Download presentation
Presentation is loading. Please wait.

1
Diabetic Foot Infection

2
Of all the late complications of diabetes, foot problems are probably the most preventable. Joslin, who wrote in 1934 that “diabetic gangrene is not heaven-sent, but earth-born

3
Approximately 5% to 10% of diabetic patients have had past or present foot ulceration, and 1% have undergone amputation

4
Foot infections Foot infections are among the
most common and serious complications of diabetes mellitus. Types of infection include cellulitis, myositis, abscesses, necrotizing fasciitis, septic arthritis, tendinitis, and osteomyelitis.

5
Pathophysiology Patients with diabetes are particularly susceptible to foot infection primarily because of neuropathy, vascular insufficiency, and diminished neutrophil function. Peripheral neuropathy has a central role in the development of a foot infection and it occurs in about 30 to 50 percent of patientswith diabetes.

8
Microbiology The most common pathogens in acute, previously untreated, superficial infected foot wounds in patients with diabetes are aerobic gram-positive bacteria, particularly Staphylococcus aureus and beta-hemolytic streptococci (group A, B, and others).
.")
9
Microbiology Infection in patients who have recently received antibiotics or who have deep limb-threatening infection or chronic wounds are usuallycaused by a mixture of aerobic gram-positive, aerobic gram-negative (e.g., Escherichia coli, Proteus species, Klebsiella species), and anaerobic organisms (e.g., Bacteroides species, Clostridium species, Peptococcus and Peptostreptococcus species).
, and anaerobic organisms (e.g., Bacteroides species, Clostridium species, Peptococcus and Peptostreptococcus species).")
10
Key Components of the Comprehensive Diabetic Foot Examination
Dermatologic Skin status: color, thickness, dryness, cracking Sweating Infection: check between toes for fungal infection Ulceration Calluses/blistering: hemorrhage into callus?

11
Musculoskeletal Deformity (e.g., claw toes, prominent metatarsal heads, Charcot joint) Muscle wasting (guttering between metatarsals) Assess whether shoes are appropriate for the feet (e.g., size, width)
 Muscle wasting (guttering between metatarsals) Assess whether shoes are appropriate for the feet (e.g., size, width)")
12
Neurologic Ability to perceive pressure from a 10-g monofilament plus one of the following: Vibration using 128-Hz tuning fork Pinprick sensation Ankle reflexes Vibratory perception threshold

13
VASCULAR Foot pulses Ankle-brachial index, if indicated

14
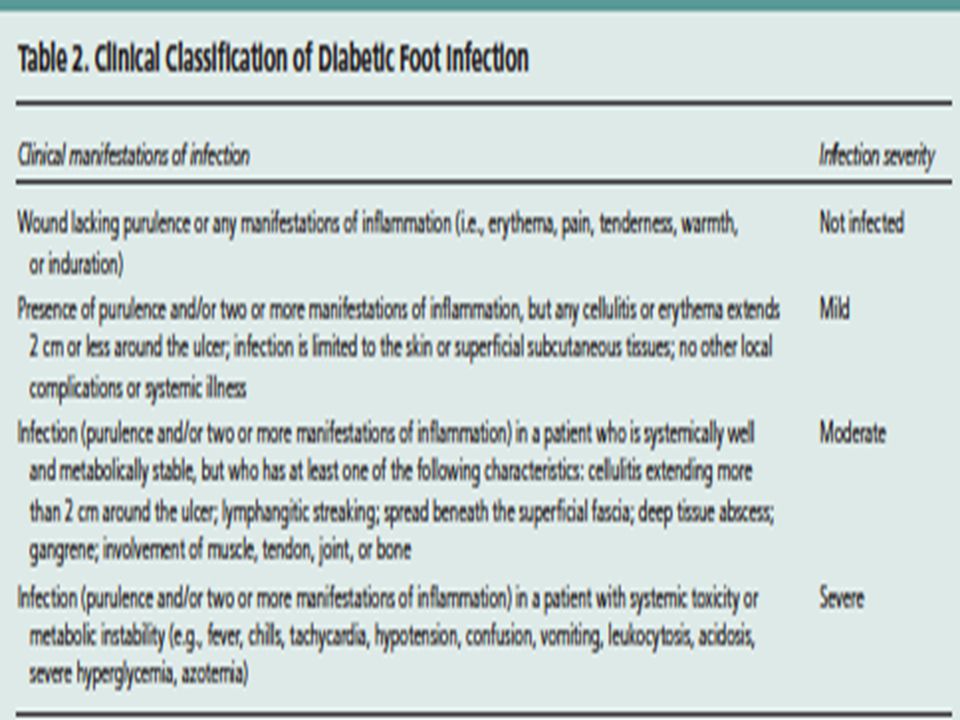
Clinical Evaluation existence, severity, and extent of infection, as well as vascular status, neuropathy, and glycemic control should be assessed in patients with a diabetic foot infection. Visible bone and palpable bone on probing are suggestive of underlying osteomyelitis in patients with a diabetic foot infection. Before an infected wound of a diabetic foot infection is cultured, any overlying necrotic debris should be removed to eliminate surface contamination and to provide more accurate results. Routine wound swabs and cultures of material from sinus tracts are unreliable and strongly discouraged in the management of diabetic foot infection. The empiric antibiotic regimen for diabetic foot infection should always include an agent active against Staphylococcus aureus, including methicillin-resistant S. aureus if necessary, and streptococci.

15
Meggitt–Wagner classification of
foot ulcers Grade Description of the ulcer Grade 0 Pre- or post-ulcerative lesion completely epithelialized Grade 1 Superficial, full thickness ulcer limited to the dermis, not extending to the subcutis Grade 2 Ulcer of the skin extending through the subcutis with exposed tendon or bone and without osteomyelitis or abscess formation Grade 3 Deep ulcers with osteomyelitis or abscess formation Grade 4 Localized gangrene of the toes or the forefoot Grade 5 Foot with extensive gangrene

16
CONFIRMING THE DIAGNOSIS
must be diagnosed clinically rather than bacteriologically The clinical diagnosis of foot infection is basedon Thepresence of purulent discharge from an ulcer or the classic signs of inflammation (i.e., erythema, pain, tenderness, warmth, or induration). Other suggestive features of infection include foul odor, the presence of necrosis, and failure of wound healing despite optimal managment
. Other suggestive features of infection include foul odor, the presence of necrosis, and failure of wound healing despite optimal managment")
22
Arterial inflow is adequate Infection is treated appropriately
Arterial inflow is adequate Infection is treated appropriately. Pressure is removed from the wound and the immediate surrounding area.

Similar presentations



























, also known as simply diabetes, is a group of metabolic diseases in which there are high blood sugar levels.>")
