Download presentation
Presentation is loading. Please wait.

1
ICD FOR PRIMARY PREVENTION EVIDENCE REVIEW
VINOD G V

2
MADIT I (The Multicenter Automatic Defibrillator Implantation Trial)
196 patients In NYHA I, II, or III with prior myocardial infarction Left ventricular ejection fraction < 0.35 Documented episode of asymptomatic unsustained ventricular tachycardia Inducible, nonsuppressible ventricular tachyarrhythmia on electrophysiologic study Randomly assigned to receive an implanted defibrillator (n=95) or conventional medical therapy (n=101)
 or conventional medical therapy (n=101)")
3
Exclusion criteria Previous cardiac arrest or ventricular tachycardia causing syncope that was not associated with an acute myocardial infarction Symptomatic hypotension while in a stable rhythm Myocardial infarction within the past three weeks Patients who had undergone CABG within the past two months or coronary angioplasty within the past three months

4
Primary endpoint: All cause Mortality
Two patient groups (1:1) 1. Conventional Medical Therapy (CMT) 2. CMT + ICD Mean follow up 27 months Primary endpoint: All cause Mortality From bsci.com – see reference section as well. Picture taken from bsci.com
 1. Conventional Medical Therapy (CMT) 2. CMT + ICD. Mean follow up 27 months. Primary endpoint: All cause Mortality. From bsci.com – see reference section as well. Picture taken from bsci.com.")
7
54% reduction in all cause mortality in ICD group (p o.oo9)
No evidence that amiodarone ,betablockers had any significant influence on mortality curves

8
MADIT II

9
Implantable defibrillator Conventional medical therapy
MADIT II: Study Design 1232 Patients with prior MI more than 30 days and LVEF < 30% randomized in a 3:2 ratio Implantable defibrillator (n=742) Conventional medical therapy (n=490) All Cause Mortality - Average follow-up of 20 months Stopped early
 Conventional medical therapy. (n=490) All Cause Mortality - Average follow-up of 20 months. Stopped early.")
10
MADIT II: All-Cause Mortality
Death Avg. follow-up=20 months P=0.016 Hazard Ratio = 0.65 Conventional Therapy ICD

11
MADIT II: Mortality Events
Non Cardiac Cardiac Arrhythmic Non Arrhythmic Conv Therapy ICD Conv Therapy Conv Therapy Conv Therapy ICD ICD ICD

12
New or Worsening Heart Failure
MADIT II: CHF New or Worsening Heart Failure P=0.09 Conventional Therapy ICD

13
CABG Patch trial — The Coronary Artery Bypass Graft (CABG) Patch trial
900 patients undergoing surgical revascularization for severe CAD significant LV dysfunction (LVEF <36 percent) A positive signal-averaged electrocardiogram Average follow-up of 32 months There were 101 deaths in the ICD group (71 of which were cardiac) and 95 in the control group (72 of which were cardiac). The hazard ratio was a difference that was not significant
 A positive signal-averaged electrocardiogram. Average follow-up of 32 months. There were 101 deaths in the ICD group (71 of which were cardiac) and 95 in the control group (72 of which were cardiac). The hazard ratio was 1.07 a difference that was not significant.")
15
Prophylactic therapy with the ICD did reduce arrhythmic death at 42 months by 45 percent
Since 71 percent of the deaths in this trial were nonarrhythmic, the reduction in arrhythmic death did not impact upon total mortality. ICD therapy was unable to improve mortality in this primary prevention trial because coronary revascularization itself has such a beneficial effect in the prevention of sudden death.

16
MUSTT(Multicentre UnSustained Tachycardia Trial)
Inclusion criteria Patients with coronary artery disease Left ventricular ejection fraction of 40 percent or less Asymptomatic, unsustained ventricular tachycardia. Patients in whom sustained ventricular tachyarrhythmias were induced by programmed stimulation

17
MUSTT 704 patients underwent randomization
351 were assigned to receive electrophysiologically guided therapy 353 were assigned to receive no antiarrhythmictherapy. Antiarrhythmic drug in 154 and an ICD in 161. The median follow-up was 39 months

18
Results The two-year (12 versus 18 percent) and five-year (25 versus 32 percent) rates for the primary endpoint were significantly lower for EPS guided therapy compared to no therapy. There was a nearly significant reduction in the secondary endpoint of total mortality at five years in the group receiving EPS guided therapy (42 versus 48 percent, p = 0.06). The reduction in the primary and secondary endpoints in the EPS guided group was largely attributable to ICD therapy At five years the primary endpoint occurred in 9 percent of those receiving an ICD compared with 37 percent of those receiving an antiarrhythmic drug, and the secondary endpoint occurred in 24 and 55 percent respectively. There was no difference in outcome between patients receiving no therapy and those treated with an antiarrhythmic drug
 and five-year (25 versus 32 percent) rates for the primary endpoint were significantly lower for EPS guided therapy compared to no therapy. There was a nearly significant reduction in the secondary endpoint of total mortality at five years in the group receiving EPS guided therapy (42 versus 48 percent, p = 0.06). The reduction in the primary and secondary endpoints in the EPS guided group was largely attributable to ICD therapy. At five years the primary endpoint occurred in 9 percent of those receiving an ICD compared with 37 percent of those receiving an antiarrhythmic drug, and the secondary endpoint occurred in 24 and 55 percent respectively. There was no difference in outcome between patients receiving no therapy and those treated with an antiarrhythmic drug.")
24
Conclusions Electrophysiologically guided antiarrhythmic therapy with implantable defibrillators but not with antiarrhythmic drugs reduces the risk of sudden death in high-risk patients with coronary disease.

25
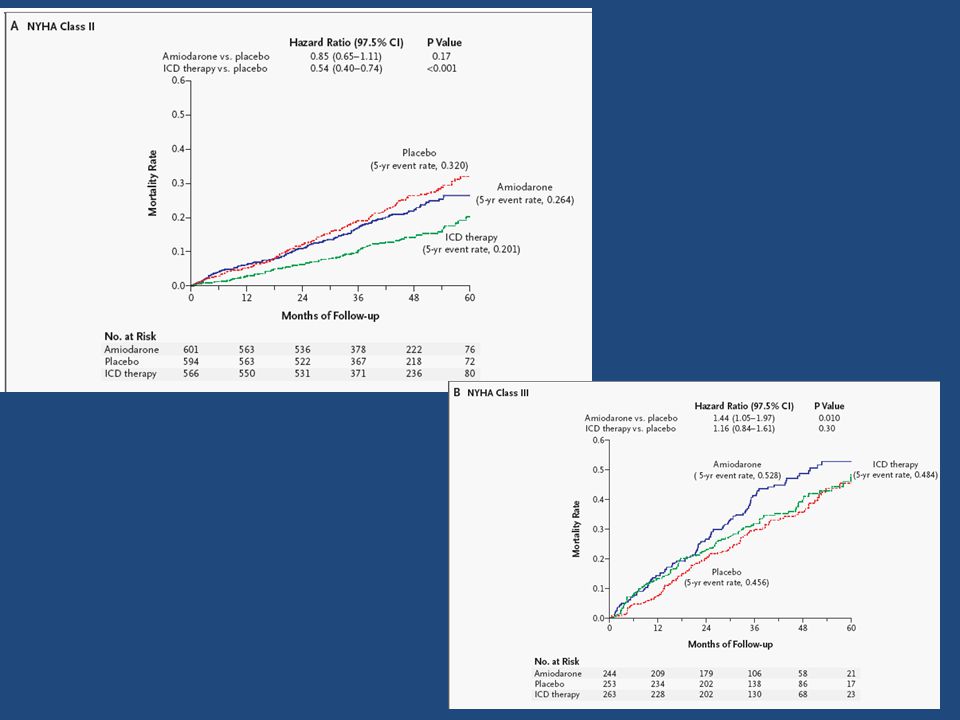
SCD-HeFT trial — The Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT)
Role of an ICD or amiodarone in patients with heart failure (HF) due to either an ischemic or nonischemic cardiomyopathy A total of 2521 patients LVEF ≤35 percent NYHA class II or III HF Randomly assigned to ICD implantation, amiodarone, or placebo. The etiology of cardiomyopathy was ischemic in 52 percent and nonischemic in 48 percent
 due to either an ischemic or nonischemic cardiomyopathy. A total of 2521 patients. LVEF ≤35 percent. NYHA class II or III HF. Randomly assigned to ICD implantation, amiodarone, or placebo. The etiology of cardiomyopathy was ischemic in 52 percent and nonischemic in 48 percent.")
26
Results Overall mortality at five years was significantly reduced with ICD therapy (29 versus 36 percent with placebo, HR 0.77, 95% CI ). The benefit of an ICD was comparable among patients with either an ischemic or nonischemic cardiomyopathy. Patients with NYHA class III HF did not appear to benefit from ICD therapy as there was a nonsignificant trend toward increased mortality in this group (HR 1.16 compared to 0.54 in NYHA class II HF). In a post hoc analysis, the benefit of an ICD was seen in patients with an LVEF ≤30 percent, but not in those with an LVEF >30 percent (HR 0.73 versus 1.08).
. In a post hoc analysis, the benefit of an ICD was seen in patients with an LVEF ≤30 percent, but not in those with an LVEF >30 percent (HR 0.73 versus 1.08).")
30
Conclusion An ICD is beneficial in patients with HF and a diminished LVEF (≤35 percent, or perhaps ≤30 percent). In contrast amiodarone was not beneficial in these patients.
. In contrast amiodarone was not beneficial in these patients.")
31
Early post MI trials DINAMIT IRIS

32
DINAMIT— The Defibrillator in Acute Myocardial Infarction Trial (DINAMIT)
Evaluated the role of prophylactic ICD implantation compared to no ICD Inclusion criteria 674 patients with MI in the preceding 6 to 40 days (mean 18 days) LVEF ≤35 percent Reduced heart rate variability or elevated resting heart rate (≥80beats/min). Exclusion criteria Patients with sustained VT >48 hours post-MI, NYHA class IV HF, or coronary artery bypass grafting (CABG) or three-vessel percutaneous coronary intervention post-MI Mean follow-up was 30 months.
 LVEF ≤35 percent. Reduced heart rate variability or elevated resting heart rate (≥80beats/min). Exclusion criteria. Patients with sustained VT >48 hours post-MI, NYHA class IV HF, or coronary artery bypass grafting (CABG) or three-vessel percutaneous coronary intervention post-MI. Mean follow-up was 30 months.")
33
Results There was no difference in annual all-cause mortality between the ICD patients and controls (7.5 versus 6.9 percent). Arrhythmic deaths were more frequent in the control arm, while nonarrhythmic deaths were more frequent in the ICD arm.

37
IRIS trial- Immediate Risk Stratification Improves Survival (IRIS)
Enrolled 898 patients . Inclusion criteria included an MI within the preceding 5 to 31 days and one or both of the following two criteria: LVEF ≤40 percent and a resting heart rate ≥90 beats/min Nonsustained VT at a rate of ≥150 beats/min Mean follow-up was 37 months

38
Results No difference in all-cause mortality between patients randomly assigned to ICD therapy and those assigned to medical therapy. The rate of SCD was higher in the control group The number of nonsudden cardiac deaths was higher in the ICD arm.

42
Significant recovery of ventricular function may have occurred in some of the patients which would dilute the long-term benefit of the ICD in such patients. Some SCD events in the early postinfarction period may have been due to recurrent ischemia which would not be definitively treated by ICD discharge ICD implantation might impose additional risk in these patients immediately post-MI. The enrollment requirements of reduced heart rate variability in DINAMIT and resting heart rate ≥90 beats/minin IRIS could have selected a group of patients with a high mortality from nonarrhythmic causes .

43
Patients with a nonischemic dilated cardiomyopathy LVEF ≤35 percent
DEFINITE trial — Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Patients with a nonischemic dilated cardiomyopathy LVEF ≤35 percent Ventricular premature beats or NSVT 458 patients were enrolled All received standard medical therapy including an ACE inhibitor (86 percent) and a beta blocker (85 percent). Patients were randomly assigned to an ICD or medical therapy alone
 Patients with a nonischemic dilated cardiomyopathy. LVEF ≤35 percent. Ventricular premature beats or NSVT. 458 patients were enrolled. All received standard medical therapy including an ACE inhibitor (86 percent) and a beta blocker (85 percent). Patients were randomly assigned to an ICD or medical therapy alone.")
44
There was a trend toward reduction in the primary endpoint of all-cause mortality in patients treated with an ICD (7.9 versus 14.1 percent with medical therapy alone, hazard ratio (HR) 0.65, 95% CI 0.40 to 1.06). Among the subset of patients with NYHA class III HF the difference was significant (HR 0.37, 95% CI 0.15 to 0.90). Fewer sudden deaths occurred in the ICD arm, although the number was very small (three deaths versus 14 deaths in the medical therapy arm, HR 0.20, 95% CI 0.06 to 0.71).
. Fewer sudden deaths occurred in the ICD arm, although the number was very small (three deaths versus 14 deaths in the medical therapy arm, HR 0.20, 95% CI 0.06 to 0.71).")
45
ICD combined with CRT

46
COMPANION trial — The Comparison Of Medical Therapy, Pacing, And Defibrillation In Heart Failure (COMPANION) trial 1520 patients NYHA class III-IV HF LVEF ≤35 percent who had had a hospitalization for HF within the year prior to enrollment Nearly half of all patients enrolled had a nonischemic etiology of HF. Randomly assigned to optimal medical therapy, CRT alone, or CRT with an ICD. Medical therapy for HF included ACEI OR ARB in 89 percent, beta blockers in 66 percent, and spironolactone in 55 percent.

47
Results At 12 months there was a significant reduction in the incidence of the combined endpoint of all-cause mortality and all-cause hospitalization in the two arms receiving CRT compared to the medical therapy only arm (56 versus 68 percent) . The CRT plus ICD arm, but not the CRT only arm, experienced a significant improvement in the secondary endpoint of all-cause mortality alone
 . The CRT plus ICD arm, but not the CRT only arm, experienced a significant improvement in the secondary endpoint of all-cause mortality alone.")
Similar presentations

























>")











