Download presentation
Presentation is loading. Please wait.

1
TMJ and Temporomandibular Joint Disorder
Dr. Soukaina Ryalat

2
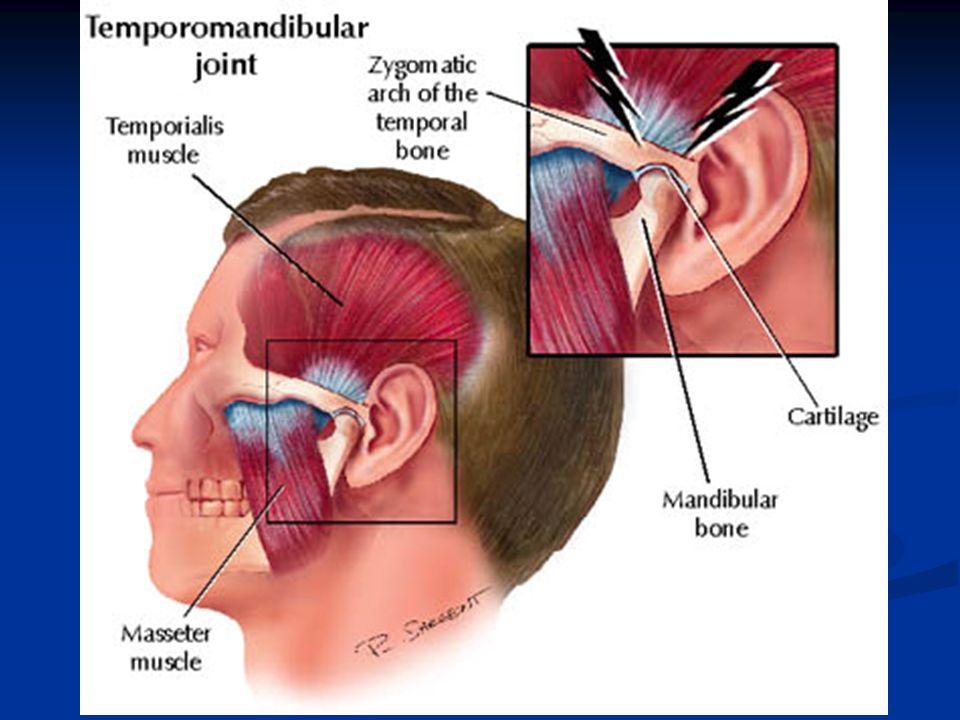
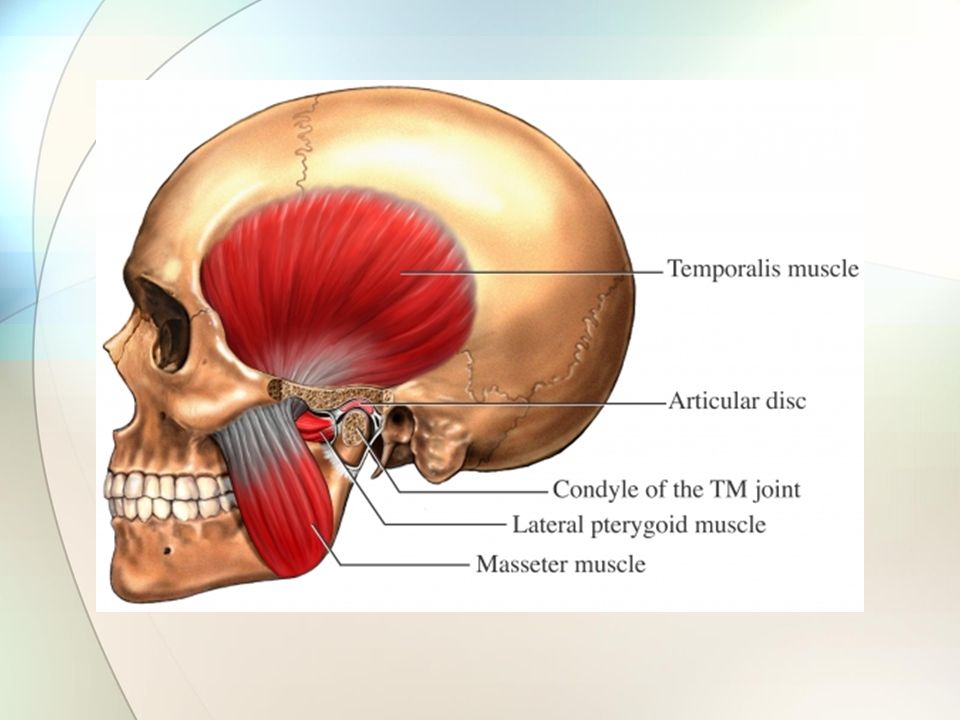
Basic Anatomy Basic Structure Mandibular condyle Temporal bone
Meniscus Coronoid proces

4
TMJ Anatomy continued Primary articulation is formed by the mandibular condyle and the mandibular fossa It is considered a “sliding” hinge joint and allows movement in only one plane, forward and backward movement

5
TMJ Articular Disc Function
Transmits forces, protects, lubricates the articulating surfaces Divided into 3 portions, anterior, intermediate and posterior Movement is mediated by lateral pterygoid attachment on the anterior disc, retrodiscal tissue on the posterior disc and the amount of synovial fluid in the joint capsule Anterior

6
TMJ Disc Facts The intermediate portion is the thinnest and has very little or no innervation or vascularity. Its nutrition comes from the synovial fluid pressed into it by the properly aligned condyle and fossa during closure The anterior and posterior portion is highly vascularized and innervated and also receives some nutrition from synovial fluid

7
Facts on TMJ Most soft clicking noise are not an indicator of joint dysfunction and are of no clinical significance Loud clicking while opening, with deviation present on opposite side, clinically significant of possible anterior condyle displacement. Loud clicking while closing, with deviation present on opposite side, clinically significant of possible posterior condyle displacement. Signs/Symptoms of TMD

8
More TMJ Facts 40% of population have some type of joint noise, indicating the existence of possible disc problems 24% have some head, neck and/or face pain 12% report pain when opening

10
The temporomandibular (TM) joint is located one fingertip-width in front of the auditory meatus, the external opening for the ear canal. The TMJ is comprised of muscles, blood supplies, nerves, and bones. You have 2 TMJs, one on each side of your jaw. Muscles involved in chewing (mastication) also open and close the mouth. The jawbone itself, controlled by the TMJ, has 2 movements: rotation or hinge action, which is opening and closing of the mouth, and gliding action, a movement that allows the mouth to open wider. The coordination of this action also allows you to talk, chew, and yawn. A small disc of cartilage separates the bones, much like in the knee joint, so that the mandible may slide easily; each time you chew you move it.
 also open and close the mouth. The jawbone itself, controlled by the TMJ, has 2 movements: rotation or hinge action, which is opening and closing of the mouth, and gliding action, a movement that allows the mouth to open wider. The coordination of this action also allows you to talk, chew, and yawn. A small disc of cartilage separates the bones, much like in the knee joint, so that the mandible may slide easily; each time you chew you move it.")
11
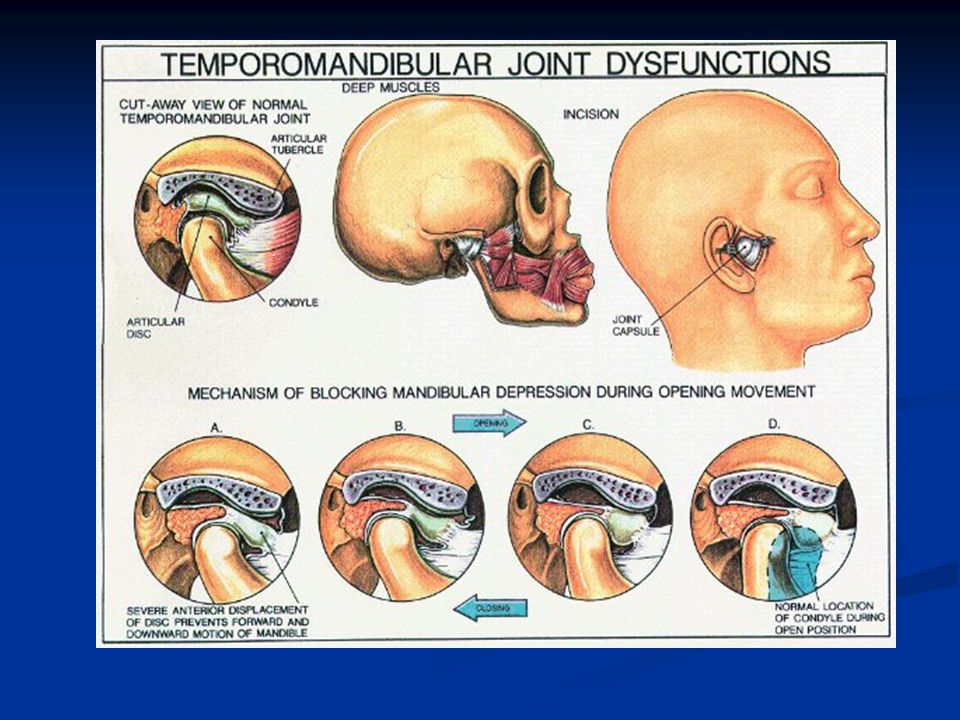
Enlargement of Temporomandibular Joint with Jaw Closed

12
Enlargement of Temporomandibular Joint with Jaw Open - Injured - Medical Illustration

13
TMJ Disorders Temporomandibular joint and muscle disorders, commonly called “TMJ” or TMD are a group of conditions that cause pain and dysfunction in the jaw joint and the muscles that control jaw movement.

14
TMJ Disorder dysfunctional conditions involving the masticatory system
“TMJ syndrome” previous teminology Temporomandibular dysfunction (TMD) is a term used to describe a number of dysfunctional conditions involving the masticatory system. (Masticatory Muscles- Surrounding the joint are groups of muscles that contract and relax in harmony so the jaws function properly (TIME). When the muscles are relaxed and flexible, and not under stress, they work in harmony with the other parts of the TMJ complex) PICTURE TMD is a common condition arising from one or more of numerous factors, including but not limited to tooth position (orthodontic), muscular tonus and harmony, trigger point referrals, cranial compression, damaged or misaligned articular disc, or other intracapsular disorders, such as arthritis or infection and injury by blow. There are many other suspected contributing factors, such as emotional well-being, mineral and hormonal imbalances, nutritional factors, allergies and chemical exposures. The previously used term ‘TMJ syndrome’ is reflective of dysfunctions within the joint capsule, whereas TMD reflects possibilities of involvement of other factors, such as occlusal interferences, muscular disorders, neurological disorders and biochemical imbalances.
 is a term used to describe a number of dysfunctional conditions. involving the masticatory system. (Masticatory Muscles- Surrounding the joint are groups of muscles that contract and relax in harmony so the jaws function properly (TIME). When the muscles are relaxed and flexible, and not under stress, they work in harmony with the other parts of the TMJ complex) PICTURE. TMD is a common condition arising from one or more of numerous factors, including. but not limited to tooth position (orthodontic), muscular tonus and harmony, trigger point referrals, cranial compression, damaged or misaligned articular disc, or other intracapsular disorders, such as. arthritis or infection and injury by blow. There are many other suspected contributing factors, such as emotional. well-being, mineral and hormonal imbalances, nutritional factors, allergies and chemical exposures. The previously used term ‘TMJ syndrome’ is reflective of dysfunctions within the joint capsule, whereas TMD reflects. possibilities of involvement of other factors, such as occlusal interferences, muscular disorders, neurological. disorders and biochemical imbalances.")
15
TMJ Disorders For most people, pain in the area of the jaw joint or muscles does not signal a serious problem. Generally, discomfort from these conditions is occasional and temporary, often occurring in cycles. The pain eventually goes away with little or no treatment. Some people, however, develop significant, longterm symptoms.

16
TMJ Muscles Temporalis - closes jaw and retracts mandible
Masseter – closes jaw Internal or medial Pterygoid – closes jaw External or lateral Pterygoid – opens jaw, moves jaw side to side and protrudes mandible

19
TMJ Disorder dysfunctional conditions involving the masticatory system
“TMJ syndrome” previous teminology Temporomandibular dysfunction (TMD) is a term used to describe a number of dysfunctional conditions involving the masticatory system. (Masticatory Muscles- Surrounding the joint are groups of muscles that contract and relax in harmony so the jaws function properly (TIME). When the muscles are relaxed and flexible, and not under stress, they work in harmony with the other parts of the TMJ complex) PICTURE TMD is a common condition arising from one or more of numerous factors, including but not limited to tooth position (orthodontic), muscular tonus and harmony, trigger point referrals, cranial compression, damaged or misaligned articular disc, or other intracapsular disorders, such as arthritis or infection and injury by blow. There are many other suspected contributing factors, such as emotional well-being, mineral and hormonal imbalances, nutritional factors, allergies and chemical exposures. The previously used term ‘TMJ syndrome’ is reflective of dysfunctions within the joint capsule, whereas TMD reflects possibilities of involvement of other factors, such as occlusal interferences, muscular disorders, neurological disorders and biochemical imbalances.
 is a term used to describe a number of dysfunctional conditions. involving the masticatory system. (Masticatory Muscles- Surrounding the joint are groups of muscles that contract and relax in harmony so the jaws function properly (TIME). When the muscles are relaxed and flexible, and not under stress, they work in harmony with the other parts of the TMJ complex) PICTURE. TMD is a common condition arising from one or more of numerous factors, including. but not limited to tooth position (orthodontic), muscular tonus and harmony, trigger point referrals, cranial compression, damaged or misaligned articular disc, or other intracapsular disorders, such as. arthritis or infection and injury by blow. There are many other suspected contributing factors, such as emotional. well-being, mineral and hormonal imbalances, nutritional factors, allergies and chemical exposures. The previously used term ‘TMJ syndrome’ is reflective of dysfunctions within the joint capsule, whereas TMD reflects. possibilities of involvement of other factors, such as occlusal interferences, muscular disorders, neurological. disorders and biochemical imbalances.")
20
Intrajoint dysfunction Psychological factors Biochemical factors
TMD reflects possibilities of involvement of other factors, not just the joint capsule Occlusal factors Intrajoint dysfunction Psychological factors Biochemical factors Skeletal misalignments The previously used term ‘TMJ syndrome’ is reflective of dysfunctions within the joint capsule, whereas TMD reflects possibilities of involvement of other factors, such as occlusal interferences, muscular disorders, neurological disorders and biochemical imbalances. occlusal factors (premature contacts, loss of vertical dimension), intrajoint dysfunction (adhesions, scarring, disc displacements, disc destruction, and arthrosis), psychological factors (stress, emotional distress, depression and neurosis), biochemical factors (hormonal, dietary neurostimulants, allergies, chemical exposures, prescription, over-the-counter and recreational drugs, mineral/vitamin deficiencies and Biochemical imbalances) skeletal misalignments (including cranial distortions).
, intrajoint dysfunction. (adhesions, scarring, disc displacements, disc destruction, and arthrosis), psychological factors (stress, emotional distress, depression and neurosis), biochemical factors (hormonal, dietary neurostimulants, allergies, chemical exposures, prescription, over-the-counter and recreational drugs, mineral/vitamin deficiencies and. Biochemical imbalances) skeletal misalignments (including cranial distortions).")
21
What are TMJ Disorders? TMJ disorders fall into three main categories:
Myofascial pain, the most common temporo- mandibular disorder, involves discomfort or pain in the muscles that control jaw function. Internal derangement of the joint involves a displaced disc, dislocated jaw, or injury to the condyle. Arthritis refers to a group of degenerative or inflammatory joint disorders that can affect the temporomandibular joint

22
The most common type of TMJ disorder is myofascial pain and dysfunction, usually as a result of bruxism and jaw clenching Related to stress, anxiety, depression or chronic pain 3 cardinal features of TMJ are orofacial pain, restricted jaw function and noise in the jaw

23
TMD is characterized by many symptoms Headache
Burning or tingling sensation Tenderness and swelling Clicking or popping Reduced ROM Ear pain w/o infections Neck and or facial pain TMD is characterized by many symptoms that could arise from other ailments, and it therefore has a reputation as an elusive, baffling condition. These symptoms include headache, toothache, burning or tingling sensations in the face, tenderness and swelling on the sides of the face, clicking or popping of the jaw when opening or closing the mouth, reduced range of motion of the mandible, ear pain without infection, hearing changes, dizziness, sinus-type pain and neck pain (Kaplan & Williams 1988, Moles 1989). Referred pain pattern
. Referred pain pattern.")
24
Grinding teeth at night
Pain that worsens with stress Pain with opening of your mouth Teeth that meet differently from time to time Pain while chewing

25
Summary of Symptoms: History of trauma, blow to jaw, MVA ( motor vehicle accident), dental malocclusions Pain and tenderness of the TMJ Head and/or ear pain Sore and stiff jaw muscles Locking of the jaw in a shut or open position Frequent headaches and/or neck aches Pain that worsens when teeth are clenched

26
Referred pain pattern of TMJ

27
sternomestoid; (B) upper trapezius; (C) temporalis; (D) masseter.
A complete postural evaluation will examine for forward head posture and pelvic position, which may contribute to head placement. Since Louise has complained of lower back discomfort, the lower back and pelvis should be addressed at some point. An exercise programme to strengthen weak postural muscles will help to inhibit hypertonic ones as well as provide structural support for proper head placement. She should evaluate her sitting posture at the computer and pay attention to unnecessary leaning, particularly of the head, as well as clenching of the teeth when working. Several muscles are known to contain trigger points (Fig. 18), which refer into Louise’s familiar pain pattern and should be thoroughly examined and treated by neuromuscular techniques (Chaitow 1996), spray and stretch or injection (Travell & Simons 1983). These muscles include the temporalis, masseter, both pterygoids, upper trapezius, sternocleidomastoid, and suboccipital muscles and attachments, which may contribute to forward head position as well as to referred pain (Travell & Simons 1983, Kaplan 1988, Moles 1989, Bonica 1990, Cailliet 1992).
, which refer into Louise’s familiar pain. pattern and should be thoroughly examined and treated by neuromuscular techniques (Chaitow. 1996), spray and stretch or injection (Travell & Simons 1983). These muscles include the temporalis, masseter, both pterygoids, upper trapezius, sternocleidomastoid, and suboccipital muscles and attachments, which may contribute to forward head position as well as to referred pain (Travell & Simons 1983, Kaplan. 1988, Moles 1989, Bonica 1990, Cailliet 1992).")
30
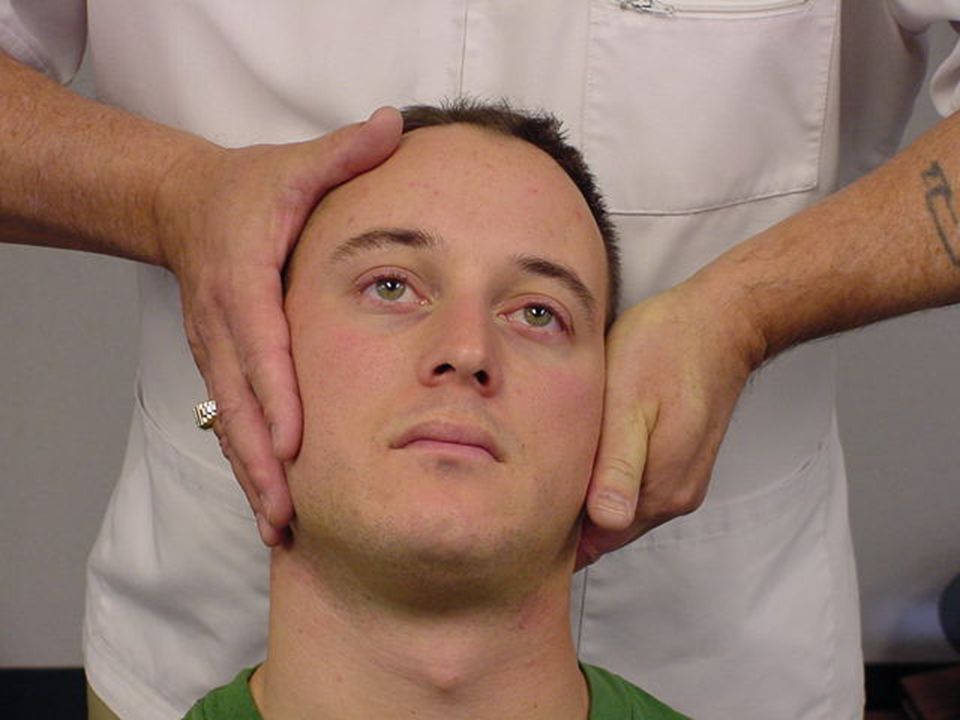
Assessment of TMJ Intercuspid alignment Mandibular gait pattern
Screening (3 finger test) Palpate joint and soft tissues Adjustive procedure Distraction technique Translation technique
 Palpate joint and soft tissues. Adjustive procedure. Distraction technique. Translation technique.")
31
TMJ Examination: History: Bare the area Bilateral observation
Bilateral palpation Active ROM Passive ROM Ortho/neuro X-ray ?

33
Normal opening should be enough to fit 3 fingers into mouth
Normal opening should be enough to fit 3 fingers into mouth. Have the patient use their own fingers.

34
C and S Curve Examination
Normal Watch for deviation from center when patient slowly opens and closes mouth

35
While having the patient slowly open
the mouth feel for the movement of the condyles

38
Alternate Procedure: Inferior Misalignment

39
Arthroscopic Repairs of the TMJ

40
How are TMJ Disorders Treated?
Because more studies are needed on the safety and effectiveness of most treatments for jaw joint and muscle disorders, experts recommend using the most conservative and reversible treatments when possible. Reversible treatments do not cause permanent changes in the structure or position of the jaw or teeth. Even when TMJ disorders have become persistent, most patients still do not need aggressive types of treatment.

41
How are TMJ Disorders Treated?
Treatment by a Prosthodontist may be needed for other reasons such as to restore severely worn, damaged, or diseased teeth or to replace teeth for the purpose of improving chewing, providing enhanced support for your lips or cheeks, or improving the appearance of your smile. Extensive prosthodontic treatment should only be provided after the TMJ disorder has been adequately diagnosed and its pain successfully managed.

42
Conservative Treatments
Most jaw joint and muscle problems are temporary and do not get worse. Treatment is based on a proper diagnosis which should be conservative and reversible. Self-Care Practices Pain Medications Stabilization Splints Prosthodontic Treatment

43
Self-Care Practices Your Prosthodontist may recommend steps that you can take that may be helpful in easing symptoms, such as: eating soft foods, applying ice packs to recommended areas, avoiding extreme jaw movements (such as wide yawning, loud singing, and gum chewing), learning techniques for reducing stress, practicing gentle jaw stretching and relaxing exercises that may help increase jaw movement.
, learning techniques for reducing stress, practicing gentle jaw stretching and relaxing exercises that may help increase jaw movement.")
44
Pain Medications For many people with TMJ disorders, short-term use of over-the-counter pain medicines or nonsteroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen, may provide temporary relief from jaw discomfort. When necessary, your dentist or doctor can prescribe stronger pain or antiinflammatory medications, muscle relaxants, or antidepressants to help ease symptoms.
, such as ibuprofen, may provide temporary relief from jaw discomfort. When necessary, your dentist or doctor can prescribe stronger pain or antiinflammatory medications, muscle relaxants, or antidepressants to help ease symptoms.")
45
Stabilization Splints
Your Prosthodontist may recommend an oral appliance, also called a stabilization splint or bite guard, which is a plastic guard that fits over the upper or lower teeth. Stabilization splints are the most widely used treatments for TMJ disorders. If a stabilization splint is recommended, it should be used only for a short time and should not cause permanent changes in the way your teeth bite together when the splint is removed from your mouth.

46
Prosthodontic Treatment
Occlusal splints may also be used to reestablish the bite prior to prosthodontic treatment. It is used when the bite is not contacting evenly due to missing or worn teeth and may relax the muscles.

47
If a joint is badly damaged and cannot be repaired, it must be removed and replaced. Conditions requiring surgery may include: severe degenerative disease, congenitally deformed TMJs and advanced rheumatoid arthritis. Due to the general risks associated with surgery, this treatment is used only after other treatment options have been considered. Over the past 20 years, total joint replacement surgeries have become a safer and more common option for those suffering with TMJ disease. As these surgeries have become more mainstream, a variety of prosthetic TMJ joints Partial joint replacement When only one of the components (disk, ball or socket) of the TMJ is replaced, it is called a partial joint replacement. If the temporal bone no longer provides a smooth socket (articular fossa), a metal liner (fossa replacement) is placed inside the TMJ to restore motion and flexibility in the TMJ. When the ends of the jawbone (condyles) are damaged and no longer ball-shaped, they can be replaced. Surgeons can harvest bone from another part of the patient's body, such as the ribs, and attach it with screws to the damaged section of the TMJ. A metal prosthesis is often used instead of bone because less surgery is needed, since there is no "donor" site. Total joint replacement In a total joint procedure the original ball and joint are both replaced with metal parts. Once inserted, the two metal components slide smoothly across each other's surfaces, eliminating any painful grinding and consequently eliminating the need for a disk. As padding is no longer needed, the disk is removed.Those with joint replacement will face some restrictions with their new prosthesis. Just like knee replacement patients are not advised to run marathons, certain lifestyle and behavioral changes are suggested to minimize pain and reduce stress on the TMJ
 of the TMJ is replaced, it is called a partial joint replacement. If the temporal bone no longer provides a smooth socket (articular fossa), a metal liner (fossa replacement) is placed inside the TMJ to restore motion and flexibility in the TMJ. When the ends of the jawbone (condyles) are damaged and no longer ball-shaped, they can be replaced. Surgeons can harvest bone from another part of the patient s body, such as the ribs, and attach it with screws to the damaged section of the TMJ. A metal prosthesis is often used instead of bone because less surgery is needed, since there is no donor site. Total joint replacement. In a total joint procedure the original ball and joint are both replaced with metal parts. Once inserted, the two metal components slide smoothly across each other s surfaces, eliminating any painful grinding and consequently eliminating the need for a disk. As padding is no longer needed, the disk is removed.Those with joint replacement will face some restrictions with their new prosthesis. Just like knee replacement patients are not advised to run marathons, certain lifestyle and behavioral changes are suggested to minimize pain and reduce stress on the TMJ.")
Similar presentations
















>")







