Download presentation
Presentation is loading. Please wait.

1
Necrotizing Fasciitis
By Dr.Hana’a Tashkandi

2
Necrotizing Fascitiis
Definition Risk factors Etiology Pathophysiology Epidemiology Clinical Features Investigations Management

3
Diffuse Necrotizing Infection (flesh-eating)
Dangerous………………Why?

4
Difficult to diagnose Extremely toxic Spread rapidly May lead to limb amputation

5
Classification @ Colistridial : # Necrotizing cellulitis # Myositis
@ Non-colistridial : # NECROTIZING FASCIITIS # Streptococcal gangrene

6
Necrotizing Fasciitis
It is a progressive, rapidly spreading, inflammatory infection located in the deep fascia with 2ry necrosis of the subcutaneous tissue.

7
Risk Factors Immunocompression illnesses
e.g.: DM, Cancer, alcoholism, vascular insufficiency, organ transplant, HIV or neutropenia. Trauma or foreign bodies in surgical wound. Idiopathic as scrotal or penile necrotizing fasciitis.

8
Causative Agents It is a mixed microbial flora:
# microaerophilic streptococci. # staphylococci. # aerobic gram –ve # anaerobes ( peptostreptococi – bacteroids)
")
9
Pathophysiology

10
Mortality & Morbidity The overall morbidity & mortality is 70 – 80%
Fournier’s gangrene has a reported mortality as high as 75%

11
Sex: Male : Female :1 Age: * the mean age is 38 to 44 years. * pediatric cases are rare but reported from countries where poor hygiene in.

12
Clinical Features Symptoms:
*sudden onset of pain and swelling at the site of trauma or recent surgery. *in some cases, the symptoms may begin at the site distant from the initial traumatic insult. *Fournier's gangrene begin with pain and itching of the scrotal skin.

13
Clinical Features (cont.)
Sings: * pt. appears moderately to severely toxic (but sometimes might looks well) * typically, erythema that quickly spread over a course of hours to days. * the redness quickly spread & the margin of infection move out into normal skin without being raised nor sharply demarcated. * anesthesia # Note: *I.M. injections & I.V. infusions may lead to necrotizing fasciitis. *minors insect bites may set the stage for necrotizing infections.
 * typically, erythema that quickly spread over a course of hours to days. * the redness quickly spread & the margin of infection move out into normal skin without being raised nor sharply demarcated. * anesthesia. # Note: *I.M. injections & I.V. infusions may lead to necrotizing fasciitis. *minors insect bites may set the stage for necrotizing infections.")
16
Investigations Lab: CBC, U&E, Glu, Creatinine, Blood &
tissue cultures, Urine analysis, & ABG.

17
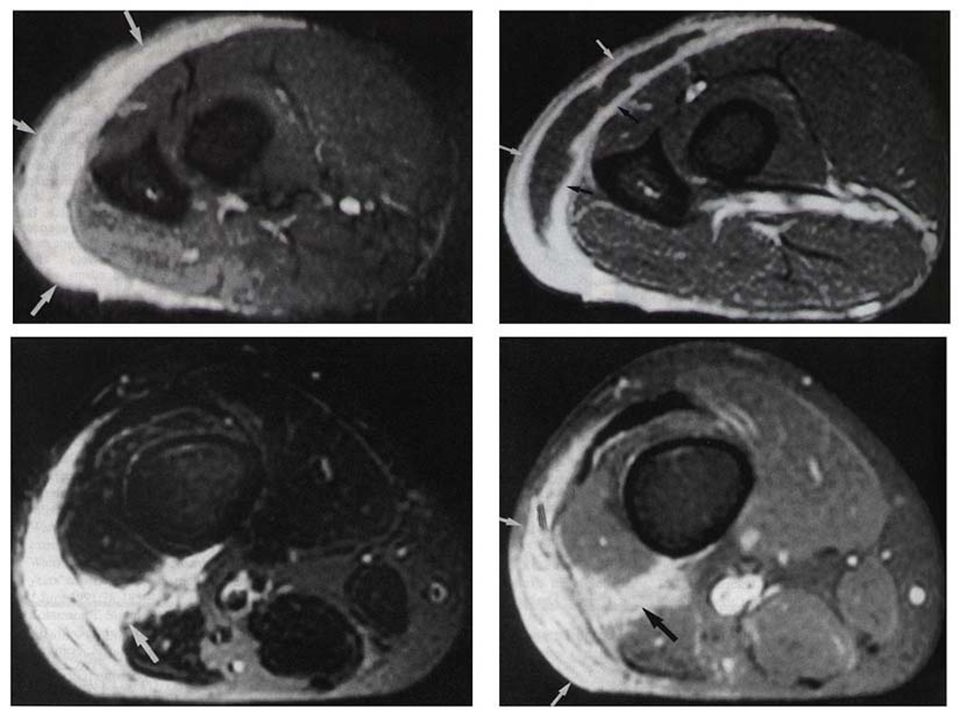
Investigations (cont.)
Imaging Studies: # X-ray gas in the subcutaneous fascia planes. ?? D.D. of subcutaneous gas in a radiograph. # C.T. demonstrating necrosis with asymmetric fascial thickening & gas in the tissues. # MRI.

19
Investigations (cont.)
Microbiology: Gram stain & wound culture Procedures: Biopsy is the best method to use to obtain proper cultures for micro-organisms.

21
Emergency Department care
B C D

22
Management If streptococci are the identified major pathogens, the D.O.C is Penicillin-G with clindamycin as an alternative. To ensure adequate treatment, we have to cover aerobic & anaerobic bacteria. The anaerobic coverage can be provided by Metronidazole or 3rd generation cephalosporin's.

23
Management (cont.) Gentamicine combined with clindamycine or chloramphenicol has been reported as a standard coverage. Ampicilline may be added to the basic regimen to treat enterococci if suspected by gram stain.

24
Further In-Patient Care
Surgical debridment. Fasciotomy. H.B.O.

25
Complications Renal Failure.
Septic Shock with cardiovascular collapse. Scarring with cosmetic deformity.

26
Medico-legal Pitfalls
Early in the course of the disease, necrotizing fasciitis may appear quiet benign. Be wary of the patient with pain out of the proportion to physical finding.

27
THANK YOU Hana’a Tashkandi

Similar presentations














 –Bacteria or their products may migrate to adjacent tissues or bloodstream.>")




 Disease (strep throat, necrotizing fasciitis, impetigo) By: Dr. Awatif Alam.>")


