Download presentation
Presentation is loading. Please wait.

1
Congenital Heart Disease in Children Dr. Sara Mitchell January 31. 2007

2
Changes in circulation at birth Foramen ovale ________ Ductus arteriosis ________ Ductus venous ________ Umbilical vein & artery _________

3
Differences in the pediatric heart Heart rate ______& stroke volume ______ than in adults ______ _______ are normal findings in infants the ______’s thorax is _____-______ the ______'s thorax is ________ by age __ years, the AP:transverse thorax has mature proportions

4
Differences in the pediatric heart ( continued ) The PMI is located at the __th intercostal space in the child younger than __ years of age The apical pulse may be visible
 The PMI is located at the __th intercostal space in the child younger than __ years of age The apical pulse may be visible")
5
Congenital heart disease what's the incidence? ~ 40,000 babies are born each year in the Untied States with congenital heart disease

6
Congenital heart disease what’s the cause? ~90% of congenital heart disease is thought to be due to ___________ ____________

7
Congenital heart disease When in gestation does it occur? Development of the heart and great vessels occurs between the 2nd & 9th week of gestation

8
Congenital heart disease: name the types Lesions with increased pulmonary blood flow Lesions with decreased pulmonary blood flow Mixed circulation defects Obstructive lesions

9
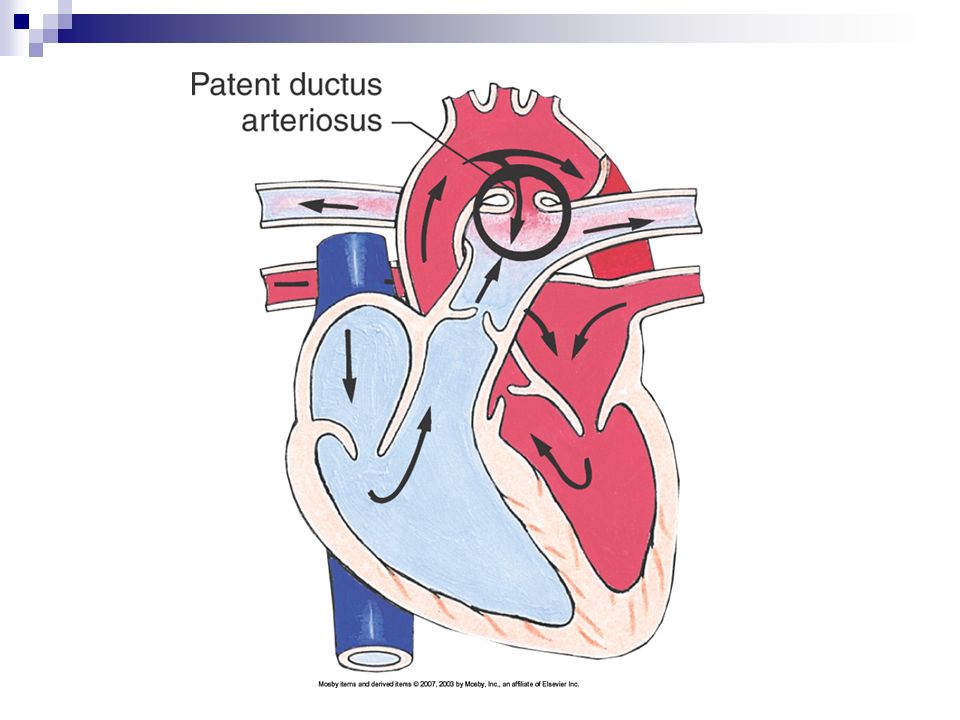
Lesions with ________ pulmonary blood flow: What are they? ______ septal defect (ASD) ______ ductus arterious (PDA) _________ septal defect (VSD) AV canal defect
 ______ ductus arterious (PDA) _________ septal defect (VSD) AV canal defect.")
10
Ventricular Septal Defect

12
Lesions with decreased pulmonary blood flow _________ of _____ ________ atresia _________ atresia Epstein anomaly

13
Tetralogy of Fallot

14
Tricuspid Atresia

15
TET spells – what are they? _____________ spells May occur in any child whose heart defect includes ________ to ________ blood flow and communication between the ventricles

16
TET spells - what do they look like The infant becomes acutely cyanotic because of sudden ________ in pulmonary blood flow and _______ in _______-to-____ shunting. Spells occur more often in the _______ May be preceded by feeding, crying, or defecation.

17
TET spells need to be treated ASAP to prevent _______ ______ with resulting brain damage and possible _______

18
TET spells – what is the management? Place infant in ____- _____ position Employ calm, comforting approach Administer _____% O 2 by face mask Give ________ SQ or IV Begin IV fluid replacement and volume expansion if needed

19
Mixed Circulation defects What are they? ___________ of the great arteries Total anomalous _________ venous connection Trucus Arterious Hypoplastic ______ Heart Syndrome

20
Transposition of the great arteries

21
Truncus Arterious

22
Obstructive cardiac lesions: What are they ? _________ stenosis Aortic stenosis __________ of the Aorta

23
Coarctation of the aorta

24
Pulmonic Stenosis

25
Cardiac Catherization Pre-Op assessment accurate ________ assess & mark _____ _______. baseline ___ explain procedure to child & family

26
Cardiac catheterization (continued) Post-Op assessment be aware of most common complications check pulses ______ cath site check color and temperature of affected extremity check vital signs every 15 minutes (per facility policy). * Be sure to check heart rate for a full 60 seconds **_________________________________________ __________________________________

27
Congestive heart failure Causes of CHF can be classified according to the following changes: Volume overload* Pressure overload* Decreased contractility High cardiac output demands * = most common in children in which structural abnormalities result in an increased volume load or increased pressure load on the ventricles.

28
Therapeutic management of congestive heart failure Two groups of drugs are used to enhance myocardial function in CHF: Digatalis - improves contractility ACE inhibitors - reduce the afterload on the heart making it easier for the heart to pump Diuretics - remove excess fluid

29
Things to know about giving digoxin to infants & children Always check the dosage with a _______ _______ before giving. Count the ______ pulse Monitor for signs & symptoms of toxicity Know what to do if a dose is missed

30
Nursing care plan for a child with congenital heart disease Problem Goal/OutcomeIntervention 1. ________ cardiac output R/T structural defect, myocardial dysfunction. 2. Ineffective breathing pattern R/T _________ _______. 3. Fluid volume excess R/T _____ ________ 4.Activity intolerance R/T___________. 5. Risk for infection R/T reduced body______________. 6. Altered family processes R/T a child with life-threatening illness The child will exhibit 1. Improved _________ 2. Improved respiratory function 3. No evidence of fluid excess 4. The child will experience decreased cardiac demands. 5. The child will maintain adequate nutritional status 6. The child/family will receive adequate support & education Rationale

Similar presentations