Download presentation
Presentation is loading. Please wait.

1
Hypovolemic shock Hypovolemic shock Case and discussion By R1 張家穎

2
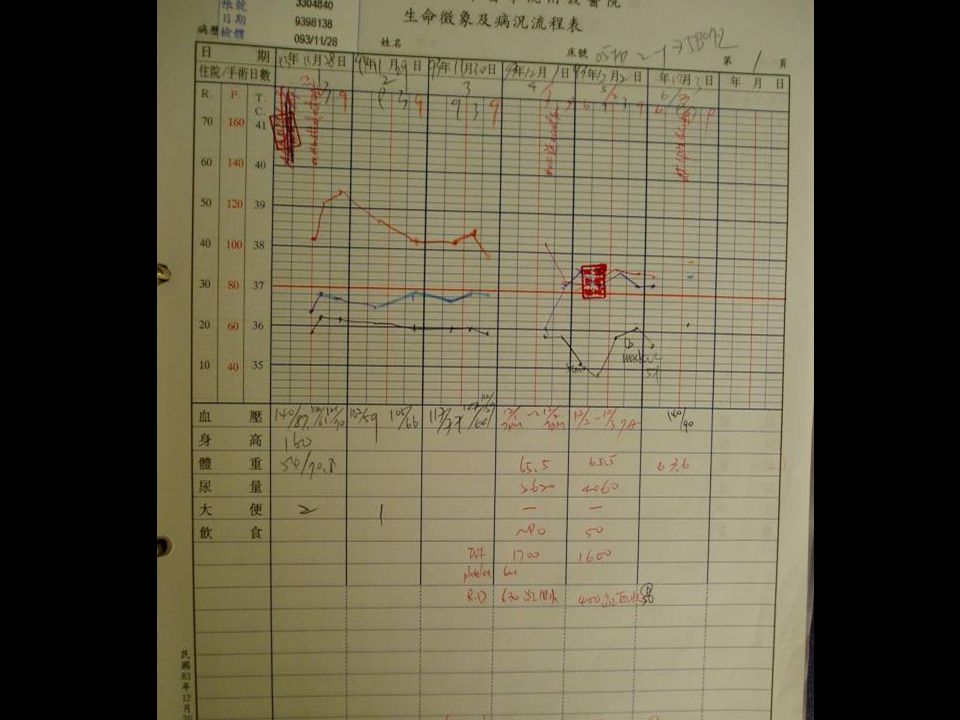
A 38 y/o pregnant woman is diagnosed of placenta acreta. C/S was performed smoothly. She was then sent to our POR………………..

3
Check Abd.Sono. Keep obs. c/o:bil.leg pain. pulse:weak Remove bil.TAE pH: 7.464 pO2: 85.9 pCO2: 23.8 HCO3-: 17.2 O2Sat: 97.3 B.E.: -6.8 Na+: 138 K+: 4.6 Cl-: 114 Ca++: 0.99 Hb: 6.8 Hct: 20

5
Heart echo: hypovolemia.

6
Anesthetic induction Hypovolemic pts are sensitive to the vasodilating and negative inotropic effects of anesthetic drugs. Spinal or epidural anesthesia- sympathetic blockade. IV induction agents: thiopental and propofol - SVR and myocardial contractility. Etomidate, ketamine, large dose of opioids. prefer

7
IHA : isoflurane producing profound vasodilatation. Muscle relaxants : facilitate intubation. histamine release- atracurium. Positive pressure ventilation- reduce preload.

8
Fluid resuscitation “How much” is primary importance. Further consideration is “What fluid”

9
Fluid resuscitation for the trauma patient Resuscitation 2001;48(1):57-69
:57-69")
10
Intraoperative fluid management - what and how much? Chest 1999;115(5 Suppl):S106-12
:S106-12")
11
Fluid resuscitation for the trauma patient Resuscitation 2001;48(1):57-69
:57-69")
12
Goals Proper intravascular volume is the foundation for cardiovascular function. Maintenance of renal function. Avoidance of lung water accumulation. Minimizing splanchnic and hepatic circulatory insufficiency. Ensuring GI integrity-prevent endotoxemia.

13
Fluid therapy Crystaloid- N.S v.s. L.R. 1. potential effect on electrolyte and acid- base equilibrium. 2. 3:1 ratio. Colloid- controversy. Dextrose solutions- possibility of increasing cerebral acidosis. Oxygen-carrying capacity and coagulation.

14
Intraoperative fluid management - what and how much? Chest 1999;115(5 Suppl):S106-12
:S106-12")
15
The existence of congestive heart failure and pul. edema is a major cause of perioperative morbidity and mortality. Minimize severe hypotension and hypoperfusion during anesthetic induction.

17
Electrolyte and Acid-Base Balance Na+, K+, Cl- are the principal electrolytes affected by the choice of crystalloid solution. NS: hyperchloremic metabolic acidosis. LR: lactate-metabolic alkalosis. Ca++-limited in blood transfusion.

18
Colloid A number of conflicting studies~~ Comparing with crystalloid resuscitation, colloids will increase extravascular lung water and worsen pul. Function. Colloids reduce the incidence of pul. Edema. Lymphatic flow can increase by up to 20 times.

19
Oxygen-carrying capacity. DO2=CaO2*C.O. CaO2=SaO2*Hb*1.31+0.003*PaO2. No difference between restrictive transfusion (Hb: 7-9) and liberal transfusion (Hb: 10-12). Pre-existing cardiopulmonary function is unknown and the concentration of Hb. changes rapidly during resuscitation.
 and liberal transfusion (Hb: 10-12). Pre-existing cardiopulmonary function is unknown and the concentration of Hb. changes rapidly during resuscitation..")
20
Coagulation factor Causes for depletion: hemodilution, intravascular consumption, bone marrow depression, hypersplenism. Most common intra-OP coagulopathy- dilutional thrombocytopenia. FFP Platelate Cryoprecipitate- factor 8.13, fibrinogen Whole blood

21
pT: 11.6/13.5 aPTT: 33.2/29.4

22
I need fluid therpy of this kind.

23
Nutrition, glucose Avoidance of hyperglycemia and hypoglycemia is of increased concern in pts with DM and ES”L”D. Dextrose solutions are generally omitted- hyperglycemia-induced hyperosmolarity, osmotic diuresis and cerebral acidosis.

24
Fluid warming Hypothermia (B.T.<35 ℃ ): The oxyhaemoglobin dissociation curve is shifted to the left. Shivering compounds the lactic acidosis. Increase bleeding. Increase the risk of infection. Increase the risk of cardiac morbid events.

25
Small volume resuscitation Rapid infusion of a small dose (4 ml/kg B.W.) of 7.2%-7.5% NaCl/colloid solution. Endogenous fluid shift along the osmotic gradient form the intracellular to the intravascular compartment. Immediate BP, SVR. Reduction of postischemic reperfusion injury. Pts with head injury benefit more!

26
Small-volume resuscitation: from experimental evidence to clinical routine. Advantages and disadvantages of hypertonic solutions Acta Anaesthesiologica Scandinavica 2002;46(6):625-38
:")
28
Vasopressin in shock states. Exogenous vasopressin injection arterial BP and SVR Vasopressin at a dosage of 2-6 U/hr is effective in reversing catecholamine- resistant vasodilatory shock due to sepsis or after CPB.

29
References. Vasopressin in shock states Current Opinion in Anaesthesiology 2003;16(2):159-64 Small-volume resuscitation: from experimental evidence to clinical routine. Advantages and disadvantages of hypertonic solutions Acta Anaesthesiologica Scandinavica 2002;46(6):625-38 Fluid management of the trauma patient Current Opinion in Anaesthesiology 2001;14(2):221-5 Fluid resuscitation for the trauma patient Resuscitation 2001;48(1):57-69 Intraoperative fluid management - what and how much? Chest 1999;115(5 Suppl):S106-12 Lange clinical Anesthesiology, 3rd edition.
: Small-volume resuscitation: from experimental evidence to clinical routine. Advantages and disadvantages of hypertonic solutions Acta Anaesthesiologica Scandinavica 2002;46(6): Fluid management of the trauma patient Current Opinion in Anaesthesiology 2001;14(2):221-5 Fluid resuscitation for the trauma patient Resuscitation 2001;48(1):57-69 Intraoperative fluid management - what and how much. Chest 1999;115(5 Suppl):S Lange clinical Anesthesiology, 3rd edition..")
30
Near “”the end” The end!

31
Wait~~~ Wait~~

33
No more use of nasal canula. SaO2:97% Mild dyspnea when rapid iv. Loading. Not any memory of POR and 2nd emergent surgery. She is happy with her husband and twin babies. Bye!!

Similar presentations