Download presentation
Presentation is loading. Please wait.

2
www.washingtonhra.com

3
3 million Americans 160,000 new cases each year 16 million by 2050 90% of patients have recurrences Incremental cost = $26 billion JACC 2004; 43(1): 47-52. Circ 2006; 114: 119-125. Circ Cardiovasc Qual Outcomes 2011; 4(3): 313-20.
:")
4
RATE CONTROL RHYTHM CONTROL STROKE PREVENTION

5
An 84 year old woman with HTN presents for routine follow-up of long-standing atrial fibrillation. She is active and asymptomatic. She is on Toprol 100 mg daily and warfarin. Her resting HR is irregular and 97, blood pressure 110/68. Her exam is otherwise normal. What should you do next? A. Continue current therapy. B. Increase her Toprol to 150 mg daily. C. Start dronedarone 400 mg bid. D. Add digoxin 0.125 mg daily. E. Refer for DCCV.

6
An 84 year old woman with HTN presents for routine follow-up of long-standing atrial fibrillation. She is active and asymptomatic. She is on Toprol 100 mg daily and warfarin. Her resting HR is irregular and 97, blood pressure 110/68. Her exam is otherwise normal. What should you do next? A. Continue current therapy. B. Increase her Toprol to 150 mg daily. C. Start dronedarone 400 mg bid. D. Add digoxin 0.125 mg daily. E. Refer for DCCV.

7
Rest heart rate ≤ 80 bpm. 24-hr Holter average ≤ 100 bpm. 6-min walk HR ≤ 110 bpm. NEJM. 347(23): 2002.
:")
8
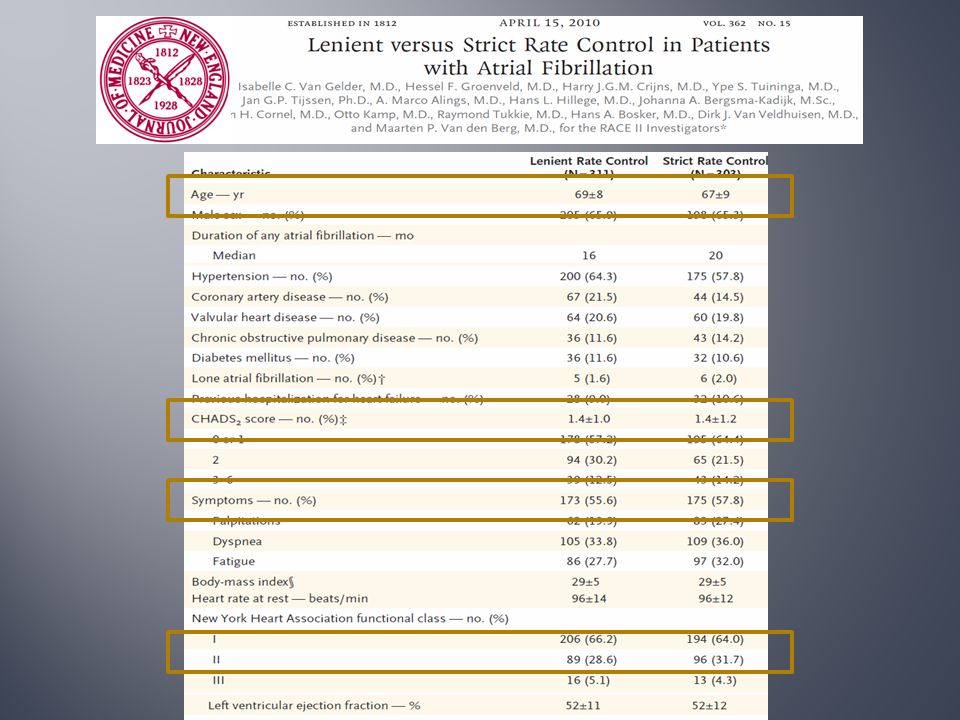
614 patients with permanent atrial fibrillation Strict vs. lenient rate control: < 80 bpm vs. < 110 bpm Noninferiority trial 1˚ EP: death from cardiovascular causes, hospitalization from CHF, CVA, systemic embolization, bleeding and life threatening arrhythmic events Follow-up: 2-3 years

10
Dyspnea, fatigue or palpitations 45.6% vs. 46.0%Avg HR: 94±9 vs. 76±12

11
Paroxysmal <7 days Persistent >7 days Permanent >12 months

12
A 52 year old man with atrial fibrillation and mild LV systolic dysfunction presents with recurrent atrial fibrillation and heart failure despite multiple attempts at DCCV followed by trials of dofetilide and amiodarone. Vitals: HR 68, BP 120/80. What should you do next? A. Titrate heart failure medications, nothing further can be done for the atrial fibrillation. B. Refer for AV node ablation and pacemaker placement. C. Start dronedarone 400 mg bid. D. Cardiovert and refer for catheter ablation (pulmonary vein isolation).
..")
13
A 52 year old man with atrial fibrillation and mild LV systolic dysfunction presents with recurrent atrial fibrillation and heart failure despite multiple attempts at DCCV followed by trials of dofetilide and amiodarone. Vitals: HR 68, BP 120/80. What should you do next? A. Titrate heart failure medications, nothing further can be done for the atrial fibrillation. B. Refer for AV node ablation and pacemaker placement. C. Start dronedarone 400 mg bid. D. Cardiovert and refer for catheter ablation (pulmonary vein isolation).
..")
14
A 52 year old man with atrial fibrillation and mild LV systolic dysfunction presents with recurrent atrial fibrillation and heart failure despite multiple attempts at DCCV followed by trials of dofetilide and amiodarone. Vitals: HR 68, BP 120/80. What should you do next? A. Titrate heart failure medications, nothing further can be done for the atrial fibrillation. B. Refer for AV node ablation and pacemaker placement. C. Start dronedarone 400 mg bid. D. Cardiovert and refer for catheter ablation (pulmonary vein isolation).
..")
18
1˚ EP ( recurrence or premature study drug discontinuation) : 74% vs 55% Atrial fibrillation recurrence 63.5% vs. 42% Premature discontinuation 10.4% vs. 13.3% J Cardiovasc Electrophysiol 2010; 21: 597-605.

19
DAFNE: to determine the most appropriate loading dose for prevention of AF after DCCV Freedom from Atrial Fibrillation

20
Resting HRExertional HR

21
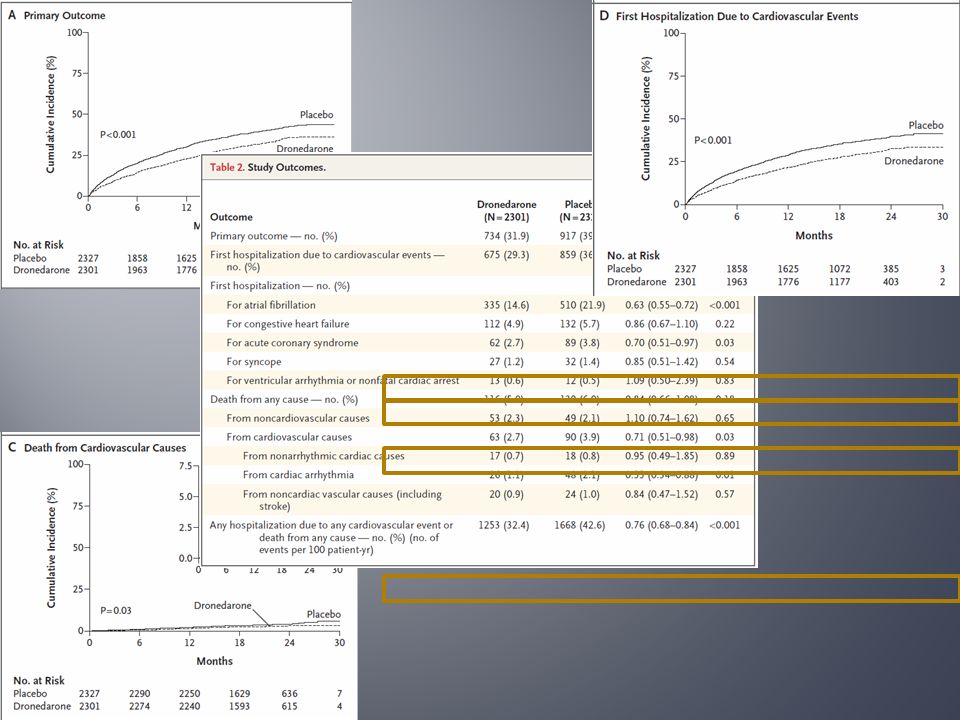
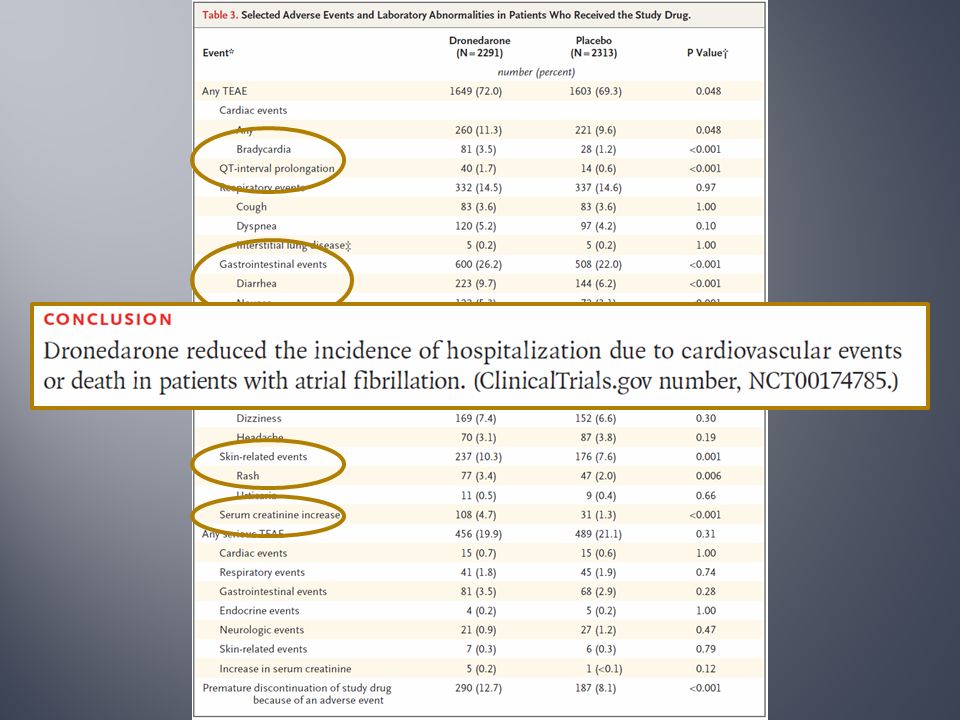
4628 patients: dronedarone 400 mg bid vs placebo 1˚ EP: 1 st hospitalization due to CV events or death Mean f/u 21 months Rx discontinuation: 30.2% vs 30.8% > 70 years old hypertension diabetes mellitus prior TIA/CVA/embolization LA diameter ≥50 mm LVEF ≤ 40%

26
Multi-national, RDBPC trial comparing placebo to dronedarone in patients with permanent atrial fibrillation Inclusion criteria: > 65 years old with history of embolization, myocardial infarction, ASCAD, prior CHF or >75 years old/HTN/DM. Exclusion criteria: class IV or unstable class III CHF Composite endpoint: MACE (stroke, systemic arterial embolization, MI, cardiovascular death), cardiovascular hospitalization and all-cause mortality
, cardiovascular hospitalization and all-cause mortality.")
27
Target enrollment: 10,800 patients Stopped at 3149 patients significant increase in cardiovascular events in patients taking dronedarone (Permanent Atrial fibriLLAtion outcome Study using dronedarone)
")
28
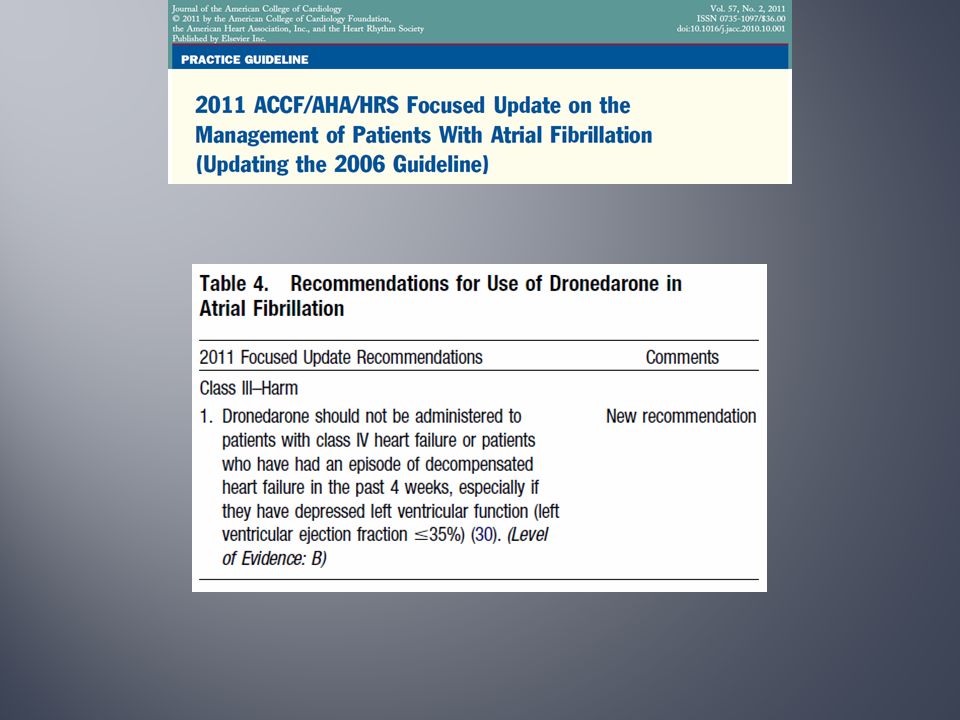
Hypothesis: Dronedarone will reduce the rate of hospitalization due to heart failure and possibly also reduce mortality by reducing arrhythmia. Inclusion Criteria: Class III-IV CHF or PND with LVEF ≤ 35% Exclusion Criteria: Acute pulmonary edema <12 hours prior Recent myocardial infarction Planned or recent cardiac surgery or angioplasty

29
Planned enrollment: 1000 patients Terminated after a median follow-up of 2 months HR 2.13; 95% CI: 1.07 to 4.25, p =0.03

31
A 52 year old man with atrial fibrillation and mild LV systolic dysfunction presents with recurrent atrial fibrillation and heart failure despite multiple attempts at DCCV followed by trials of dofetilide and amiodarone. Vitals: HR 68, BP 120/80. What should you do next? A. Titrate heart failure medications, nothing further can be done for the atrial fibrillation. B. Refer for AV node ablation and pacemaker placement. C. Start dronedarone 400 mg bid. D. Cardiovert and refer for catheter ablation (pulmonary vein isolation).
..")
32
A 52 year old man with atrial fibrillation and mild LV systolic dysfunction presents with recurrent atrial fibrillation and heart failure despite multiple attempts at DCCV followed by trials of dofetilide and amiodarone. Vitals: HR 68, BP 120/80. What should you do next? A. Titrate heart failure medications, nothing further can be done for the atrial fibrillation. B. Refer for AV node ablation and pacemaker placement. C. Start dronedarone 400 mg bid. D. Cardiovert and refer for catheter ablation (pulmonary vein isolation).
..")
33
…... www.atrialfibrillationablation.org

35
www.aafp.org

36
Multicenter, prospective, randomized, open-label clinical trial Hypothesis: Percutaneous LACA for the purpose of eliminating atrial fibrillation is superior to current state- of-the-art therapy with either rate control or rhythm control drugs. Inclusion criteria: paroxysmal or persistent atrial fibrillation with stroke/TIA or one or more risk factors 1˚ Endpoint: total mortality Follow-up: minimum of 2 years

37
A 76 year old male with HTN and diabetes presents with the new diagnosis of atrial fibrillation, discovered on a preoperative EKG for cataract surgery. He is active and asymptomatic. Medications include Toprol and Metformin. His resting heart rate is well controlled. What do you advise to decrease his risk for stroke? A. No additional treatment is necessary. B. Start ASA 325 mg daily. C. Start ASA 81 mg daily and Plavix 75 mg daily. D. Begin warfarin. E. Jantoven, dabigatran or rivaroxaban should be started.

38
www.med.umich.edu otm.oxfordmedicine.com

39
A 76 year old male with HTN and diabetes presents with the new diagnosis of atrial fibrillation, discovered on a preoperative EKG for cataract surgery. He is active and asymptomatic. Medications include Toprol and Metformin. His resting heart rate is well controlled. What do you advise to decrease his risk for stroke? A. No additional treatment is necessary. B. Start ASA 325 mg daily. C. Start ASA 81 mg daily and Plavix 75 mg daily. D. Begin warfarin. E. Jantoven, dabigatran or rivaroxaban should be started.

40
Low risk = ASAHigh Risk = AC

41
*Vascular disease = prior MI, aortic plaque or peripheral vascular disease * Anticoagulation for scores ≥ 2

43
1° Endpoint: stroke, systemic embolization, myocardial infarction or vascular death

45
Hypothesis: The addition of clopidogrel to ASA will reduce the risk of vascular events. 1° Endpoint: stroke, systemic embolization, myocardial infarction or vascular death

46
7,554 patients, median follow-up 3.6 years 1° Endpoint: stroke, systemic embolization, myocardial infarction or vascular death

49
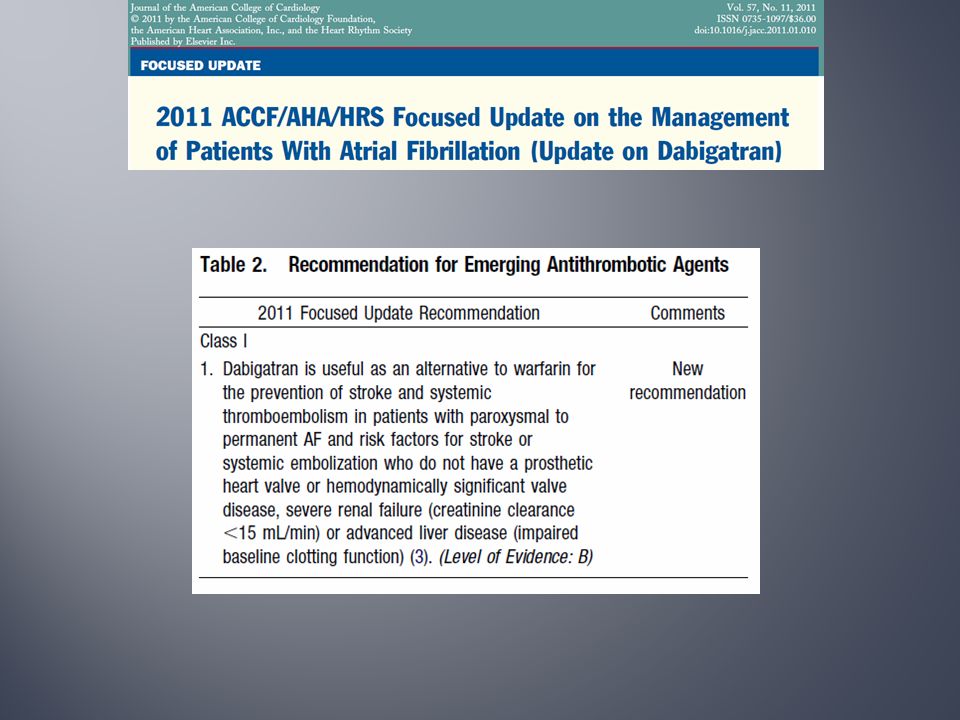
FDA NEWS RELEASE : 19 OCT 2010 FDA approves Pradaxa to prevent stroke in patients with ATRIAL FIBRILLATION

51
A 76 year old male with HTN and diabetes presents with the new diagnosis of atrial fibrillation, discovered on a preoperative EKG for cataract surgery. He is active and asymptomatic. Medications include Toprol and Metformin. His resting heart rate is well controlled. What do you advise to decrease his risk for stroke? A. No additional treatment is necessary. B. Start ASA 325 mg daily. C. Start ASA 81 mg daily and Plavix 75 mg daily. D. Begin warfarin. E. Jantoven, dabigatran or rivaroxaban should be started.

52
A 76 year old male with HTN and diabetes presents with the new diagnosis of atrial fibrillation, discovered on a preoperative EKG for cataract surgery. He is active and asymptomatic. Medications include Toprol and Metformin. His resting heart rate is well controlled. What do you advise to decrease his risk for stroke? A. No additional treatment is necessary. B. Start ASA 325 mg daily. C. Start ASA 81 mg daily and Plavix 75 mg daily. D. Begin warfarin. E. Jantoven, dabigatran or rivaroxaban should be started.

53
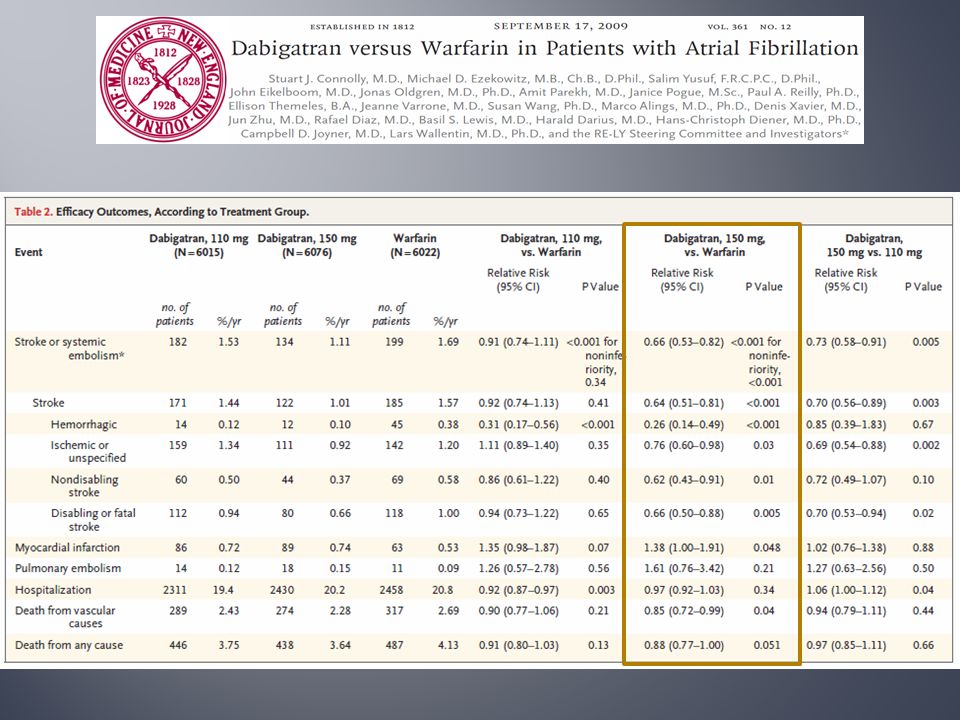
18,113 patients randomized to twice daily dabigatran (110,150 mg) or warfarin. Inclusion: over 75 years old and ≥1: Prior CVA or TIA EF <40%, h/o NYHA class II 65-74 years old with DM, HTN or ASCAD 1 ⁰ Endpoint: stroke or systemic embolization Median follow-up = 2 years

59
History of heart valve disorder Need for anticoagulant treatment of disorders other than atrial fibrillation Stroke in the previous 6 months Severe renal impairment (CrCl <30 cc/min) Reversible causes of atrial fibrillation (cardiac surgery, untreated hyperthyroidism) Plan to perform pulmonary vein isolation
 Reversible causes of atrial fibrillation (cardiac surgery, untreated hyperthyroidism) Plan to perform pulmonary vein isolation")
60
Increased bleeding risk: -major surgery 3 months -history of intracranial, intraocular, spinal or retroperitoneal or atraumatic intra-articular bleeds -gastrointestinal hemorrhage <1 year; PUD < 1 month -hemorrhagic disorder -uncontrolled hypertension -malignancy or radiation therapy < 6 months; survival < 3 years

61
Anemia (Hgb <10) or thrombocytopenia (<100) Active endocarditis Active liver disease Pregnancy or not taking contraception
 or thrombocytopenia (<100) Active endocarditis Active liver disease Pregnancy or not taking contraception")
62
For patients with CrCl >30 mL/min: 150 mg orally, twice daily. For patients with CrCl 15-30 mL/min: 75 mg orally, twice daily. Missed doses should be skipped if it cannot be taken at least 6 hours before the next scheduled dose.

63
From warfarin: When converting patients from warfarin therapy to PRADAXA, discontinue warfarin and start PRADAXA when the international normalized ratio (INR) is below 2.0 From Parenteral Therapy: start 0 to 2 hours before the time that the next dose of the parenteral drug was to have been administered
 is below 2.0 From Parenteral Therapy: start 0 to 2 hours before the time that the next dose of the parenteral drug was to have been administered")
64
Before initiating treatment with a parenteral anticoagulant: Wait 12 hours for CrCl ≥30 mL/min Wait 24 hours for CrCl <30 mL/min.

65
For CrCl >50 mL/min, start warfarin 3 days before discontinuing PRADAXA. For CrCl 31-50 mL/min, start warfarin 2 days before discontinuing PRADAXA. For CrCl 15-30 mL/min, start warfarin 1 day before discontinuing PRADAXA.

66
Discontinue PRADAXA 1 to 2 days (CrCl ≥50 mL/min) or 3 to 5 days (CrCl <50 mL/min) before invasive or surgical procedures. Consider longer times for patients undergoing major surgery, spinal puncture, or placement of a spinal or epidural catheter.

67
Most common adverse reactions (>15%) are gastritis-like symptoms and bleeding. P-gp inducers and inhibitors: avoid coadministration of rifampin.

68
Offering PRADAXA to all eligible new atrial fibrillation consultations Prescribing PRADAXA to appropriate existing atrial fibrillation patients who request it Screening existing atrial fibrillation patients and providing educational materials

69
limelightprsonar.files.wordpress.com

71
Wafarin Dabigatran Rivaroxaban Apixaban X X X XX

72
DabigatranRivaroxabanApixaban Pharmacology12-17 hrs (bid)7-11 hrs (daily)12 hrs (bid) CHADS2 Prior TIA/CVA Primary Outcome Bleeding Death Notes
7-11 hrs (daily)12 hrs (bid) CHADS2 Prior TIA/CVA Primary Outcome Bleeding Death Notes")
73
DabigatranRivaroxabanApixaban Pharmacology12-17 hrs (bid)7-11 hrs (daily)12 hrs (bid) CHADS22.13.52.1 Prior TIA/CVA20%55%19% Primary Outcome Bleeding Death Notes
7-11 hrs (daily)12 hrs (bid) CHADS Prior TIA/CVA20%55%19% Primary Outcome Bleeding Death Notes")
74
DabigatranRivaroxabanApixaban Pharmacology12-17 hrs (bid)7-11 hrs (daily)12 hrs (bid) CHADS22.13.52.1 Prior TIA/CVA20%55%19% Primary OutcomeSuperior (1.53%)Noninferior/ Superior? (1.7-2.1%) Superior (1.27%) Bleeding Death Notes
 Superior (1.27%) Bleeding Death Notes.")
75
DabigatranRivaroxabanApixaban Pharmacology12-17 hrs (bid)7-11 hrs (daily)12 hrs (bid) CHADS22.13.52.1 Prior TIA/CVA20%55%19% Primary OutcomeSuperior (1.53%)Noninferior/ Superior? (1.7-2.1%) Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) Death Notes
 Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) Death Notes.")
76
DabigatranRivaroxabanApixaban Pharmacology12-17 hrs (bid)7-11 hrs (daily)12 hrs (bid) CHADS22.13.52.1 Prior TIA/CVA20%55%19% Primary OutcomeSuperior (1.53%)Noninferior/ Superior? (1.7-2.1%) Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) DeathNoninferior (p=0.051) NoninferiorSuperior Notes
 Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) DeathNoninferior (p=0.051) NoninferiorSuperior Notes.")
77
DabigatranRivaroxabanApixaban Pharmacology12-17 hrs (bid)7-11 hrs (daily)12 hrs (bid) CHADS22.13.52.1 Prior TIA/CVA20%55%19% Primary OutcomeSuperior (1.53%)Noninferior/ Superior? (1.7-2.1%) Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) DeathNoninferior (p=0.051) NoninferiorSuperior NotesGIB? MI?ACS, DVTNot FDA Approved
 Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) DeathNoninferior (p=0.051) NoninferiorSuperior NotesGIB. MI ACS, DVTNot FDA Approved.")
78
DabigatranRivaroxabanApixaban Pharmacology12-17 hrs (bid)7-11 hrs (daily)12 hrs (bid) CHADS22.13.52.1 Prior TIA/CVA20%55%19% Primary OutcomeSuperior (1.53%)Noninferior/ Superior? (1.7-2.1%) Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) DeathNoninferior (p=0.051) NoninferiorSuperior NotesGIB? MI?ACS, DVTNot FDA Approved
 Superior (1.27%) BleedingNoninferior (3.11%)Noninferior (3.6%)Superior (2.1%) DeathNoninferior (p=0.051) NoninferiorSuperior NotesGIB. MI ACS, DVTNot FDA Approved.")
79
I’m not dead yet! Bring out your dead- 45% of patients with atrial fibrillation appropriately anticoagulated. Broad indications for use. Safety with renal dysfunction. $$$$$$$

80
Strict rate control is not necessary in well compensated atrial fibrillation (III). Dronedarone is an option to decrease cardiovascular hospitalizations in patients with paroxysmal atrial fibrillation (IIa). Not with class IV CHF or recent decompensation (III). Evidence is mounting for catheter ablation (I). Dual anti-platelet therapy is an option in patients unsuitable to safely sustain AC or due to patient preference (IIb). Oral alternatives to warfarin are available (I).
. Not with class IV CHF or recent decompensation (III). Evidence is mounting for catheter ablation (I). Dual anti-platelet therapy is an option in patients unsuitable to safely sustain AC or due to patient preference (IIb). Oral alternatives to warfarin are available (I)..")
Similar presentations


















>")
















