Download presentation
Presentation is loading. Please wait.

1
Monitored Anesthesia Care with Dexmedetomidine: A Prospective, Randomized, Double-Blind, Multicenter Trial This study was funded by Hospira Inc. Dr. Keith Candiotti Department of Anesthesiology University of Miami

2
MAC Investigators Martin W. Allard Alex Y. Bekker Sergio D. Bergese Keith A. Candiotti Eric L. Diamond Dennis D. Doblar Thomas J. Ebert Marc Feldmam Robert B. Fisher Tong J. Gan Steven Gayer Ira J. Gottlieb Craig T. Hartrick Gary R. Haynes Fima Lenkovsky Terri Monk Paul A. Moore Thomas N. Pajewski Beverly K. Philip Michael A.E. Ramsay Ruben Ricardo Bernhard Riedel Charles R. Roberson Fred E. Shapiro Jeffrey H. Silverstein Tracey L. Stierer.

3
A 2006 review of closed claims in the ASA Closed Claims Database reveals that oversedation leading to respiratory depression played a major role in patient injuries during MAC.A 2006 review of closed claims in the ASA Closed Claims Database reveals that oversedation leading to respiratory depression played a major role in patient injuries during MAC. MAC claims were fewer than GA overallMAC claims were fewer than GA overall Claims for death or permanent brain damage were 40%, similar to GA 1Claims for death or permanent brain damage were 40%, similar to GA 1 1 Bhananker SM et al. Anesthesiology 2006;104:228-34.

4
Most commonly used drugs are midazolam, propofol and fentanyl.Most commonly used drugs are midazolam, propofol and fentanyl. All 3 of these drugs is known to cause respiratory depression-especially in combination.All 3 of these drugs is known to cause respiratory depression-especially in combination. 1 Bhananker SM et al. Anesthesiology 2006;104:228-34.

5
DEX is a centrally acting alpha-2 receptor antagonist that does not produce significant respiratory depression. 1-3DEX is a centrally acting alpha-2 receptor antagonist that does not produce significant respiratory depression. 1-3 Dex has an analgesic-sparing effect, reducing opioid requirements both during and after surgery. 3Dex has an analgesic-sparing effect, reducing opioid requirements both during and after surgery. 3 The agent also possess a sympatholytic effect that can mitigate tachycardia and HTN. 3The agent also possess a sympatholytic effect that can mitigate tachycardia and HTN. 3 1 Ebert TJ et al. Anesthesiology 2000;93:382-94. 2 Venn RM et al. Crit Care 2000;4:302-8. 3 Arain SR et al. AA 2002;95:461-6

6
DEX is currently approved for use in initially intubated patients in an intensive care setting.DEX is currently approved for use in initially intubated patients in an intensive care setting. This trial was designed to evaluate the safety and efficacy of DEX in non-intubated patients in a large multicenter trial (26 sites) using it as the primary sedative agent.This trial was designed to evaluate the safety and efficacy of DEX in non-intubated patients in a large multicenter trial (26 sites) using it as the primary sedative agent. FDA trial designed to compare against a placebo group using midazolam and fentanyl for rescue.FDA trial designed to compare against a placebo group using midazolam and fentanyl for rescue.
 using it as the primary sedative agent.This trial was designed to evaluate the safety and efficacy of DEX in non-intubated patients in a large multicenter trial (26 sites) using it as the primary sedative agent. FDA trial designed to compare against a placebo group using midazolam and fentanyl for rescue.FDA trial designed to compare against a placebo group using midazolam and fentanyl for rescue..")
7
Study Design Randomized 2:2:1Randomized 2:2:1 LOADLOAD –DEX 0.5 mcg/kg load –DEX 1 mcg/kg load –Saline Placebo MAINTENANCEMAINTENANCE –Both DEX groups 0.6 mcg/kg/hr (titrated) –Placebo had saline infusion
 –Placebo had saline infusion")
8
DEX 130 Load Maintenance DEX 0.5 mg/kg 10 min DEX 130 PBO 65 DEX 1 mcg/kg 10 min 0.6 mcg/kg/hr titrate 0.6 mcg/kg/hr titrate PBO 10 min PBO Infusion Midazolam/Fentanyl Rescue

9
Observer’s Assessment of Alertness/Sedation Scale used (OAA/S) 5=responds to name spoken in normal tone 4=responds only after mild prodding or shaking 3=responds only after name loudly and/or repeatedly 2=lethargic response to name spoken in normal tone 1=does not respond to mild prodding or shaking
 5=responds to name spoken in normal tone 4=responds only after mild prodding or shaking 3=responds only after name loudly and/or repeatedly 2=lethargic response to name spoken in normal tone 1=does not respond to mild prodding or shaking")
10
Study drug started at least 15 min prior to block or local anestheticStudy drug started at least 15 min prior to block or local anesthetic Midazolam 0.5 mg doses given for OAA/S>4Midazolam 0.5 mg doses given for OAA/S>4 Fentanyl was given for painFentanyl was given for pain

11
Primary endpointPrimary endpoint –% patients not requiring midazolam for rescue based on an OAA/S of ≤ 4. Secondary endpointSecondary endpoint –Total rescue midazolam and/or fentanyl –Time to rescue –Patients who converted to alternative therapy –Readiness for D/C –Hemodynamic stability –Patient and Anesthesiologist Satisfaction Safety endpointsSafety endpoints –Cardiac and pulmonary etc.

12
326 in intent-to-treat326 in intent-to-treat Randomization was goodRandomization was good Fewer patients in both DEX groups required midazolam and used less (p< 0.001)Fewer patients in both DEX groups required midazolam and used less (p< 0.001) Both DEX groups required less fentanyl (p< 0.01)Both DEX groups required less fentanyl (p< 0.01)
Fewer patients in both DEX groups required midazolam and used less (p< 0.001) Both DEX groups required less fentanyl (p< 0.01)Both DEX groups required less fentanyl (p< 0.01)")
13
Groups vs. PBO (p< 0.001) Mean 1.4 mg Mean 0.9 mg Mean 4.1 mg
 Mean 1.4 mg Mean 0.9 mg Mean 4.1 mg")
15
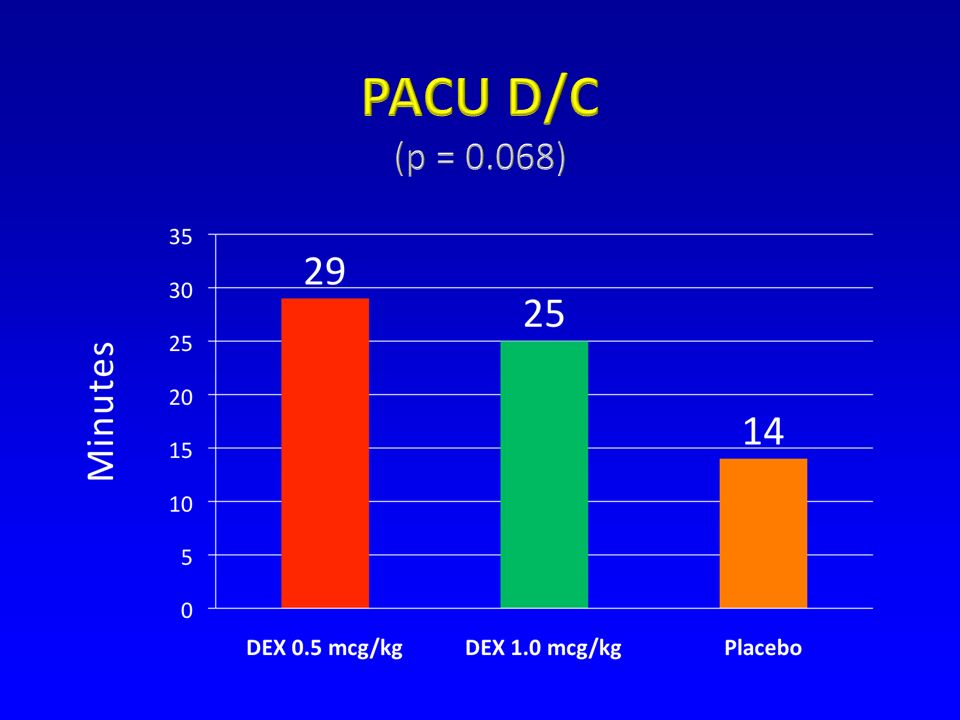
Anesthesiologists indicated that DEX was easier to control than PBO + midazolam (p<0.009)Anesthesiologists indicated that DEX was easier to control than PBO + midazolam (p<0.009) PBO required more fentanyl in PACU than DEX 1 mcg load group (p≤0.068)PBO required more fentanyl in PACU than DEX 1 mcg load group (p≤0.068) Patient satisfaction was higher with DEX (p<0.009)Patient satisfaction was higher with DEX (p<0.009)
Anesthesiologists indicated that DEX was easier to control than PBO + midazolam (p<0.009) PBO required more fentanyl in PACU than DEX 1 mcg load group (p≤0.068)PBO required more fentanyl in PACU than DEX 1 mcg load group (p≤0.068) Patient satisfaction was higher with DEX (p<0.009)Patient satisfaction was higher with DEX (p<0.009)")
16
Most common AE with DEX were protocol defined bradycardia and hypotension which were predominately mild to moderate in severity and did not require intervention.Most common AE with DEX were protocol defined bradycardia and hypotension which were predominately mild to moderate in severity and did not require intervention. Mean decrease in SBP (p≤0.043) and DBP (p<0.001) was greater in DEX than PBO group.Mean decrease in SBP (p≤0.043) and DBP (p<0.001) was greater in DEX than PBO group.
 and DBP (p<0.001) was greater in DEX than PBO group.Mean decrease in SBP (p≤0.043) and DBP (p<0.001) was greater in DEX than PBO group..")
17
HR decrease in both DEX groups was significant from baseline and vs. PBO group (p<0.001)HR decrease in both DEX groups was significant from baseline and vs. PBO group (p<0.001) Incidence of significant respiratory depression (RR < 8 or O2 Sat% < 90%) was lower in DEX treated patients (p=0.018)Incidence of significant respiratory depression (RR < 8 or O2 Sat% < 90%) was lower in DEX treated patients (p=0.018)
HR decrease in both DEX groups was significant from baseline and vs. PBO group (p<0.001) Incidence of significant respiratory depression (RR < 8 or O2 Sat% < 90%) was lower in DEX treated patients (p=0.018)Incidence of significant respiratory depression (RR < 8 or O2 Sat% < 90%) was lower in DEX treated patients (p=0.018).")
20
Coadministration of midazolam or fentanyl with DEX was not associated with an increase in hypotension, bradycardia or respiratory depression.Coadministration of midazolam or fentanyl with DEX was not associated with an increase in hypotension, bradycardia or respiratory depression. In PBO group midazolam and fentanyl were associated with a respective 13.1 and 16.1% rate absolute respiratory depression or need for intervention.In PBO group midazolam and fentanyl were associated with a respective 13.1 and 16.1% rate absolute respiratory depression or need for intervention.

21
DEX is an effective baseline sedative for patients undergoing MAC for a variety of procedures.DEX is an effective baseline sedative for patients undergoing MAC for a variety of procedures. Less opioids are required and less respiratory depression is seen with DEX.Less opioids are required and less respiratory depression is seen with DEX.

22
FDA decision based on this trial:FDA decision based on this trial: “This supplemental new drug application provides for the use of Precedex Injection for sedation of nonintubated patients prior to and/or during surgical and other procedures”. “This supplemental new drug application provides for the use of Precedex Injection for sedation of nonintubated patients prior to and/or during surgical and other procedures”.

Similar presentations



 GORDONR. BERNARD, M.D. et al. The New England Journal of Medicine.>")


 and Inpatient (Study 2) Settings Study.>")














