine :
No real advantage with regard to A1C Lower fasting blood glucose and fewer hypoglycemic episodes Do not mix with other insulin

11
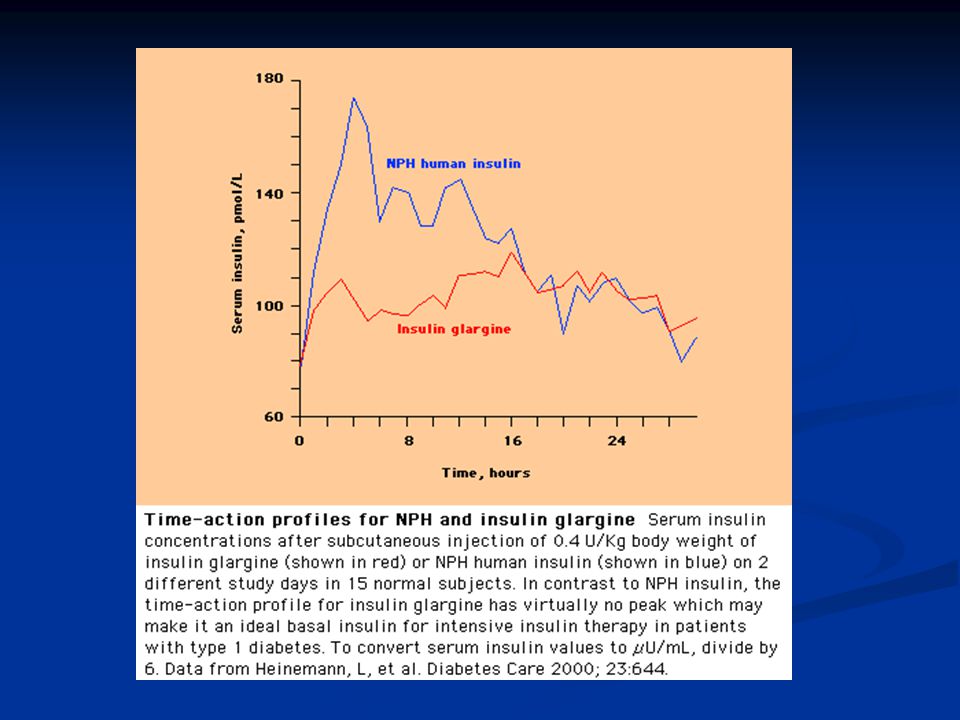
Glargine: A New Long-Acting Insulin Analogue
Modifications to human insulin chain Substitution of glycine at position A21 Addition of two arginines at position B30 Unique release pattern from injection site

12
Characteristics of Insulin Glargine
Euglycemic clamp studies vs. NPH Smooth continuous release from injection site Longer duration of action Continued effect at end of 24-hour clamp study No differences in the absorption rate from arm, leg, or abdominal sites No inflammatory reactions at any of the injection sites Flat insulin profile As effective in lowering FPG levels as NPH insulin, with significantly reduced nocturnal hypoglycemia

15
Insulin detemir Its duration of action appears to be substantially shorter than that of insulin glargine, Compare to NPH insulin detemir may be associated with slightly less nocturnal hypoglycemia and weight gain

16
Very-rapid-acting insulin
lispro, aspart glulisine Onset of action within 5 to15 Peak action at 30 to 90 Duration of action of two to four hours.

17
Clinical Efficacy of Insulin Lispro
Worldwide clinical trials of insulin lispro in >10,000 patients with type 1 or type 2 diabetes Dosage regimen: insulin lispro 10 min before and soluble human insulin 30 to 45 minutes before meals, with NPH or ultralente insulin as the basal insulin supplement

18
Advantages of very rapid acting to regular
decreases the postprandial rise in blood glucose reduce the frequency of hypoglycemia It is more convenient because it can be injected immediately before meals No difference in A1C Need to increase in the dose of NPH when a patient is switched from regular insulin to a very-rapid-acting insulin

19
The teratogenicity and long term safety profile of rapid-acting insulins in pregnancy are unknown, although many diabetologists do prescribe very-rapid-acting insulins during pregnancy.

20
CHOICE OF INSULIN REGIMEN
The basic requirements are : Baseline dose of insulin (whether an intermediate or long-acting insulin or given via CSII) plus Adjustable doses of pre-meal rapid-acting insulin (regular) or very-rapid-acting insulin analogs (lispro, aspart, or glulisine).
 plus. Adjustable doses of pre-meal rapid-acting insulin (regular) or very-rapid-acting insulin analogs (lispro, aspart, or glulisine).")
21
Method of Insulin Preparation
Conventional insulin therapy Intensive insulin therapy: MSI CSII

25
Getting started Start on a total daily dose of 0.2 to 0.4 units of insulin per kg per day, although most will ultimately require 0.6 to 0.7 units per kg per day. One-half of the total dose as a basal insulin (2/3 in the morning 1/3 in the bed time The remainder is given as rapid or very rapid-acting insulin, divided before meals. The pre-meal dosing is determined by the usual meal size and content, as well as activity and exercise pattern.

26
Conventional insulin therapy

27
Methods of MSI

28
Major drawback to intensive therapy
Cost (three times ) Weight gain Risk of hypoglycemia (three times)
 Weight gain. Risk of hypoglycemia (three times)")
29
When to start intensive therapy
Intensive therapy should be started as early as possible following the diagnosis of type 1 diabetes.

30
Residual beta cell function
Intensive insulin therapy Residual beta cell function lower risk of hypoglycemia

31
MANAGEMENT ISSUES Consistency SMBG The content and timing of meals,
The site of insulin injections, The timing and frequency of exercise. SMBG Four to seven times daily

33
Insulin Pump CSII: uses portable infusion pump connected to an indwelling subcutaneous catheter to deliver short-acting insulin

34
MSI or CSII Same efficacy, Same frequency of hypoglycemic events,
Same impact on quality of life for most patients

35
MSI CSII For a patient who has been well controlled on his previous MSI (eg, A1C <7.0 percent), the initial total daily dose of insulin administered by pump may be 10 to 20 percent less than the total daily dose of the previous regimen. Conversely, patients with inadequate glycemic control may be started with the same total daily dose as they had been using with their injection regimens.
, the initial total daily dose of insulin administered by pump may be 10 to 20 percent less than the total daily dose of the previous regimen. Conversely, patients with inadequate glycemic control may be started with the same total daily dose as they had been using with their injection regimens.")
36
In general, approximately one-half of the total daily dose is administered as basal rate.
For most patients, basal rates are in the range of 0.01 to units per kg per hour (ie, for a 60 kg woman approximately 0.6 to 0.9 units per hour).
.")
37
Advantages of CSII instead of MSI
Slightly better glycemic control (lower A1C) The use of very-rapid-acting insulin instead of regular may result in a lower A1C, less hypoglycemia, and less weight gain More flexibility in the timing of meals Insulin absorption is less variable from day to day
 The use of very-rapid-acting insulin instead of regular may result in a lower A1C, less hypoglycemia, and less weight gain. More flexibility in the timing of meals. Insulin absorption is less variable from day to day.")
38
Disadvantages of CSII instead of MSI
Cost Infection at the site of needle insertion infusion-system failure DKA is more common

39
Insulin Pump

40
Insulin therapy in Type 2 Diabetes: Current and Future Directions

41
Pharmacologic Therapy for Type 2 Diabetes
Sulfonylureas (glyburide, glipizide, glimepiride) Biguanides (metformin) Alpha-glucosidase inhibitors (acarbose, miglitol, voglibose) Benzoic acid analogues (repaglinide) Thiazolidinediones (troglitazone, rosiglitazone, pioglitazone) Insulin (human insulin, insulin analogues)
 Biguanides (metformin) Alpha-glucosidase inhibitors (acarbose, miglitol, voglibose) Benzoic acid analogues (repaglinide) Thiazolidinediones (troglitazone, rosiglitazone, pioglitazone) Insulin (human insulin, insulin analogues)")
42
Treatment Algorithm Nonpharmacologic therapy Monotherapy
Very symptomatic Severe hyperglycemia Ketosis Latent autoimmune diabetes Pregnancy Monotherapy Sulfonylureas/Benzoic acid analogue Biguanide Alpha-glucosidase inhibitors Thiazolidinediones Insulin Combination therapy Insulin

43
UKPDS: Effect of Intensive Therapy on Glycemia
UKPDS Group. Lancet. 1998;352:

44
UKPDS 10-Year Cohort Data: Reductions With Intensive vs
UKPDS 10-Year Cohort Data: Reductions With Intensive vs. Conventional Therapy UKPDS Group. Lancet. 1998;352:

45
Summary of Key Findings
Kumamoto trial: Intensive insulin treatment reduced microvascular complications Established glycemic threshold to prevent onset and progression of complications UKPDS: Diet therapy alone inadequate in two thirds of patients Pharmacologic therapy plus nutrition/exercise necessary Weigh benefit:risk ratio No threshold for HbA1c reduction in reducing complications Insulin does not increase macrovascular disease

46
Strategies for Insulin Therapy in Elderly Patients
Insulin therapy often considered a last resort in the elderly Therapeutic goals: Relieve symptoms Prevent hypoglycemia Prevent acute complications of hyperglycemia Ways to facilitate insulin treatment: Simple dose schedules Premixed preparations Improved, more convenient delivery systems

47
Combination Therapy: Oral Agents Plus Insulin
Rationale Combination of two agents with different mechanisms of action More convenient and may be safer Sulfonylurea + Insulin BIDS therapy: bedtime insulin/daytime sulfonylurea Useful in patients early in course of disease Metformin + Insulin Improves insulin sensitivity Alpha glucosidase inhibitor (acarbose) + Insulin Decreases postprandial glycemia Thiazolidinediones + Insulin Improves insulin resistance, improves insulin action in peripheral tissues Reduces insulin requirement
 + Insulin. Decreases postprandial glycemia. Thiazolidinediones + Insulin. Improves insulin resistance, improves insulin action in peripheral tissues. Reduces insulin requirement.")
49
Meta-Analysis of Sulfonylurea/Insulin Combination Therapy
Johnson JL, et al. Arch Intern Med. 1996;156:

50
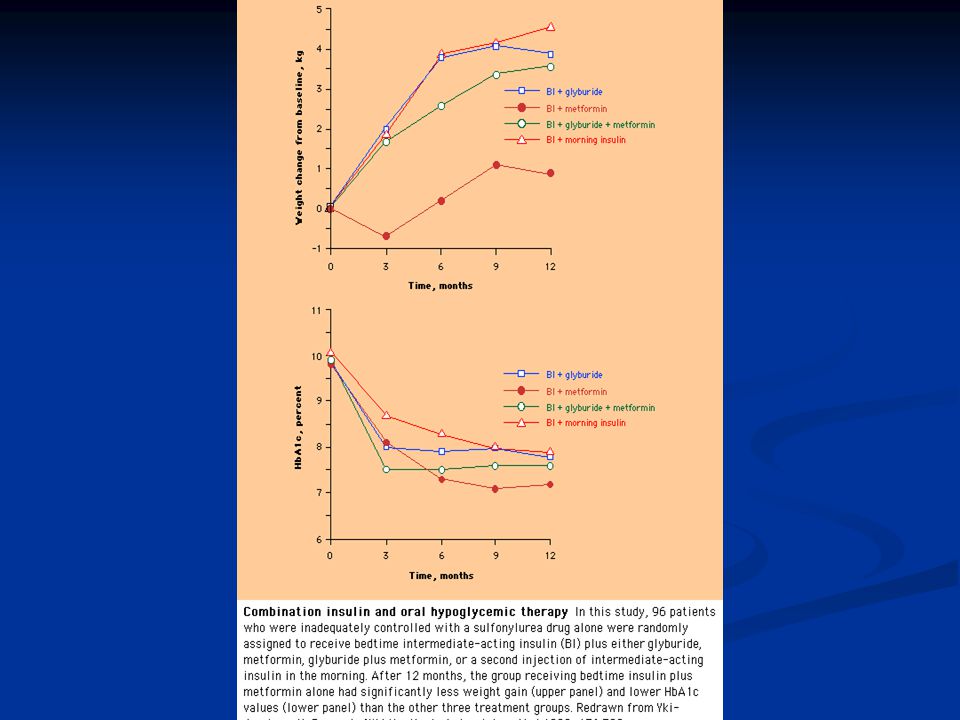
Comparison of Insulin Regimens Among Oral Treatment Failures
Yki-Jarvinen H, et al. N Engl J Med. 1992;327:

51
Need for Novel Delivery Systems of Insulin
Disadvantages of conventional subcutaneous injection: Discomfort Inconvenience Systemic delivery Inconsistent pharmacokinetics Irreversible after injection Insulin pumps: too complex, limited experience and utility with type 2 Insulin pen: beneficial but underutilized Systems in clinical testing Inhaled formulation Jet-injected systems

52
Insulin Pen Benefits Advantages of newer insulin pens
More accurate dosing mechanisms Faster and easier than conventional syringes Improved patient attitude and compliance Advantages of newer insulin pens LCD display to show dosage setting Dosage settings change quickly and easily Safety button automatically resets after drug delivery

53
Insulin Pen

54
Inhaled Insulin Formulations
Gelfand RA, et al. Presented at ADA 58th Annual Meeting. 1998:Abstract 0235.

55
Continuous Glucose Sensors
When available, may provide only mechanical means of achieving “normal” glucose homeostasis Will direct insulin delivery automatically on demand (“closed loop”) One technology uses reverse iontophoresis to noninvasively extract and measure glucose levels Technical challenge to develop
 One technology uses reverse iontophoresis to noninvasively extract and measure glucose levels. Technical challenge to develop.")
56
Conclusions Type 2 diabetes: gradual deterioration of glycemic control
Significant morbidity and mortality; tight glycemic control reduces risk of complications Earlier institution of insulin may help attain initial glycemic control Objectives of insulin therapy: Achieve normal fasting glucose levels Achieve normal postprandial glucose levels Minimize hypoglycemia Intensive insulin therapy should: Provide good glycemic control Produce little hypoglycemia Improve lipid profile Reduce risks and costs of treating complications

57
Conclusions (cont’d) New delivery systems:
Reduce limitations of conventional insulin syringes Improve patient compliance and disease management New long-acting insulin analogues (eg, insulin glargine): Produce flat insulin profile with no peaks Allow once-daily administration Significantly reduce nocturnal hypoglycemia
: Produce flat insulin profile with no peaks. Allow once-daily administration. Significantly reduce nocturnal hypoglycemia.")
59
Type of insulin available
Regular insulin Insulin analogues, Lispro, Glargine Alternate delivery system pump , pulmonary, intranasal , ocular, rectal , transdermal Combination with oral agents Initiating insulin in patient on oral agents bedtime insulin

60
What regimens are best for type 1?
Newly diagnosed patients or latent autoimmune DM may do well receiving once or twice basal insulin Physiological regimens or both prandial and basal insulin is required in severe insulin deficiency

61
Practical strategy to start insulin in type 2 DM
Continue oral agents at the same dose (eventually reduce) Add single evening dose(5 -10 IU) for thin and (10-15 IU) for obese patients Adjust dose weekly 2-4 IU
 Add single evening dose(5 -10 IU) for thin and (10-15 IU) for obese patients. Adjust dose weekly 2-4 IU.")
62
How dose the patient use supplement and adjustment ?
A conservative dose for type 1 is additional 1 IU per 50 mg /dl above the target For type 2 DM 1IU per 30 mg/dl above the target If patients are to inject supplements less than 3 hours after previous insulin they can decrease it 50%

63
Meal bolus insulin Exercise
* The dose should be decrease by 30% for postprandial exercise of less than one hour, 40 % for 1-2 hours, 50 % for more than two hours Food * Insulin requirement approximately 1 unit of insulin per 15 g carbohydrate

64
Experience Each patient must educated for insulin and blood glucose and record data Blood glucose and insulin logs should be reviewed weekly until goal

65
Discontinuation of insulin in T2DM
Reduce the dose by 10 to 15% of total dose If the blood glucose rise, restore the initial dose If the blood glucose dose not rise reduce 10 %- 15% every 1-2 weeks When daily dose reached to u/kg consider discontinuing insulin

66
Benefits of combination therapy?
Reduces fasting and postprandial glucose Directly suppresses hepatic glucose production Reduce free fatty acid levels Counteracts dawn phenomenon Minimal education needed Easily started on an outpatient state Better compliance Less total exogenous insulin needed

Similar presentations














. Who needs screening for DM? Age >45 Obese – BMI >25 1 st degree relative with DM Racial groups: –African American –Hispanic American.>")










>")

