Download presentation
Presentation is loading. Please wait.

1
SUPRA-NATIONAL REFERENCE LABORATORY NETWORK Possible research projects A. Van Deun

2
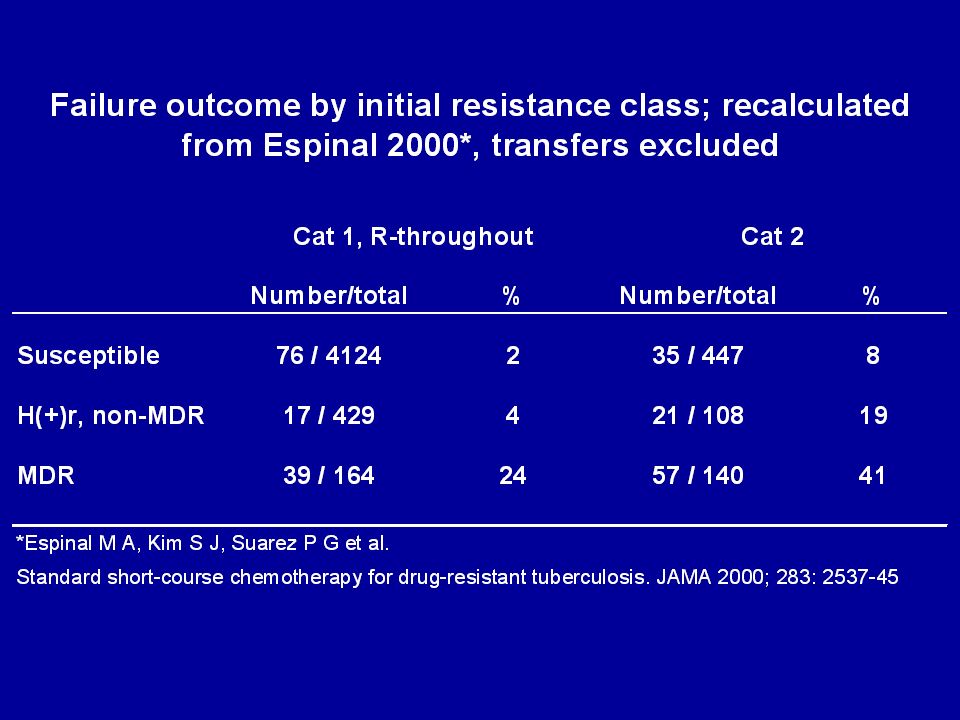
1. RELEVANCE OF BORDERLINE R-RESISTANCE Background: SRL rounds –too many discordant strains in Rounds –all with documented Rr-conferring mutation –WT fraction not visible by sequencing, so hetero- resistance or mixture cannot explain the discordance? Background: clinical experience –poor results Cat. 2 retreatment after 6-months R Cat. 1 –far more failures within same (non-MDR) resistance- group than with weaker Cat 1 low-level Rr missed in retreatment cases??
 resistance- group than with weaker Cat 1 low-level Rr missed in retreatment cases .")
4
STUDY OUTLINE Testing R at 20 and 40 µg/ml (or corresponding) –recommended in Canetti 1969 proportion method ref. paper –MIC 30-40 for +/- 10% probably R-resistant at coordinating lab document frequency R20r/R40s Use QA strains from random sampling surveys –request all retreatment strains for QA, including susc. –also collect outcome of treatment information (including relapse) All strains for monitoring of resistance in retreatment strains (and DOTS-Plus) –if randomly sampled –i.e. systematic FU of Cat 1 / Cat 2 retreatments in SRL in HBC
 All strains for monitoring of resistance in retreatment strains (and DOTS-Plus) –if randomly sampled –i.e. systematic FU of Cat 1 / Cat 2 retreatments in SRL in HBC.")
5
ACCURACY OF GENOTYPIC DST FOR R Background: –literature: about 95% correlation –discordants: no mutation but phenotypic Rr –however: too few phenoypic R-susceptible checked in these studies clinical significance of pheno-Rr / geno Rs ??

6
STUDY OUTLINE Combine with first proposal on discordants Same group of strains – random and representative samples from retreatment cases Do also rpoB sequencing (or hybridisation) –cluster 1 or extended? –document outcome of standard treatment !! but MDR-TB treatment would interfere so only projects without DOTS-Plus in place?

7
RELEVANCE OF E-TESTING Background –high error-rates, lower reproducibility, discordance between systems (LJ versus BACTEC/MGIT) –interpretation problems: potency adjustment or not? microcolonies (at 4 weeks? at 6 weeks?) –significance?? Er but still synergistic with amoxy-clavulanic in vitro replacement by cycloserin in MDR-regimens –not done in standardised regimen in Bangladesh cured : 98/122 (80%) of cured have HRE(S) resistant strain versus 7/9 (78%) of the failures
 –significance . Er but still synergistic with amoxy-clavulanic in vitro replacement by cycloserin in MDR-regimens –not done in standardised regimen in Bangladesh cured : 98/122 (80%) of cured have HRE(S) resistant strain versus 7/9 (78%) of the failures.")
8
STUDY OUTLINE Study populations from DRS surveys –meta-analysis, lump surveys together? –only Cat 1 : 2EHRZ/6HE –failure / relapse (F/R) outcome initally H(S)r versus initially H(S)Er stratify for exact critical concentration (E-potency adjustment!); and method? –if possible: compare also acquired Rr in F/R strains, same arms (cf. Vietnam experience with 2SHRZ/6HE failures: 40% ADR to R)
 outcome initally H(S)r versus initially H(S)Er stratify for exact critical concentration (E-potency adjustment!); and method. –if possible: compare also acquired Rr in F/R strains, same arms (cf. Vietnam experience with 2SHRZ/6HE failures: 40% ADR to R).")
9
KANAMYCIN / ETHIONAMIDE / OFLOXACIN Background –may be more important in panel than E and S (DOTS-Plus) –but not well standardised for LJ –and clinical significance less known K resistance level and amikacin activity ? O resistance level and moxi, gati activity ? ETH / INH cross-resistance clinical relevance?

10
STUDY PROPOSAL Standardise K, O and ethionamide for LJ proportion method / other systems? Document MIC values and determine critical concentrations –K, Ethion: outcome of MDR-TB standard regimen including K, thioamide (and quinolone susceptible) –O: outcome of MDR-TB standard regimen including moxi or gati (and other second-line susceptible)
 –O: outcome of MDR-TB standard regimen including moxi or gati (and other second-line susceptible).")
Similar presentations