Download presentation
Presentation is loading. Please wait.

1
Necrotizing Fasciitis Dolan Wenner, D.O. Internal Medicine Lecture Series 1/31/07

2
Necrotizing Fasciitis Definition – commonly referred to as “flesh-eating bacteria,” it is a rare infection of the deeper layers of the skin and subcutaneous tissue (fascia)
")
3
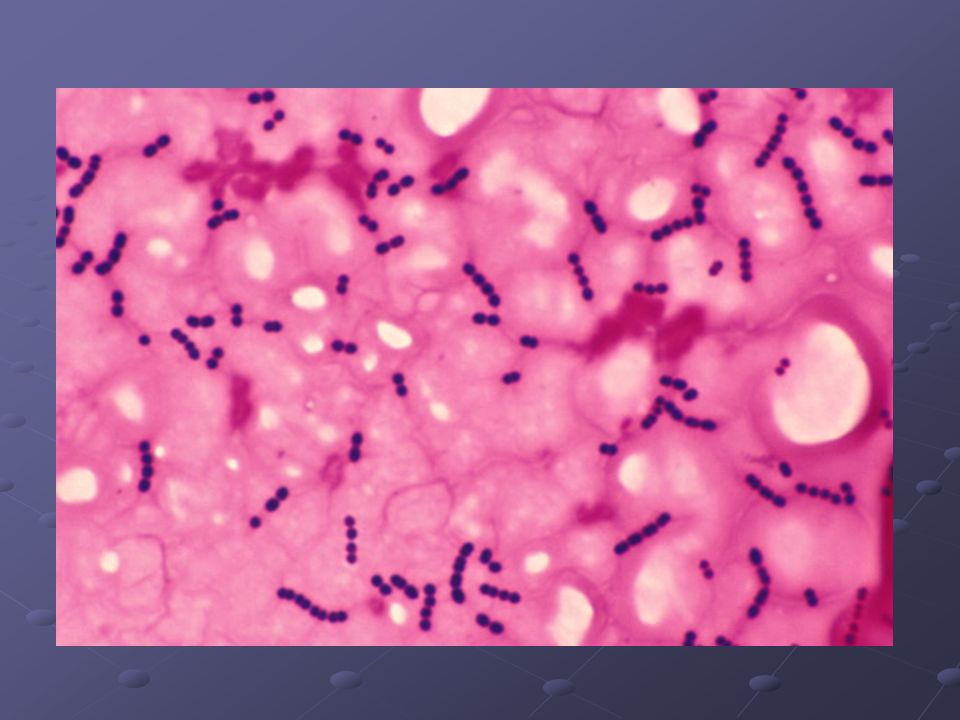
Organisms Most common associated organism is group A beta-hemolytic streptococci Other isolated organisms: Staph. aureus, Clostridium perfringens, Staph. Epidermidis, enterococci, Enterobacteriaceae species, E. coli, Proteus mirabilis, Klebsiella pneumonia, Pseudomonas aeruginosa, Bacteroides/Prevotella species, anaerobic gram- positive cocci

4
Pathophysiology Organisms spread from the subcutaneous tissue along the superficial and deep fascial planes facilitated by bacterial enzymes and toxins M1 and M3 surface proteins – increase adherence of streptococci to the tissues, also protects bacteria against neutrophilic phagocytosis Streptococcal pyrogenic exotoxins (SPEs) A, B, C and streptococcal superantigens (SSA) – lead to the release of cytokines and produce clinical signs such as hypotension
 A, B, C and streptococcal superantigens (SSA) – lead to the release of cytokines and produce clinical signs such as hypotension")
5
Pathophysiology Deep infection can cause Vascular occlusion Vascular occlusion Ischemia Ischemia Tissue necrosis Tissue necrosis Nerve damage Nerve damage Septicemia (systemic toxicity) Septicemia (systemic toxicity)
 Septicemia (systemic toxicity)")
6
Necrotizing Fasciitis syndromes Type I (polymicrobial) Type II group A beta-steoptococcal Type III gas gangrene (clostridial myonecrosis)
 Type II group A beta-steoptococcal Type III gas gangrene (clostridial myonecrosis)")
7
NF – Type I Polymicrobial Typically occurs after surgery or trauma Can be mistaken for simple wound cellulitis May also be observed with urogenital or anogenital infections Aerobic and anearobic bacteria usually found in combination work synergistically Variant of NF – saltwater NF, usually minor skin would contaminated with saltwater that contains Vibrio species

9
NF – Type II So-called “flesh-eating bacterial infection” Monomicrobial Caused by group A beta-streptococcus Varicella infection and use of non-steroidal anti-inflammatory drugs may be predisposing factors

11
NF – Type III Gas gangrene (clostridial myonecrosis) Usually caused by Clostridium perfringens When this type occurs spontaneously, Clostridium septicum most likely etiologic agent usually occur in association with colon CA or leukemia Skeletal muscle infection may be associated with recent surgery or trauma
 Usually caused by Clostridium perfringens When this type occurs spontaneously, Clostridium septicum most likely etiologic agent usually occur in association with colon CA or leukemia Skeletal muscle infection may be associated with recent surgery or trauma")
14
NF – History and Physical Exam History Fever and chills Fever and chills Erythema noted Erythema noted Supralesional vesiculation or bullae formation Supralesional vesiculation or bullae formation Serosanguinous fluid drainage Serosanguinous fluid drainage Recent history of skin biopsy, illicit drug use, frostbite, chronic venous stasis ulcers, open bone fractures, insect bites, surgical wounds, and skin abcesses Recent history of skin biopsy, illicit drug use, frostbite, chronic venous stasis ulcers, open bone fractures, insect bites, surgical wounds, and skin abcesses History of Diabetes History of Diabetes

17
NF – History and Physical Exam Physical Exam Rapidly advancing erythema Rapidly advancing erythema Painless ulcers Painless ulcers Black necrotic eschar may be evident at the borders of the affected areas Black necrotic eschar may be evident at the borders of the affected areas Vesiculation or bullae formation may be noted Vesiculation or bullae formation may be noted Sepsis/shock Sepsis/shock Gas may be evident (crepitus) Gas may be evident (crepitus) Pain out of proportion to exam Pain out of proportion to exam
 Gas may be evident (crepitus) Pain out of proportion to exam Pain out of proportion to exam")
19
Cellulitis vs. NF The following may suggest NF Rapid progression Rapid progression Poor therapeutic response Poor therapeutic response Blistering necrosis Blistering necrosis Cyanosis Cyanosis Extreme local tenderness Extreme local tenderness High temperature High temperature Tachycardia Tachycardia Hypotension Hypotension Altered level of consciousness Altered level of consciousness

20
Lab Studies Elevated WBCs Hyponatremia Elevated BUN AnemiaHypocalcemiaAcidosisThrombocytopenia Prolonged PT associated with higher mortality rate

21
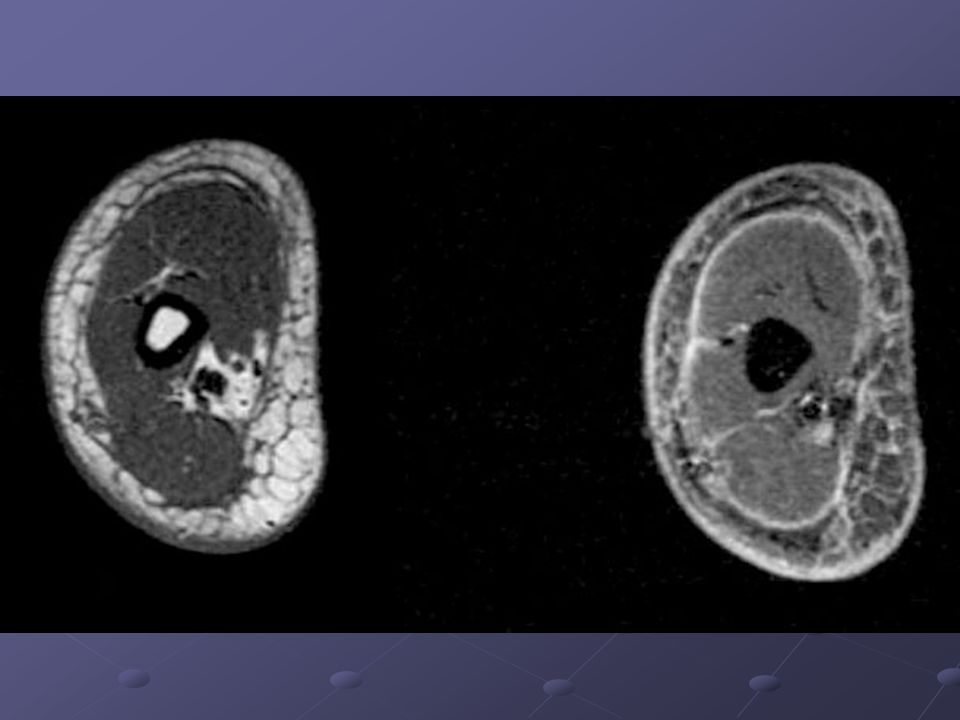
Imaging Studies Standard radiographs – little value unless free air is depicted, as with gas-forming infections CT – can show subcutaneous air T2-weighted MRIs may show well-defined regions of high signal intensity in the deep tissues sensitivity exceeds specificity CT and MRI may be useful in directing rapid surgical debridement

24
Other Tests Excisional deep tissue biopsy is gold standard Gram staining (can help delineate between Type I and Type II) Cultures
 Cultures")
27
Treatment Transfer pt to ICU or Surgical ICU Maintain hemodynamic parameters Surgical Debridement Combination antibiotic therapy Single antibiotic therapy Vancomycin Hyperbaric oxygen (HBO) may reduce mortality rate, but no literature to support IVIG anecdotal evidence
 may reduce mortality rate, but no literature to support IVIG anecdotal evidence")
28
Treatment Surgical Debridement Incisions should be deep and extend beyond the areas of necrosis until viable tissue is reached Incisions should be deep and extend beyond the areas of necrosis until viable tissue is reached Wound should be well irrigated Wound should be well irrigated Hemostasis should be maintained Hemostasis should be maintained Wound should be kept open Wound should be kept open Debridement and evaluations should be repeated on a daily basis Debridement and evaluations should be repeated on a daily basis

29
Treatment Antimicrobial therapy Ampicillin (Principen, Omnipen) Ampicillin (Principen, Omnipen) Gentamicin (Garamycin, Jenamicin) Gentamicin (Garamycin, Jenamicin) Clindamycin (Cleocin) Clindamycin (Cleocin) Metronidazole (Flagyl) Metronidazole (Flagyl) Imipenem and cilastatin (Primaxin) Imipenem and cilastatin (Primaxin) Ampicillin and sulbactam (Unasyn) Ampicillin and sulbactam (Unasyn) Piperacillin-tazobactam (Zosyn) Piperacillin-tazobactam (Zosyn) Vancomycin Vancomycin Amphotericin B Amphotericin B
 Ampicillin (Principen, Omnipen) Gentamicin (Garamycin, Jenamicin) Gentamicin (Garamycin, Jenamicin) Clindamycin (Cleocin) Clindamycin (Cleocin) Metronidazole (Flagyl) Metronidazole (Flagyl) Imipenem and cilastatin (Primaxin) Imipenem and cilastatin (Primaxin) Ampicillin and sulbactam (Unasyn) Ampicillin and sulbactam (Unasyn) Piperacillin-tazobactam (Zosyn) Piperacillin-tazobactam (Zosyn) Vancomycin Vancomycin Amphotericin B Amphotericin B")
30
NF – Complications Sepsis and renal failure Metastatic plaques may occur Septicemia leads to severe system toxicity and rapid death unless treated quickly and appropriately

31
NF - Prognosis Poor prognosis linked to certain streptococcal strains Mortality rate can be as high as 25% Cases of NF with renal failure and sepsis have mortality rate as high as 70% Early recognition and appropriate treatment can help ensure better prognosis

32
Thank you!

33
Question 1 What is the most common organism associated with necrotizing fasciitis (“flesh-eating disease”)? A.E. coli B.Group A beta-hemolytic streptococci C.Pseudomonas aeruginosa D.Proteus mirabilis

34
Question 1 What is the most common organism associated with necrotizing fasciitis (“flesh-eating disease”)? A.E. coli B.Group A beta-hemolytic streptococci C.Pseudomonas aeruginosa D.Proteus mirabilis

35
Question 2 What test is considered the “gold standard” for diagnosis of necrotizing fasciitis? A.MRI B.CT scan C.Excisional deep tissue biopsy D.Cultures

36
Question 2 What test is considered the “gold standard” for diagnosis of necrotizing fasciitis? A.MRI B.CT scan C.Excisional deep tissue biopsy D.Cultures

37
Question 3 What is the organism that is most commonly associated with Type III necrotizing fasciitis? A.Group A beta-hemolytic streptococci B.Proteus mirabilis C.Clostridium perfringens D.Staphylococcus aureus

38
Question 3 What is the organism that is most commonly associated with Type III necrotizing fasciitis? A.Group A beta-hemolytic streptococci B.Proteus mirabilis C.Clostridium perfringens D.Staphylococcus aureus

39
The End

Similar presentations


















 David A Wininger, MD Internal Medicine Residency Program Director Associate Professor, Clinical.>")




 –Bacteria or their products may migrate to adjacent tissues or bloodstream.>")




