Download presentation
Presentation is loading. Please wait.

1
Atrial Fibrillation Warfarin and its newer alternatives
Dr Mark Abelson Cardiologist Somerset West

9
Association of AF and Stroke MM00453 (01) Intl 06/09
 Intl 06/09")
11
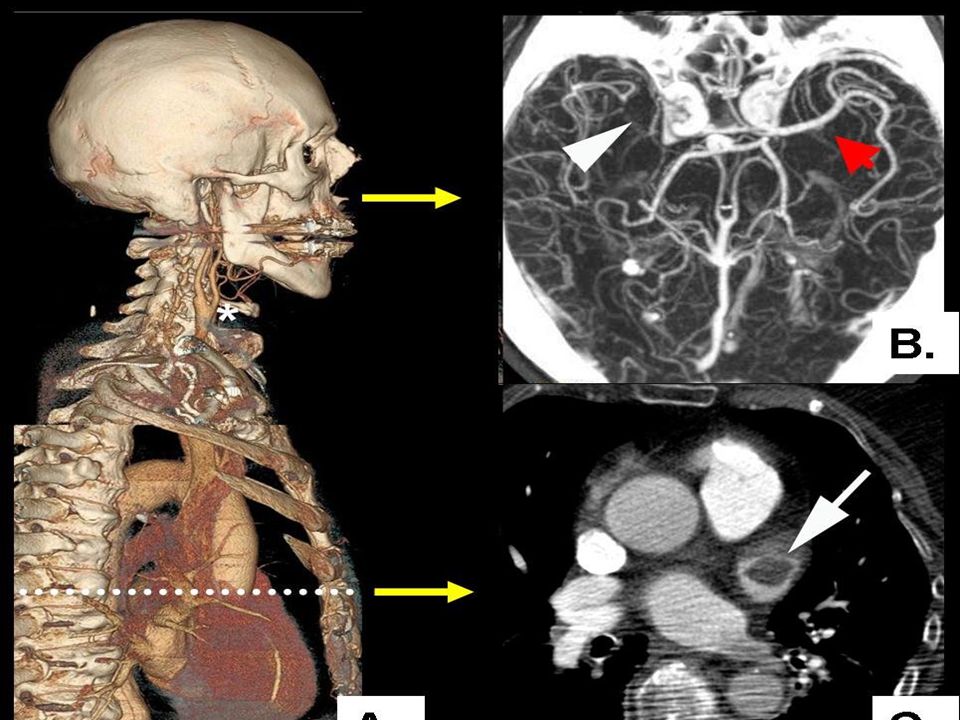
Occluded Left ICA-T Pre and Post Embolectomy
54y M, “Wake up” >4h,NIHSS=32 90 d

12
Carotid Embolectomy

13
AF and Stroke Atrial Fibrillation and Stroke
3 million in US and 4.5 million in the EU have AF 2/3 of AF population are at high-risk of stroke AF is responsible for 15-20% of ischemic strokes AF Incidence increases with age % in general population % of yrs of age % of >60 yrs of age -- 10% of > 80 yrs of age

14
Relationship of AF and Stroke

15
Annual Stroke Risk for Patients with AF
Risk Stratification and Annual Stroke Risk for Patients with AF Annual Stroke Risk for Patients with AF By CHADS(2) Score CHADS(2) Score CHADS Congestive heart failure +1 Hypertension Age 75> Diabetes Mellitus Stroke or History of Cerebral Ischemia +2 F GAGE et al., 2004; 110:
 Score. CHADS(2) Score. CHADS. Congestive heart failure. +1. Hypertension. Age 75> Diabetes Mellitus. Stroke or History of Cerebral Ischemia. +2. F GAGE et al., 2004; 110:")
16
The CHA2DS2-VASc score predicts clinical risk of stroke and thromboembolism in atrial fibrillation[1]. Congestive Heart Failure 1 Hypertension 1 Age ≥ 75 years 2 Age between 65 and 74 years 1 Stroke/TIA/TE 2 Vascular disease (previous MI, peripheral arterial disease or aortic plaque) 1 Diabetes mellitus 1 Female 1 Before bleeding risk evaluated score of 0 recommends no antithrombotic therapy and 2 or more antithrombotic therapy. A score of 1 recommends either antithrombotic or antiplatelet therapy.
![The CHA2DS2-VASc score predicts clinical risk of stroke and thromboembolism in atrial fibrillation[1].](http://slideplayer.com/slide/6099913/18/images/16/The+CHA2DS2-VASc+score+predicts+clinical+risk+of+stroke+and+thromboembolism+in+atrial+fibrillation%5B1%5D..jpg "Congestive Heart Failure 1. Hypertension 1. Age ≥ 75 years 2. Age between 65 and 74 years 1. Stroke/TIA/TE 2. Vascular disease (previous MI, peripheral arterial disease or aortic plaque) 1. Diabetes mellitus 1. Female 1. Before bleeding risk evaluated score of 0 recommends no antithrombotic therapy and 2 or more antithrombotic therapy. A score of 1 recommends either antithrombotic or antiplatelet therapy.")
17
Clot Prevention Currently Available Management Options
Medical Management: Anticoagulant Effective: 67% stoke risk reduction(1) Narrow therapeutic window for proper dose Contraindicated in 14-47% of patients at risk of stroke (2) Major complication: bleeding Surgical Excision (Appendectomy) Residual shunt: 10% (3) Inconsistent outcomes due to incomplete exclusion; Can create pouch with stagnant blood flow (4,5) High invasiveness Transcatheter Device Closure Minimally invasive nature Designed for percutaneous closure of the LAA in prevention of clot embolization that may form in the LAA Intended as an alternative to warfarin therapy for patients with non-valvular atrial fibrillation
 Narrow therapeutic window for proper dose. Contraindicated in 14-47% of patients at risk of stroke (2) Major complication: bleeding. Surgical Excision (Appendectomy) Residual shunt: 10% (3) Inconsistent outcomes due to incomplete exclusion; Can create pouch with stagnant blood flow (4,5) High invasiveness. Transcatheter Device Closure. Minimally invasive nature. Designed for percutaneous closure of the LAA in. prevention of clot embolization that may form in the. LAA. Intended as an alternative to warfarin therapy for. patients with non-valvular atrial fibrillation.")
18
Warfarin Therapeutic Window - INR of 2 to 3
A small window: difficult to achieve a well controlled therapeutic range

19
AF Patients On Warfarin
% Only 55% of AF patients with no contraindications have evidence of warfarin use in previous 3 months Other studies cite warfarin use in AF patients from 17-50% Elderly patients with increased absolute risk least likely to be taking warfarin Contraindications 30-40% Ann Int Med 131(12), 1999
,")
20
INR Control – Not Good Low INR <1.6 Therapeutic INR 2-3
Efficacy 4-fold Therapeutic INR 2-3 High INR >3.2 % Bungard: Pharmacotherapy 20:1060, 2001

21
New Warfarin Alternatives
NO INR monitoring - Dabigatran ( Pradaxa) – direct thrombin inhibitor - Rivaroxaban (Xarelto) – F10a inhibitor Aspirin plus clopidogrel Aspirin (reduces stroke risk by 20%)
 – direct thrombin inhibitor. - Rivaroxaban (Xarelto) – F10a inhibitor. Aspirin plus clopidogrel. Aspirin (reduces stroke risk by 20%)")
23
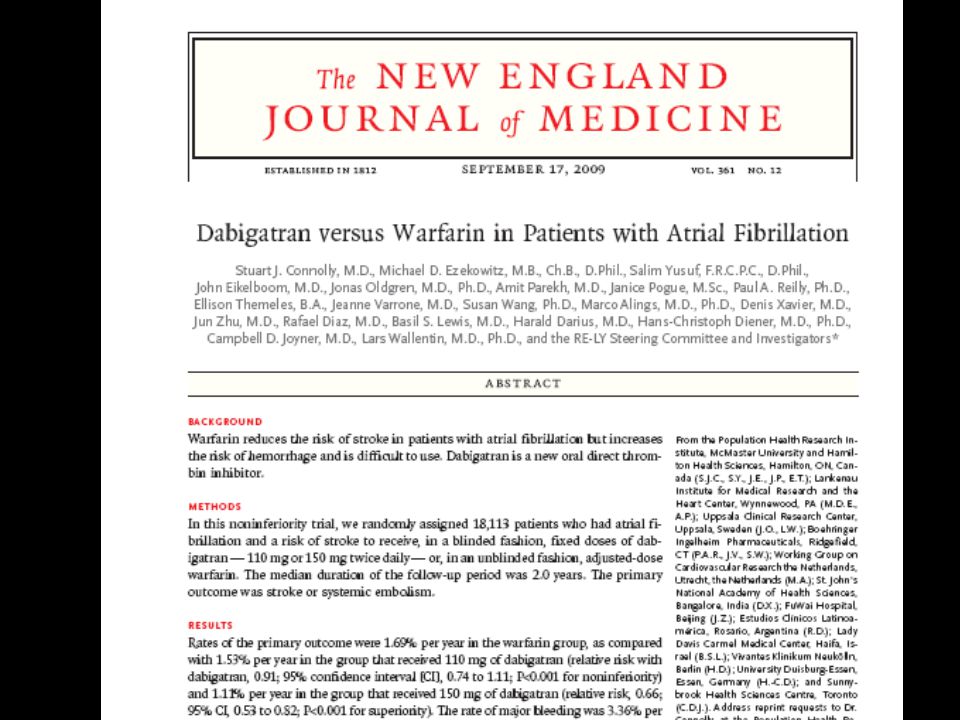
Rely Trial Background Warfarin reduces the risk of stroke in patients with atrial fibrillation but increases the risk of hemorrhage and is difficult to use. Dabigatran is a new oral direct thrombin inhibitor. Conclusions In patients with atrial fibrillation, dabigatran given at a dose of 110 mg was associated with rates of stroke and systemic embolism that were similar to those associated with warfarin, as well as lower rates of major hemorrhage. Dabigatran administered at a dose of 150 mg, as compared with warfarin, was associated with lower rates of stroke and systemic embolism but similar rates of major hemorrhage. (ClinicalTrials.gov number, NCT )
")
24
Risk of Stroke or Embolism
Figure 1. Cumulative Hazard Rates for the Primary Outcome of Stroke or Systemic Embolism, According to Treatment Group. Connolly SJ et al. N Engl J Med 2009;361:

25
Relative Risk of the Primary Outcome of Stroke or Systemic Embolism with Dabigatran versus Warfarin, According to Subgroup. Figure 2. Relative Risk of the Primary Outcome of Stroke or Systemic Embolism with Dabigatran versus Warfarin, According to Subgroup. Ethnic group was self-reported. Long-term therapy with a vitamin K antagonist (VKA) denotes a total lifetime use of a VKA of 61 days or more. The body-mass index is the weight in kilograms divided by the square of the height in meters. The CHADS2 score is a measure of the risk of stroke in which congestive heart failure, hypertension, an age of 75 years or older, and diabetes mellitus are each assigned 1 point and previous stroke or transient ischemic attack is assigned 2 points; the score is calculated by summing all the points for a given patient. 12 Creatinine clearance was calculated according to the Cockcroft–Gault method. The squares with horizontal lines are hazard ratios and corresponding 95% confidence intervals; the sizes of squares are proportional to the sizes of the subgroups. PPI denotes proton-pump inhibitor. Connolly SJ et al. N Engl J Med 2009;361:
 denotes a total lifetime use of a VKA of 61 days or more. The body-mass index is the weight in kilograms divided by the square of the height in meters. The CHADS2 score is a measure of the risk of stroke in which congestive heart failure, hypertension, an age of 75 years or older, and diabetes mellitus are each assigned 1 point and previous stroke or transient ischemic attack is assigned 2 points; the score is calculated by summing all the points for a given patient. 12 Creatinine clearance was calculated according to the Cockcroft–Gault method. The squares with horizontal lines are hazard ratios and corresponding 95% confidence intervals; the sizes of squares are proportional to the sizes of the subgroups. PPI denotes proton-pump inhibitor. Connolly SJ et al. N Engl J Med 2009;361:")
26
Rivaroxaban Xarelto® is the first oral, once-daily direct Factor Xa inhibitor for the prevention of venous thromboembolism in adult patients undergoing elective hip or knee replacement surgery Atrial Fibrillation

27
ROCKET AF TRIAL (Stroke Prevention Using the Oral Direct Factor Xa Inhibitor Rivaroxaban Compared With Warfarin in Patients with Nonvalvular Atrial Fibrillation) The trial showed that the experimental factor Xa inhibitor rivaroxaban was as effective as warfarin in preventing stroke in 14,264 AF patients and did not increase their risk of bleeding. In the per protocol analysis, the rate of stroke and embolism was lower in the rivaroxaban group than in the warfarin group (p<0.001 for non-inferiority, p=0.018 for superiority). Major bleeding complications occurred at a similar rate (p=0.576). Rate of stroke and embolism: Rivaroxaban: 1.71 events per 100 patient-years Warfarin: 2.16 events per 100 patient-years Major bleeding complications: Rivaroxaban: 3.60 events per 100 patient-years Warfarin: 3.45 events per 100 patient-years However, in the full intention-to-treat analysis, the superiority of rivaroxaban over warfarin did not achieve statistical significance (p=0.177). Intracerebral hemorrhage occurred in 55 patients on riveroxaban and 84 on warfarin (p=0.019). “The main implication is that we have an alternative to warfarin,” said Robert Califf, M.D., co-principal investigator of the study, in an AHA press release. “Equally important, there was no increase in bleeding, so we have a drug you can take once a day, without monitoring, that is at least as good as warfarin and carries no additional risk.”
. Major bleeding complications occurred at a similar rate (p=0.576). Rate of stroke and embolism: Rivaroxaban: 1.71 events per 100 patient-years. Warfarin: 2.16 events per 100 patient-years. Major bleeding complications: Rivaroxaban: 3.60 events per 100 patient-years. Warfarin: 3.45 events per 100 patient-years. However, in the full intention-to-treat analysis, the superiority of rivaroxaban over warfarin did not achieve statistical significance (p=0.177). Intracerebral hemorrhage occurred in 55 patients on riveroxaban and 84 on warfarin (p=0.019). The main implication is that we have an alternative to warfarin, said Robert Califf, M.D., co-principal investigator of the study, in an AHA press release. Equally important, there was no increase in bleeding, so we have a drug you can take once a day, without monitoring, that is at least as good as warfarin and carries no additional risk.")
28
Can’t Take Warfarin?? Frail, falls GI bleeds Cerebral bleeds
Stroke despite therapeutic warfarin Non-compliant / labile INR (Do not want warfarin)
")
29
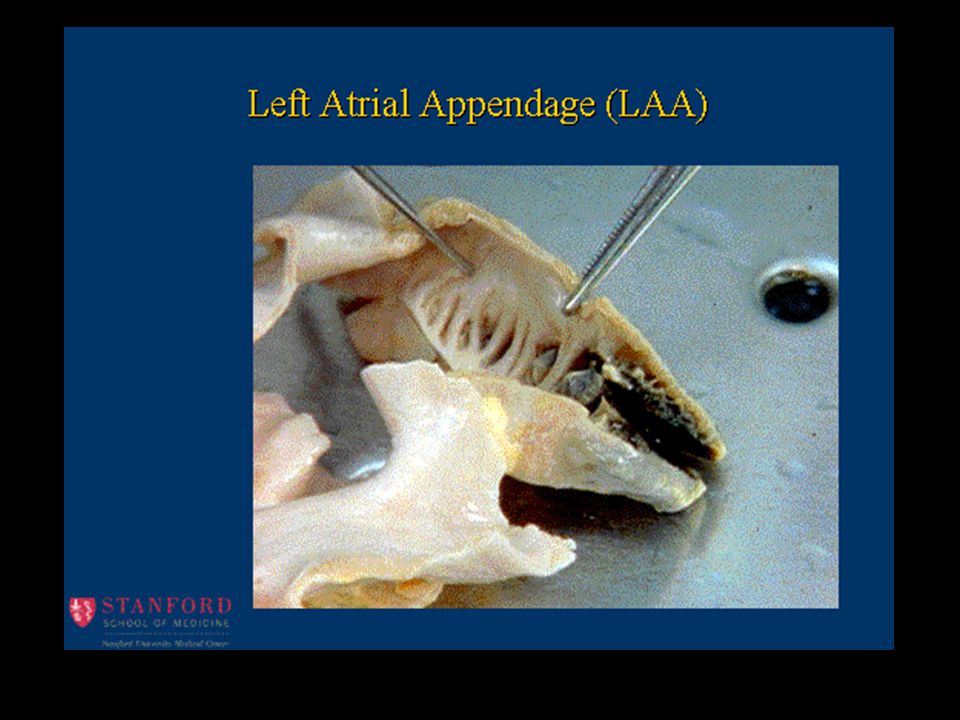
90% of clots in appendage

30
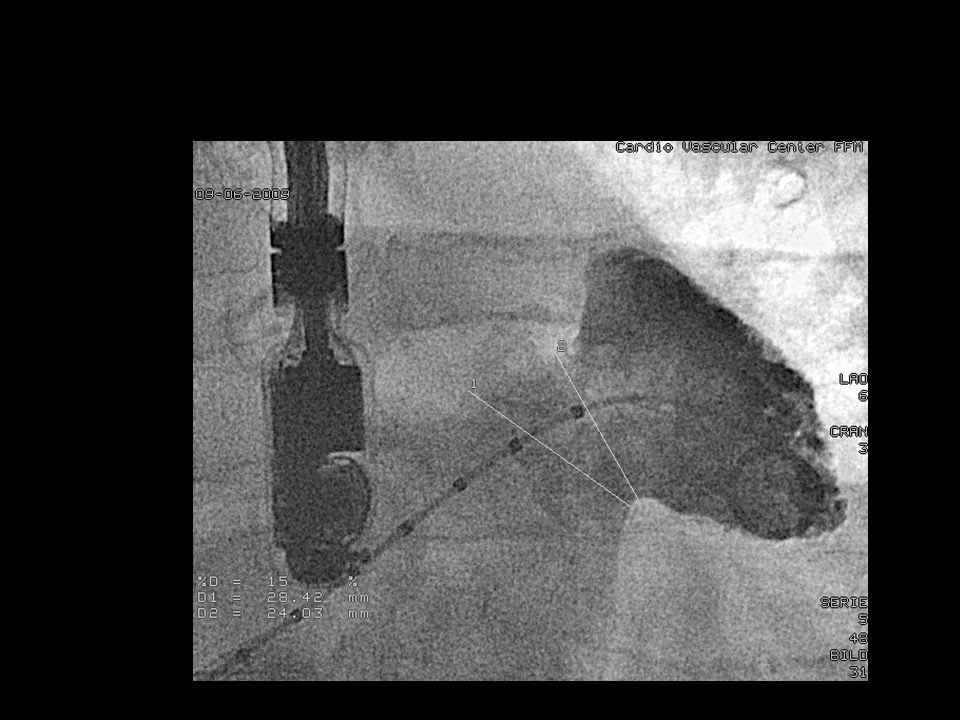
Left Atrial Appendage Occluders
Transcatheter Occlusion of the LAA Currently available in limited markets AMPLATZER® Cardiac Plug WATCHMAN®

35
Device Event Rate (95% CI) Control Event Rate (95% CI)
WATCHMAN® PROTECT – AF: Updated Data (Bayesian sequential design) Primary Safety Results End Point Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort 48 8.7 ( ) 13 4.2 ( ) 2.08 ( ) Primary Efficacy Results End Point Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort 20 3.4 ( ) 16 5.0 ( ) 0.68 ( ) All Stroke, HS, and IS by Intervention End Point Device Event Rate (95% CI) Control Event Rate (95% CI) Relative Risk (95% CI) All Stroke 2.6 ( ) 3.5 (1.7 – 5.7) 0.74 (0.36 – 1.76) IS 2.4 (1.3 – 3.9) 1.6 (0.5 – 3.1) 1.53 (0.654 – 5.43) HS 0.2 ( ) 1.9 (0.7 – 3.7) 0.09 (0.00 – 0.45) Holmes DR: ACC & i2 Summit 2009
 Primary Safety Results. End Point. Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort ( ) ( ) 2.08 ( ) Primary Efficacy Results. End Point. Device Events (n) Device Rate (95% CI) Control Event (n) Control Rate (95% CI) Relative Risk (95% CI) 900 pts-yr cohort ( ) ( ) 0.68 ( ) All Stroke, HS, and IS by Intervention. End Point. Device Event Rate (95% CI) Control Event Rate (95% CI) Relative Risk (95% CI) All Stroke. 2.6 ( ) 3.5 (1.7 – 5.7) 0.74 (0.36 – 1.76) IS. 2.4 (1.3 – 3.9) 1.6 (0.5 – 3.1) 1.53 (0.654 – 5.43) HS. 0.2 ( ) 1.9 (0.7 – 3.7) 0.09 (0.00 – 0.45) Holmes DR: ACC & i2 Summit")
36
Protect AF – 21month F/U

37
Vergelegen Experience
7 patients – all elderly men with Chads>2 Significant GI bleeds on warfarin Warfarin stopped – 2 had small strokes One INR very labile due to recurrent UTI (antibiotics. Suprapubic catheter) All discharged next day – ASA and plavix for 1 month then ASA alone.
 All discharged next day – ASA and plavix for 1 month then ASA alone.")
Similar presentations













![Patients Are Undertreated NABOR Warfarin/Warfarin + Aspirin No Treatment Patients, % Waldo AL, et al. J Am Coll Cardiol. 2005;46:1729-1736. [3] Retrospective.](/13/3883392/big_thumb.jpg "Patients Are Undertreated NABOR Warfarin/Warfarin + Aspirin No Treatment Patients, % Waldo AL, et al. J Am Coll Cardiol. 2005;46:1729-1736. [3] Retrospective.>")












 study To reviewers and moderators: These.>")

